On Thursday, the CDC’s advisory committee on vaccines voted unanimously—15 to 0—to add the Covid-19 vaccine to the country’s childhood immunization schedule.
This schedule of vaccines—which includes the vaccines for measles, mumps and rubella (MMR); tetanus, diphtheria, pertussis (Tdap); and inactivated polio—serves as the roadmap of routinely recommended vaccines for children across the nation. That’s among the many reasons the committee’s vote is consequential: State and local governments turn to the CDC’s guidance when deciding public health policy. The CDC has yet to adopt this guidance, but likely will in the coming weeks.
I believe it was both bad medicine and bad policy to add the Covid-19 vaccine to this list. I come to that conclusion for four reasons:
1. Parents are frustrated with the CDC and its Covid-19 guidance. And for very good reason. During the pandemic, many parents believed that CDC recommendations—on quarantine, for instance—resulted in local officials locking kids out of school for too long or unnecessarily, which resulted in devastating learning loss. But when those parents complained to the schools, education officials said they were simply following CDC recommendations. So now, while the CDC may be technically correct that inclusion of the Covid-19 vaccine on the immunization schedule is not a mandate, it feels to many parents like more buck-passing from this influential agency.
Covid-19 and the question of when—if ever—to vaccinate kids has become among the most politicized topics in the country. Many municipalities, private schools, and day care centers in left-leaning areas will see the CDC’s imprimatur as an opportunity to institute mandates.
Mandates are concerning for two reasons. First, it is not clear they are ethical. The standard rule in medicine is simple: We do not intrude upon individual autonomy unless that intervention provides sufficient benefit to third parties. This means there must be a large benefit to others— enough so the loss of autonomy is acceptable. Given that the Covid-19 vaccine does not halt virus transmission, the prerequisite is not met.
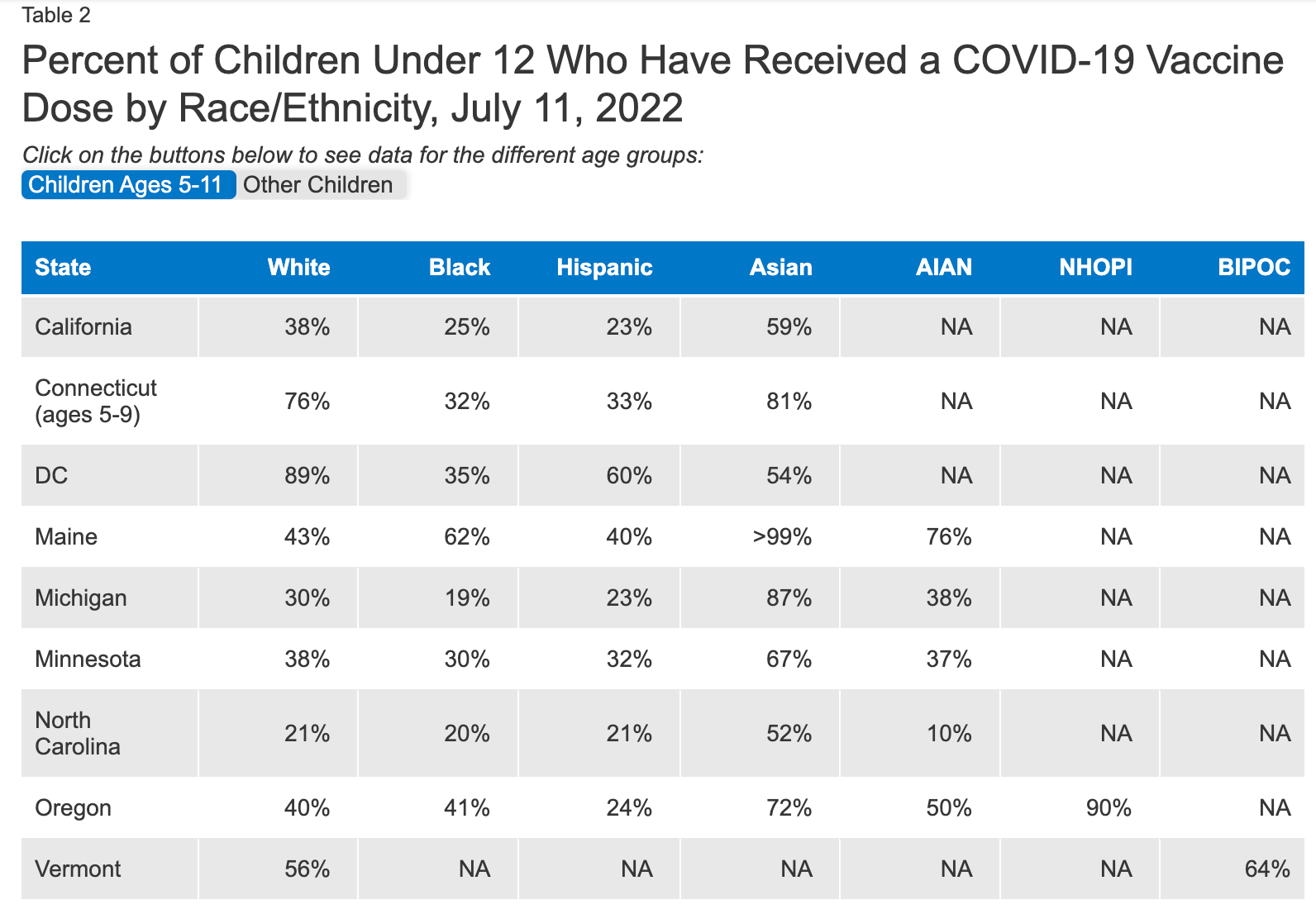
The second reason is that mandates will harm vulnerable kids. As of July, the Kaiser Family Foundation found that in several states, black and Hispanic children under 12 years old were less likely to be vaccinated than white children, as the chart below illustrates:
If mandates become the norm, unvaccinated children will be displaced to virtual school, home school, or perhaps no school at all. The harm to kids from substandard education—after nearly two years of disruption—far exceeds any gains from compliance. And that harm will disproportionately hurt poor, black kids. The same is true for mandates that prevent kids from participating in school sports. Being sedentary is far more damaging for children’s health than not getting this shot.
2. The CDC’s gamble could very well hurt vaccination rates more generally. In an effort to encourage Covid-19 vaccination, the CDC may wind up lowering vaccination rates for polio and measles. Why? Because by adding Covid-19 shots to the schedule, the CDC is tacitly implying that this new vaccine is as important to kids as the combination MMR one. This is absolutely false.
Measles can be a devastating childhood illness, but vaccination provides durable, sterilizing immunity. When vaccination rates are high, measles outbreaks can be averted. Covid-19 vaccines, as millions have learned, do not prevent you from getting Covid-19. Right now the CDC director Rochelle Walensky has Covid, despite being boosted with the bivalent booster just one month ago.
Covid vaccines do work to lower the risk of severe disease. But for healthy kids, the risk of severe disease is already extremely low. Once a child recovers from Covid, having had the disease itself provides immunity equivalent to—or perhaps better than—the vaccine. Currently, the CDC estimates that at least 86 percent of American children have had Covid. For this reason, I, along with policy makers in many advanced nations, think it is reasonable for a parent to vaccinate their child against Covid, and also reasonable not to.
One of the worst outcomes of the CDC Covid-19 vaccination recommendation would be if parents decide it is unnecessary for their children to get the Covid shot, they will also skip vital vaccines that have been saving lives for decades.
3. The U.S. is profoundly out of step with peer nations. For example, Denmark has ceased to offer vaccination in healthy kids under the age of 18, and does so only when deemed medically necessary. That’s because kids very rarely become seriously ill with Omicron. Sweden has just abandoned its recommendation for vaccinating healthy children above the age of 12 (it had never recommended vaccination for kids 5 to 11), and will only vaccinate children with medical problems. In making their new recommendation, the CDC fails to acknowledge the legitimate debate about what is best for children among our peer nations. (For males aged 10 to 40 myocarditis caused by the vaccine is an important safety concern. But this appears less common in younger children, and is not an issue for the childhood vaccination guidelines).
4. The CDC is also at odds with parents’ preferences. Data presented by the CDC show that only 6.9 percent of kids between the ages of six months and four years old have gotten even a single dose of the vaccine. Just 38.6 percent of kids between 5 and 11 have gotten one dose. Most parents have chosen not to give the Covid-19 vaccination to their kids. The CDC’s endorsement further puts the public health establishment not just out of step with other nations, but with most American parents. This risks deepening the lack of trust and authority in the agency.
To this day, the CDC advises Americans who were exposed to Covid to wear a mask in their own home for 10 days around others. It’s no wonder that the CDC has badly lost credibility with many Americans.
In 1998, the Lancet published a deeply flawed study that should never have appeared claiming vaccines were linked to autism. Eventually it was found to be fraudulent. Nevertheless, parents and activists ran wild with it. It has taken decades to fight the false connection between vaccines and autism—and it is still a battle not fully won. We need the public to believe in medically essential vaccines and be willing to give them to their children. To add an unnecessary and controversial vaccine to this list—at the risk of some states or local actors mandating it—undermines the broader good of public health.
Hematology Oncology Medicine Health Policy Epidemiology Associate Professor |