About half of all adults snore occasionally, and about a quarter snore regularly. While it’s sort of a funny topic, and often joked about in sitcoms, snoring can cause real issues in the bedroom. Whether it’s keeping you from getting the deep, restful sleep you need, or waking up your spouse at all hours (if they can get to sleep at all), snoring can create a boatload of tension. It’s worth your physical and relational health to try to get a handle on your noisy nighttime muffler.
Snoring is more common in men than women, and tends to get worse as one ages and/or gains weight. It happens when the free flow of air from the mouth/nose to the lungs is interrupted and vibration at the back of the throat occurs, for a variety of reasons: congestion, illness, poor muscle tone in the mouth/jaw, and a few more serious health concerns.
For most folks, there are natural remedies that can reduce and even eliminate their snoring. For others, however, it can be a sign of some form of sleep apnea, wherein your breathing temporarily pauses in the night, causing you to snore loudly and even occasionally jolt yourself awake. Less than 5% of people are diagnosed with sleep apnea, but it’s estimated that up to 80% of sufferers are undiagnosed.
If you try the below steps and don’t see any improvement in your snoring, it’s best to seek out a medical professional. Do not buy mouth guards or anti-snore devices without medical consultation, even from your dentist — any device going in the mouth can have an effect on your teeth and general oral well-being.
First, though, try the advice below. Odds are good that you’ll see at least some improvement, if not a total cessation of your snoring problems.
1. Lose a few pounds.
That turkey wattle you get during the holidays is hurting more than just your appearance. As weight increases, so does the prevalence of snoring. Extra poundage just generally compresses things and closes your airways more than they would be otherwise. You actually accumulate fatty tissue in the neck and back of the throat, and that tissue is “floppy” — rather than being rigid like muscle. It therefore vibrates when breathing deeply in and out during sleep.
In many people, the neck is one of the areas of the body that both loses and gains weight quickly. That’s both a positive and a negative; just a few pounds off the scale should help you out, but just a few pounds added back on and you may be in trouble again. Among the numerous benefits that come with weight loss, a decrease in snoring is likely one, and may provide some extra motivation.
2. Change your sleep position.
Lying on your back can cause your tongue and soft palate to fall back into your throat and partially block your airways, leading to snoring. Try sleeping on your side instead; memory foam mattresses help with this, as does a body pillow if you’re having a hard time adjusting.
3. Avoid alcohol.
Booze can make people snore who don’t normally do so. Beyond just stuffing you up, as beer and other alcoholic beverages can often do, alcohol relaxes the muscles too much, leading to fluttering and vibrating while sleeping. Not only will abstaining from alcohol for the 3-4 hours before bedtime just generally improve your sleep cycle, it’ll also curb your snoring. It’s a hard thing to do, especially with socializing at night, but keep it in mind if snoring is giving you or your loved one real problems.
4. Get enough sleep.
5. Keep nasal passages open.
Nasal congestion is a major cause of snoring; this is why someone who’s typically a non-snorer will become a nighttime rhino when he’s sick. If you have a cold, or are just naturally regularly congested, try taking a hot shower before bed (showers are better than baths because of the steam that circulates when in an enclosed space), or use a neti pot. Nasal strips are also worth trying.
6. Keep your room clean!
Allergens and dust can be a cause of snoring. Regularly dust your bedroom, including your ceiling fan if you have one. Wash your bedding regularly (you shouldn’t need a reminder on that one!). Vacuum often, including the curtains. Get your air ducts cleaned every couple years. Also don’t allow pets to sleep on the bed if you have snoring problems.
7. Stay hydrated.
Dry mouths lead to dry noses and throats. This can lead to build-ups of gunk and general irritation and swelling, leading to congestion and blockage. Drink plenty of water, help your snoring.
8. Keep your mouth, jaw, and throat muscles toned.
Research shows that doing daily mouth and jaw-strengthening exercises over the course of a few months reduces snoring occurrences by more than a third, and reduces snoring intensity by up to 60%.
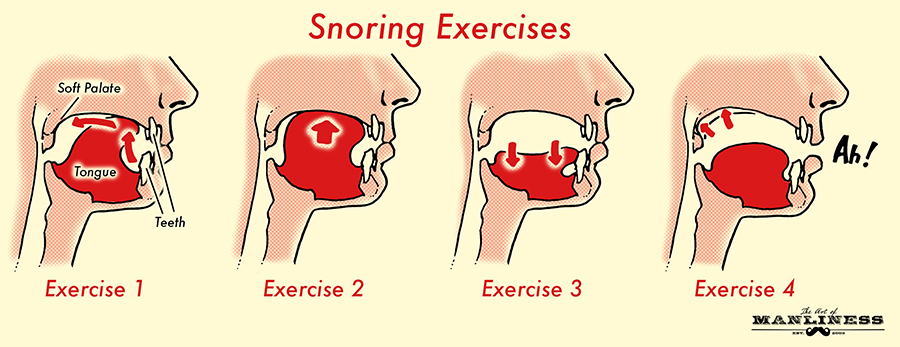
Consumer Reports recommends this daily routine; each exercise is performed 20 times a day:
- Exercise 1: Push the tip of the tongue against the roof of the mouth and slide the tongue backward.
- Exercise 2: Suck the tongue upward against the roof of the mouth and press the entire tongue against the roof of the mouth.
- Exercise 3: Force the back of the tongue against the floor of the mouth while keeping the tip of the tongue in contact with the bottom front teeth.
- Exercise 4: Elevate the soft palate (the back of the roof of the mouth) and the uvula (the fleshy protrusion that hangs from the soft palate) while making the vowel sound “Ah.”
These exercises give your mouth and jaw muscles more rigidity, making it less likely they’ll vibrate when breathing at night.
9. Avoid smoking.
Smoking irritates membranes in the nose and throat, inflaming them and causing congestion and blocked airways. As with losing weight, there are numerous benefits to quitting smoking, with decreased snoring being but one.
10. Elevate.
You can use pillows to elevate your head, but be sure you’re not doing it just at the head; elevate your chest some as well. Otherwise you can make your neck crink, giving you both pain and airway blockage that you didn’t bargain for. You can get a mattress that raises up and down, but those are rather expensive. Go the DIY route by putting a few books under your mattress, or under the legs of the bed. Even just being elevated a few inches can help things out.
11. Use a humidifier.
Dry air can irritate the nose and throat, making them swollen, and therefore causing congestion, and snoring in turn. Use a humidifier at night to open things up a bit more.
12. Ask your doc about medications.
Sleep aids and sedatives relax your muscles, making it more likely that they’ll vibrate at night, causing you to snore. Many people rely on sleep aids though, so ask your doctor about it. Other medications can do the same thing and also contribute to snoring. If you’re having real problems, ask your doc about how your prescriptions might be impacting your sleep and your snoring, and what you might be able to do about it.