Moderna is hard at work ramping up production of its mRNA COVID-19 vaccine, which is projected to reap over $19 billion for the company by year’s end. But given that the pandemic is easing in parts of the world, what’s less certain is how 2022 will play out.
After a breakout year, Moderna sees strong reason to believe 2021 won't be a one-off boom year. That's thanks to the predicted need for booster shots and additional supply deals coupled with stronger pricing power, Jefferies analysts wrote to clients Thursday following a conversation with CEO Stéphane Bancel.
The Jefferies team thinks Moderna could drive $15 billion in 2022 revenues, with an upper limit of $30 billion. Where the company lands will depend on how the pandemic progresses, fear of infection and whether the company can produce future products, like a combo shot against COVID and the flu.
Plus, it’s possible that Moderna could start charging more per dose given its high efficacy, reliable manufacturing and absence of serious side effects that have plagued other vaccine developers, the analysts said.
Moderna has said it can churn out between 800 million to 1 billion doses this year, and about 3 billion by 2022. The company has been ramping up supply lines with CDMO heavyweights and is planning a massive expansion at its own U.S.-based facilities to meet its lofty supply expectations.
With more doses coming down the line, Moderna is already engaging with countries who weren’t able to secure supply this year, as well as with those that previously ordered adenovirus shots, Jefferies analysts wrote.
And discussions are ongoing with nations that already have supply deals, given that many have yet to begin inoculating children. The company’s shot has been used in people ages 18 and older, although the company is working to expand its use to those as young as 12, including in the U.S.
The Cambridge, Massachusetts-based biotech is also developing three potential booster shots to target troublesome virus variants, including a lower dose of its original vaccine, one developed to target the variant first found in South Africa, and a combination of the two.
It’s thought that some countries will “want to ensure there are adequate orders” for booster shots as early as six months to a year after the first vaccines were administered, the Jefferies team said.
Pandemic shots aren’t the only sales prospects Moderna has in its back pocket, Jefferies said. The mRNA developer is also working on a shot for seasonal influenza, with initial results anticipated by the end of the year.
Early Alzheimer's disease progressed with high variability and this may influence whether treatment effects truly are detected in clinical trials, a simulation study suggested.
Individual trajectories on commonly used cognitive measures -- the Mini-Mental State Examination (MMSE), the Clinical Dementia Rating Sum of Boxes (CDR-SB), and the Alzheimer's Disease Assessment Scale Cognitive (ADAS-cog) -- differed greatly among individuals with prodromal and mild Alzheimer's, even among seemingly homogenous groups, reported Roos Jutten, PhD, of Amsterdam UMC in the Netherlands, and co-authors.
As a result, the 95% range of group differences observed on cognitive measures over 18 months was broad, spanning from 0.35 points improvement to 0.35 points decline on the CDR-SB, for example, they wrote in Neurology.
"Alzheimer's disease patients show substantial variation in how fast or slow their cognitive functions decline over time," Jutten told MedPage Today. "This heterogeneity in disease progression is a problem for clinical trials, which want to show that a drug or treatment can slow or halt cognitive decline."
"We investigated how natural variability in disease progression may lead to significant group differences that are not due to the therapy administered, but instead reflect patient differences in their rate of decline," she said.
"We also studied ways to reduce variability in rates of decline, by looking only at subgroups that had increased risk for fast progression, such as APOE4 carriers," Jutten continued. "An unexpected outcome of our study is it is even more difficult to find treatment effects in these high-risk groups, because they show more within-group variability in decline instead of less."
The findings highlight an important challenge of trial design, noted Rachel Buckley, PhD, of Massachusetts General Hospital in Boston, and David Knopman, MD, of Mayo Clinic in Rochester, Minnesota, in an accompanying editorial.
"In the absence of a widely accepted therapeutic success threshold to serve as a starting point, what is a minimal therapeutic benefit that is clinically meaningful?" Buckley and Knopman asked.
"Clinical meaningfulness has been an elusive concept in the world of Alzheimer's disease therapeutics," they added. "The description by Jutten et al. of the 95% confidence interval for random variation in slope of several widely used outcome measures provides a rational estimate of a floor for what clinically meaningful therapeutic benefit should look like."
In their study, Jutten and co-authors identified 302 participants from the Alzheimer's Disease Neuroimaging Initiative (ADNI) with an abnormal amyloid PET scan, diagnosis of mild cognitive impairment or dementia, baseline MMSE score of 24 or higher, global Clinical Dementia Rating score of 0.5, and at least one follow-up cognitive assessment. These were the baseline characteristics of the aducanumab EMERGE and ENGAGE trials, they noted.
Mean age of the sample was 73, 44% were women, mean education was 16.1 years, and 69% were APOE4 carriers.
The researchers simulated a clinical trial by randomly assigning individuals to "placebo" and "treatment" groups (even though no treatment was actually given), using longitudinal cognitive data to estimate change from baseline over 18 months. This gave them the variability in effect sizes between a placebo and treatment group if heterogeneity in progression wasn't accounted for. They repeated this simulation 10,000 times to determine the 95% range of effect sizes.
They compared this to effect sizes that have been reported for recent trials of several anti-amyloid drugs with similar inclusion criteria and found that, with the exception of the aducanumab EMERGE trial, the treatment effects fell within the 95% boundaries -- in other words, within the range that could be expected if there were no treatment effect.
"This suggests that, even though within some trials, differences between placebo and treatment groups were statistically significant, the possibility cannot be excluded that those differences were actually due to oversampling of fast decliners in the placebo group or oversampling of slow decliners in the treated group," Jutten and co-authors wrote.
We further showed that, when repeating our simulation for separate risk factors associated with disease progression, a positive APOE4 status and baseline abnormal total tau levels were associated with steeper cognitive decline at a group level, but also with greater variability in progression," they added. "This resulted in even broader ranges of effect sizes in these high-risk groups on all outcome measures (e.g., ±0.70 points for the CDR-SB in those with baseline abnormal tau)."
A run-in period that captures an individual's cognitive trajectory, using biomarkers as primary endpoints, or larger sample sizes may solve the problem, but these solutions have limitations.
"Overly large sample sizes invite the prospect of detecting therapeutic effects that are statistically significant but clinically trivial," Buckley and Knopman noted. "While designing a better outcome measure using criteria to exclude persons who are not likely to decline or using other strategies to minimize measurement error, therapeutics with larger effect sizes are what the field ultimately needs."
The study had several limitations, Jutten and colleagues acknowledged. The simulation was based on ADNI participants, a relatively highly educated sample with little racial and ethnic diversity. Some participants in ADNI had 6-month follow-up data, which may have led to less decline and less variability in change over time. Selection criteria and follow-up timeframe were based on the aducanumab EMERGE and ENGAGE studies, and there may be small differences with criteria used in other trials.
Disclosures
Alzheimer Center Amsterdam, Amsterdam UMC is supported by Alzheimer Nederland and Stichting VUmc funds.
Data collection and sharing for this project was funded by the Alzheimer's Disease Neuroimaging Initiative (ADNI), which receives support from the National Institutes of Health and Department of Defense.
The researchers reported no disclosures relevant to this manuscript.
Buckley reported no disclosures relevant to the manuscript. Knopman serves on a Data Safety Monitoring Board for the Dominantly Inherited Alzheimer Network study. He also serves on a Data Safety Monitoring Board for Biogen but receives no personal compensation. He is an investigator in clinical trials sponsored by Biogen, Lilly Pharmaceuticals, and the University of Southern California. He serves as a consultant for Roche, Samus Therapeutics, Third Rock, and Alzeca Biosciences but receives no personal compensation.
Argentinean Ambassador to Russia Eduardo Zuain said on Friday that his country is keeping its plans to start large-scale production of the Sputnik V vaccine in July.
The Nikolai Gamaleya National Research Center, the developer of the vaccine, confirmed on Tuesday the high quality of the batch prepared by the Argentinean laboratory as a test and sent for review in Russia.
The Argentinean representative in Moscow told Sputnik news agency at the International Economic Forum in Saint Petersburg (Spief 2021) that the next stage will be the import of antigens, a step to be taken in the near future.
Zuain stressed that despite the pandemic, Argentina and Russia are now experiencing 'an excellent time in bilateral relations' and highly valued the cooperation between the two states in the fight against Covid-19.
In this regard, he underscored the supply of the Sputnik V vaccine to Argentina, as well as the transfer of Russian technology for its manufacture.
Zuain recalled that he is not only interested in manufacturing the Russian vaccine for its use in Argentina, but also to export it to Latin America.
LUMAKRAS Shows Median Overall Survival of 12.5 Months in Patients With Previously Treated Non-Small Cell Lung Cancer
Data Confirms Rapid, Deep, and Durable Responses With Median Duration of Response of 11.1 Months
Data Presented at ASCO 2021 and Simultaneously Published in New England Journal of Medicine
Amgen (NASDAQ: AMGN) today presented data on overall survival, a secondary endpoint, from the Phase 2 results of the CodeBreaK 100 clinical study for LUMAKRASTM (sotorasib) in previously treated patients with non-small cell lung cancer (NSCLC) during the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting. These data were also simultaneously published in the New England Journal of Medicine (NEJM). The publication includes mature overall survival and duration of response data, and results from subgroup and exploratory biomarker analyses.
LUMAKRAS shows a median overall survival (OS) of 12.5 months among 124 evaluable patients, the majority of which were previously treated with both platinum-based chemotherapy and immunotherapy (81%) (data cutoff of March 15, 2021). The results confirmed an objective response rate (ORR) of 37.1%, duration of response (DoR) of 11.1 months and disease control rate (DCR) of 80.6%, with an additional patient achieving complete response (bringing the total to four complete responses and 42 partial responses) compared to previously reported results. The data published in NEJM are updated from results presented at the International Association for the Study of Lung Cancer (IASLC) 2020 World Conference on Lung Cancer (WCLC) held in January 2021 and are based on a longer follow-up time of 15.3 months.
"Patients with KRAS G12C-mutated non-small cell lung cancer face poor outcomes so we are pleased with these overall survival results and the impact LUMAKRAS may have for patients with this devastating mutation," said David M. Reese, M.D., executive vice president of Research and Development at Amgen. "The results published in the New England Journal of Medicine further confirm the deep and durable responses we have seen with LUMAKRAS throughout the CodeBreaK clinical trial program, the most advanced KRAS G12C clinical trial program with the longest follow-up."
Revered scientific journal The Lancet has created a ‘task force’ to investigate the origins of the coronavirus that caused a global pandemic, yet it has decided to employ as it’s leader the very guy who funded the dangerous gain of function research at the Wuhan lab and subsequently allegedly ‘bullied’ other scientists into avoiding looking into the lab as a potential source of the outbreak.
In the wake of renewed scrutiny of the lab leak hypothesis, the Lancet’s task force will reportedly “focus on analyzing data on all of the theories put forward on the origins of COVID, on the reasons why SARS-CoV-2 was able to break out of Wuhan and spread globally, and on the most plausible strategies to prevent future pandemics.”
It also states that “The Task Force will review thoroughly and objectively all publicly available evidence, particularly the peer-reviewed literature, and conduct interviews with key leaders in science, medicine, policy and civil society.”
‘Objectively’. Right.
Dr Peter Daszak, who is heading up this task force, is perhaps the least suitable scientist on the planet to objectively analyse the data, given his track record.
Daszak, as President of the EcoHealth Alliance, shovelled at least $600,000 to the Wuhan Institute of Virology in the past few years to play around with coronaviruses inside the lab through the now infamous ‘gain of function’ research.
Daszak, who also works for the World Health Organisation, is on record admitting that he was involved with manipulating coronaviruses. Here is a video of him talking in DECEMBER 2019 about how ‘good’ the viruses are for altering in a lab:
Daszak notes that “coronaviruses are pretty good… you can manipulate them in the lab pretty easily… the spiked proteins drive a lot about what happens. You can get the sequence you can build the protein, we work with Ralph Baric at UNC to do this, insert into the backbone of another virus and do some work in a lab.”
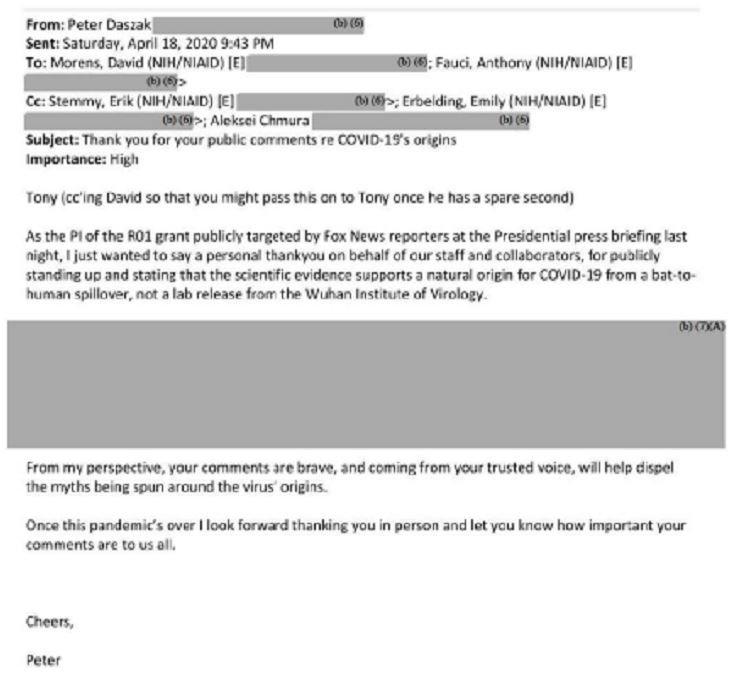
Recently released emails now document that Daszak thanked Dr Fauci for dismissing the lab leak theory before any scientific research had been done on the possibility.
Daszak’s Twitter profile is basically one long ‘it came from bats not a lab’ thread, much to the annoyance of some other scientists:
Why does this guy keep getting put in charge of investigations, task forces and ‘fact checking’, when it’s abundantly clear that he has the biggest motive to dismiss the lab leak notion?
As microbiologist Professor Richard Ebright has noted, “Daszak was the contractor who funded the laboratory at the Wuhan Institute of Virology that potentially was the source of the virus with subcontracts from $200million [£142million] from the US Department of State and $7million [£5million] from the US National Institutes of Health and he was a collaborator and co-author on research projects at the laboratory.”
Daszak has already lied about the type of research that was being conducted at the Wuhan lab, claiming, after the outbreak happened, that he didn’t know if it was gain of function or not. His own previous statements, and the Fauci emails prove he knew full well what was going on in the lab.
In addition, as reported by The Daily Mail and other outlets, Daszak “orchestrated a ‘bullying’ campaign and coerced top scientists into signing off on a letter to The Lancet aimed at removing blame for Covid-19 from the Wuhan lab he was funding with US money.”
Daszak used his influence to get the journal to publish the letter, which stated that to even suggest the lab leak theory had any credibility was equal to spreading “fear, rumours, and prejudice.”
It effectively shut down discussion among the scientific ‘consensus’ of the lab leak potential for a whole year until intelligence findings brought the matter back to the attention of the mainstream media.
WHO scientific advisor Jamie Metzl described Daszak’s letter as “scientific propaganda and a form of thuggery and intimidation.”
“By labelling anyone with different views a conspiracy theorist, the Lancet letter was the worst form of bullying in full contravention of the scientific method,” Metzl added.
The letter further stated that “We stand together to strongly condemn conspiracy theories suggesting that Covid-19 does not have a natural origin,” and even had the audacity to state that “We declare no competing interests.”
Indeed, Daszak had made sure that the letter would be devoid of any link to EcoHealth, and even considered leaving his own name off it, emails released via the Freedom of Information Act have revealed.
To make matters worse, the other members of The Lancet’s task force are practically all minions of Daszak, some of whom helped him draft the letter that unequivocally stated the lab leak theory was dangerous, and others who either worked with him on ‘fact checking’ for Facebook, or were cited as sources during that activity.
Taking all this into account, it is obvious what the outcome of The Lancet’s inquiry will be, and it should not and cannot be used as credible evidence against the lab leak theory.
Presentation available on demand as part of 2021 American Society of Clinical Oncology (ASCO) Annual Meeting
Incyte (NASDAQ:INCY) and MorphoSys US Inc., a fully owned subsidiary of MorphoSys AG (FSE: MOR; NASDAQ:MOR), today announced new three-year follow-up data from the ongoing Phase 2 L-MIND study of tafasitamab (Monjuvi®) in combination with lenalidomide in adult patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL). A total of 80 out of 81 enrolled study patients receiving tafasitamab plus lenalidomide were included in the efficacy analysis at approximately three years follow-up (≥35 months)1.The long-term analysis, as assessed by an independent review committee (IRC), showed that patients treated with tafasitamab plus lenalidomide had an overall response rate (ORR) of 57.5% (95% CI = 45.9, 68.5; 46 out of 80 patients), including a complete response (CR) rate of 40% (32 out of 80 patients). Additionally, the median duration of response (DoR) was 43.9 months (95% CI = 26.1, Not Reached [NR]), with a median overall survival (OS) of 33.5 months (95% CI = 18.3, NR) and median progression free survival (PFS) of 11.6 months (95% CI = 6.3, 45.7).
Regulators on Friday said a new version of a popular diabetes medicine could be sold as a weight-loss drug in the U.S.
The Food and Drug Administration approved Wegovy, a higher-dose version of Novo Nordisk’s diabetes drug semaglutide.
In company-funded studies, participants taking Wegovy had average weight loss of 15%, about 34 pounds (15.3 kilograms). Participants lost weight steadily for 16 months before plateauing. In a comparison group getting dummy shots, the average weight loss was about 2.5%, or just under 6 pounds.
“With existing drugs, you’re going to get maybe 5% to 10% weight reduction, sometimes not even that,” said Dr. Harold Bays, medical director of the Louisville Metabolic and Atherosclerosis Research Center. Bays, who is also the Obesity Medicine Association’s chief science officer, helped run studies of Wegovy and other obesity and diabetes drugs.
In the U.S., more than 100 million adults — about one in three — are obese.
Dropping even 5% of one’s weight can bring health benefits, such as improved energy, blood pressure, blood sugar and cholesterol levels, but it often doesn’t satisfy patients who are focused on weight loss, Bays said.
Bays said Wegovy appears far safer than earlier obesity drugs that “have gone down in flames” over safety problems. Wegovy’s most common side effects were nausea, diarrhea and vomiting. Those usually subsided, but led about 5% of study participants to stop taking it.
The drug also shouldn’t be given to people at risk for some cancers, because of a potential risk for certain thyroid tumors, the FDA said.
Patients inject Wegovy (pronounced wee-GOH’-vee) weekly under their skin. Like other weight-loss drugs, it’s to be used along with exercise, a healthy diet and other steps like keeping a food diary.
Novo Nordisk sells two semaglutide versions for controlling blood sugar in Type 2 diabetics: a daily pill called Rybelsus and Ozempic, which patients inject weekly. The Danish company hasn’t disclosed Wegovy’s list price, but Ozempic typically costs $850 or more per month without insurance.
Wegovy builds on a trend in which makers of relatively new diabetes drugs test them to treat other conditions common in diabetics. For example, popular diabetes drugs Jardiance and Novo Nordisk’s Victoza now have approvals for reducing risk of heart attack, stroke and death in heart patients.
Phylander Pannell, 49, of Largo, Maryland, joined a patient study after cycles of losing and then regaining weight. She said she received Wegovy, worked out several times a week and lost 65 pounds over 16 months.
“It helped curb my appetite and it helped me feel full faster,” said Pannell. “It got me on the right path.”
Shortly after she finished the study and stopped receiving Wegovy, she regained about half the weight. She’s since lost much of that, started exercise classes and bought home exercise equipment. She’s considering going back on Wegovy after it’s approved.
Wegovy is a synthesized version of a gut hormone that curbs appetite. That’s a new strategy in treating obesity, said Dr. Robert Kushner, a member of Novo Nordisk’s medical advisory board who heads Northwestern Medicine’s Center for Lifestyle Medicine.
Novo Nordisk also is developing a pill version that should start final patient studies later this year.