A total of 776 patients with symptomatic NERD have been enrolled and randomized in the multisite trial across the U.S.
Topline data for the primary endpoint is expected in Q1 2023 with full trial results available in late-2023
NERD is the largest subcategory of gastroesophageal reflux disease (GERD) and affects an estimated 45 million people in the U.S.
FLORHAM PARK, N.J., Oct. 24, 2022 (GLOBE NEWSWIRE) -- Phathom Pharmaceuticals, Inc. (Nasdaq: PHAT), a biopharmaceutical company focused on developing and commercializing novel treatments for gastrointestinal diseases and disorders, today announced it has completed enrollment in its PHALCON-NERD Daily Dosing Phase 3 trial of vonoprazan in non-erosive gastroesophageal reflux disease (NERD). Vonoprazan is an investigational first-in-class potassium-competitive acid blocker (PCAB) from a novel class of medicines that block acid secretion in the stomach. The Company expects to share topline data from the primary endpoint in the first quarter of 2023 and full results from the study in late 2023.
If successful, Phathom believes that the trial will form the basis of a supplemental New Drug Application (sNDA) for vonoprazan as once daily therapy for the treatment of symptomatic NERD in adults in 2023.
NERD is the largest subcategory of gastroesophageal reflux disease (GERD) and is characterized by reflux-related symptoms in the absence of esophageal mucosal erosions. There are estimated to be over 65 million individuals with GERD in the U.S., and it is estimated that seventy percent (70%) of this population have NERD.
The primary endpoint of the double-blind Phase 3 PHALCON-NERD-301 study is evaluating the efficacy of vonoprazan 10 mg and 20 mg as a daily dosing (QD) treatment, as compared to placebo (QD), in the relief of heartburn over four weeks in participants with symptomatic NERD. The trial also includes a unique blinded 20-week long-term extension period to further evaluate the safety and efficacy of both doses of vonoprazan after six months.
As of Oct. 20, 14 of London-based Hikma Pharmaceuticals' amoxicillin products and nine of Israel-based Teva Pharmaceuticals' supply are part of the national shortage, according to the ASHP's drug shortage website.
Amoxicillin comes in many forms — including capsules, powders and chewable tablets — but the most common type children take is the liquid form, which makes up at least 19 products that are part of the dearth.
Hikma's oral amoxicillin drugs are on allocation, meaning the drugmaker is curbing new orders to ensure it can meet current contracts. Teva told ASHP it expects its back-ordered products to return to normal supply levels between late October and early December.
Novartis' Sandoz business also has a lack of the antibiotic because of "significant" demand, a company spokesperson told Bloomberg.
Hikma, Teva and Sandoz account for three of four top manufacturers of the drug, according to Bloomberg. There are other antibiotics available, but the CDC recommends amoxicillin as a "first-line therapy" for multiple common pediatric infections.
PhaseBio Pharmaceuticalsplans to file Chapter 11 bankruptcy and sell off its bentracimab assets under a "stalking horse: arrangement with an unnamed large pharmaceutical company, the company announced Monday.
Bentracimab is being developed to reverse the anti-clotting effects of ticagrelor, more commonly known as AstraZeneca’s Brilinta.
Under a stalking horse arrangement, a buyer acts as the stalking horse bidder and agrees to set a minimum floor bid for the assets. Potential buyers can bid on the assets but must exceed the minimum bid. If no one does, the stalking horse bidder acquires the assets.
In this case, the unidentified company has agreed to pay PhaseBio $40 million in cash and another $60 million for hitting certain regulatory milestones related to bentracimab. It will also provide a $4 million deposit into escrow and, if approved as the stalking horse bidder, would receive a $2 million break-up fee and reimbursement of expenses of up to $750,000 to be paid from the proceeds of a sale to a different bidder.
“The Board and management team have thoroughly assessed all of our strategic options and believe that this structured process represents the best possible solution for PhaseBio, taking into account our financial needs and the challenges we have encountered while trying to negotiate a path forward with SFJ Pharmaceuticals,” Jonathan Mow, CEO of PhaseBio, stated.
PhaseBio and SFJ - a Tumultuous History
In January 2020, PhaseBio announced a financing and co-development collaboration with SFJ Pharmaceuticals in support of bentracimab.
Under the terms of the deal, SFJ agreed to fund up to $120 million in support of the drug’s development and take on a central role in clinical development and regulatory activities outside the U.S. SFJ would fund up to $90 million in development expenses through the end of 2021 and up to another $30 million based on various clinical milestones.
In a September filing, PhaseBio indicated that SFJ stated it needed to return the rights to bentracimab.
“SFJ has elected to cause the Company’s business related to bentracimab to be transferred to SFJ as a result of the Company’s failure to remedy its Going Concern Condition within the Going Concern Cure Period,” PhaseBio wrote in the SEC filing.
SFJ expected PhaseBio to transfer the rights to the drug within 10 days.
The two companies have been negotiating since early 2022 over the potential transfer of bentracimab program assets to SFJ. However, they were unable to reach a deal. SFJ then withdrew from the negotiations and informed PhaseBio about the transfer the day after the Going Concern Period expired.
SFJ is a private equity-backed firm that specializes in co-development deals. It would, theoretically, have the capabilities necessary to move bentracimab through the FDA approval process, but that would depend upon the FDA’s willingness to go along with PhaseBio’s plans to include Phase III data from only 25 to 30 patients with uncontrolled bleeds in the submission.
Analysts note that this was likely going to be a lengthy legal battle between PhaseBio and SFJ, but with less than $8 million in operating funds, PhaseBio didn’t have many resources to continue operations, let alone pay for a protracted legal battle.
In May, PhaseBio reported a successful pre-Biologics License Application (BLA) meeting with the FDA over a potential regulatory submission for bentracimab. At that time, they indicated plans to submit a BLA in the fourth quarter of this year.
The company stated it had plans to enroll 35 patients receiving ticagrelor who experienced uncontrolled bleeding events in the REVERSE-IT trial.
The FDA also confirmed a prior recommendation for post-marketing requirements that PhaseBio complete enrollment in the Phase III REVERSE-IT trial and submit data from at least 200 patients while also launching a post-approval registry study ahead of the product launch after a potential Accelerated Approval.
Technology will bundle and accelerate prior authorization for cardiovascular and surgical services
Cohere Health, a leader in intelligent utilization management (UM) technology, announced that Humana Inc. (NYSE: HUM) will expand its use of Cohere's digital UM collaboration platform to enable seamless prior authorization for cardiovascular and surgical services.
In addition to digitizing prior authorization requests for these services, the technology automates clinical intelligence into the provider's workflow, enabling episode-based, longitudinal management of the patient's care journey to reduce care variation, drive higher quality care, and minimize administrative burden. Both solutions will be deployed nationwide on January 1, 2023 for Humana Medicare Advantage members and Humana employees with the company's health plan.
In the three years or so since Covid-19 appeared, it has become increasingly clear, despite the protestations of virologists who do this kind of work, that the causative virus was probably the result of genetic manipulation in a lab. In other words, it is not a natural virus that spilled into humans from some wild animal host, but one that escaped from the Chinese laboratory in which it was being souped up as part of a high-risk scheme to predict future epidemics.
The case that Covid originated in a lab is not yet proven, but as circumstantial evidence goes, it’s pretty good. Few people appreciate quite how compelling this case is (see the outline below) because science journalists who work for the mainstream press have, by and large, failed to present it in full to their readers. Virologists, and through them most other researchers dependent on government grants, are not so keen to accept their community’s complicity in creating a pandemic that has caused upward of 6.5 million deaths. Driven by the position of their sources and the political leanings of their proprietors, mainstream science journalists have largely ignored each new piece of evidence pointing toward the lab-leak explanation, while uncritically overplaying the virologists’ self-serving arguments for the virus’s natural origin.
A particularly egregious example of this asymmetry is David Quammen’s Breathless. Quammen is a well-regarded and widely published writer about viruses and natural history, but he has grown too close to his sources, as many science writers do. He fails to consider the possibility that scientists can be swayed by the same monetary or careerist motives that drive lesser mortals. The lab at Wuhan, where researchers were manipulating Covid-type viruses, received funding from the U.S. National Institutes of Health. Could Francis Collins and Anthony Fauci, the NIH’s senior officials, have had any possible motive for suppressing their experts’ initial conclusion that the Covid virus was probably artificial? Could that explain why they apparently told no one else in government about their experts’ findings and excluded from their discussions then-CDC director Robert R. Redfield, who believed from the start that the virus was a lab escapee? Quammen does not think to raise such impolite questions.
The book showers positive epithets onto virologists who argue against the lab-leak scenario. Quammen praises as “highly respected” Edward Holmes, one of the initial group of experts who concluded that the virus was man-made but two days later changed his mind—on the basis of no known evidence but after a teleconference with Fauci and Collins on February 1, 2020. Michael Worobey is “rigorous, smart and judicious,” with a “quietly dauntless streak in him” and “steely attentiveness.” And if that weren’t enough, “his reputation is sterling and his mind is open.” This gusher of praise is Quammen’s attempt to bolster the credibility of a contentious article in which Worobey asserted that the virus must have passed naturally from animals to people in the Wuhan wet market. That argument indeed needs all the boosting it can get because no infected animal was found in the Wuhan market, and it’s impossible to exclude the likeliest explanation for Worobey’s data—namely, that the market just amplified an infection that started earlier and elsewhere, as even Chinese authorities assert.
Quammen goes furthest astray in his treatment of Peter Daszak, a central and still-enigmatic figure in the story of Covid’s origins. Daszak is president of the EcoHealth Alliance of New York. His agency was the intermediary between Fauci and Shi Zhengli, the chief expert on bat coronaviruses at the Wuhan Institute of Virology. Fauci could have given money to Shi directly but did so via Daszak, perhaps in part because domestic grants attract less regulatory scrutiny than foreign ones.
As part of the effort to squelch the lab-leak conjecture, Daszak organized a February 19, 2020, letter to the Lancet, a leading medical journal. “We stand together to strongly condemn conspiracy theories suggesting that COVID-19 does not have a natural origin,” wrote Daszak. “We declare no competing interests,” he and his co-signatories concluded. Of course, a gross conflict of interest did exist, one not declared to readers: Daszak funded and supervised Shi’s lab and would be held to account if that were the virus’s source.
But Quammen can’t bring himself to condemn even this ethical lapse. The best he can manage to say about the incident is, “Whether that constituted a conflict is another question.” Then comes the remarkable revelation that Quammen has known Daszak for many years and that “he is a friend of mine.” Too bad the reader is given this pertinent information only on page 294 of the book. No wonder almost everything Quammen has written until that point is an attempt to get Daszak off the hook for failing to supervise the ultra-high-risk work he was funding in alarmingly low-level safety conditions at the Wuhan Institute of Virology.
“I’m aware that journalists are not supposed to have friends,” Quammen writes plaintively of his relationship with Daszak. Not so—journalists just shouldn’t write about their friends if they cannot do so objectively.
Quammen interviewed many people on the natural origin side of the debate, including Shi, who has been inaccessible to most Western journalists. But he ignored serious critics of virus enhancement, known as gain-of-function research, such as Richard Ebright. Far from addressing the strongest parts of the lab-leak case, Quammen discusses only aspects of it that have never been taken seriously, such as the charge that the Covid virus was engineered from its close bat relative, a virus known as RATG13.
Readers may perceive that Quammen’s book is a work of advocacy, but many will be baffled as to what case he is attacking, because he never states it clearly—an omission his account shares with many others.
Here, briefly, is the case for the lab-leak origin.
Collins and Fauci have advocated since 2011 for the benefits of enhancing natural viruses in the lab with the hope of predicting future epidemics. From their powerful bureaucratic positions—they fund most virology research in the U.S.—they outmaneuvered critics who argued that the risks of creating novel infectious viruses were sky high and the benefits nugatory.
From 2014 onward, Fauci gave money, via Daszak, to researchers at the Wuhan Institute of Virology to collect bat coronaviruses in the wild and to manipulate the viral genomes in the lab. The goal was to see which held the greatest potential for infecting people.
In 2018, the Wuhan researchers applied to DARPA, a Defense Department agency, for a grant to construct novel, SARS-like viruses. Their plan was to take genetic elements such as the one known as the furin cleavage site and to insert them into a specific position on viral genomes. That position, a single point on the virus’s 30,000-unit long genome, is called the S1/S2 junction of the virus’s spike gene. Many viruses have furin cleavage sites, but none of the 300 known members of the SARS-like family of coronaviruses do. This is important because viruses often swap genetic elements with other viruses of their own family, but they cannot naturally acquire elements that their family does not possess.
In 2019, a novel virus, SARS-CoV-2, emerged in the city of Wuhan, home of the Wuhan Institute of Virology, and launched the Covid pandemic. The virus’s most unusual feature and a cause of its infectivity is a furin cleavage site inserted at the S1/S2 junction of its spike protein, just as outlined in the Wuhan virologists’ proposal to DARPA. The genetic coding of the virus’s furin cleavage site is designated in a sequence of units common to human cells and supplied in laboratory kits, but it is very rare in coronaviruses and unknown in the SARS-like coronavirus family.
Though viruses spill over from animal hosts to people quite often, they usually leave a trail of evidence when they do so. In the case of the SARS1 epidemic of 2003, virus researchers were able to trace the host population of wild bats, the mutations in the virus as it adapted from bats to civets and then to people, and the immunological traces it left in the human population. If SARS-CoV-2 has a natural origin, we should expect the same pieces of evidence to emerge. In three years, none has.
All this information, including the critical DARPA grant application, was available before Quammen’s book deadline. In telling only one side of a story that has two, he and many of his fellow science writers have failed their readers.
Nicholas Wade was science editor of the New York Times from 1990 to 1996.
One of the most consistent efforts made by “experts” during the early stages of the pandemic was to attempt to impress on the public that COVID was an extremely deadly disease.
While it’s clear that for the extremely elderly and severely immunocompromised, COVID does present significant and serious health concerns, the “experts” did their best to convince people of all age groups that they were in danger.
Initially the World Health Organization, in their infinite incompetence, made a substantial contribution to this perception by claiming that the mortality rate from COVID was shockingly high.
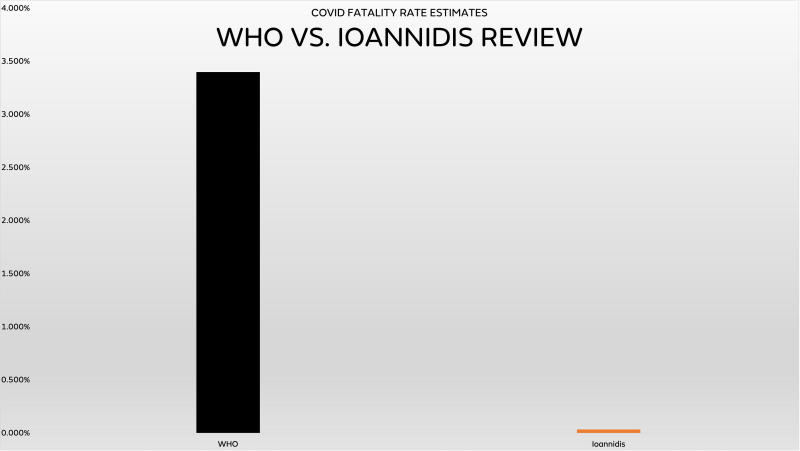
In March 2020, with precious little data, the WHO made the alarming claim that 3.4% of people who got COVID had died.
CNBC reported that an early press conference by WHO Director-General Tedros Ghebreyesus compared that expected mortality of COVID-19 to the flu:
“Globally, about 3.4% of reported COVID-19 cases have died,” WHO Director-General Tedros Adhanom Ghebreyesus said during a press briefing at the agency’s headquarters in Geneva. In comparison, seasonal flu generally kills far fewer than 1% of those infected, he said.
This stood in contrast to previous estimates, which were also above 2%:
“Early in the outbreak, scientists had concluded the death rate was around 2.3%.”
While “experts” could be forgiven for being unsure about the death rate of a brand new illness with very little data available, the fear-mongering and world-altering policy enacted based on these estimates has caused incalculable damage.
It’s now widely known and accepted that these estimates were wildly incorrect, off by orders of magnitude.
But a new paper out from one of the world’s leading experts confirms that they were off even more than we previously realized.
John Ioannidis is one of the nation’s leading public health experts, employed at Stanford University as Professor of Medicine in Stanford Prevention Research, of Epidemiology and Population Health,” as well as “of Statistics and Biomedical Data Science.”
You’d think that those impeccable qualifications and a track record of being one of the most published and cited scientists in the modern world would insulate him from criticism, but unfortunately that’s no longer how The Science™ works.
Ioannidis first drew the ire of The Keepers of The Science™ early in the outbreak, when he cautioned that society might be making tremendous decisions based on limited data that was of poor quality.
He also took part in the infamous seroprevalence study conducted in Santa Clara County, led by Dr. Jay Bhattacharya.
That examination, which looked at antibody prevalence in the San Jose area, came to the conclusion that COVID was already significantly more widespread by March and April 2020 than most people realized.
This had wide-ranging implications, but the most important revelation was that the estimates of COVID’s mortality rate used by “scientists” and the WHO were almost certainly much too high.
Those estimates were created under the assumption that COVID cases were overwhelmingly detectable; that cases were captured by testing and thus tracking deaths could be achieved with a “case fatality rate,” instead of “infection fatality rate.”
That was the mistake Tedros and the WHO made two and a half years ago.
Of course, for providing substantial evidence and data that COVID was less deadly than initially feared, Ioannidis (and Bhattacharya) was attacked from within the “expert community.”
In what has now become a familiar insult, those behind the study were vilified as COVID minimizers and dangerous conspiracy theorists who would get people killed by not taking the virus seriously enough.
But Ioannidis remained undeterred, and with several authors, he recently released another review of the infection fatality rate of COVID. Importantly, the paper looks at the pre-vaccination time period and covers the non-elderly age groups; those who were most affected by COVID restrictions and endless mandates.
The Numbers
The review begins with a statement of fact that was almost entirely ignored by lockdown “experts” throughout the pandemic, but especially when restrictions, lockdowns and mandates were at their peak early on.
The infection fatality rate (IFR) of COVID-19 among non-elderly people in the absence of vaccination or prior infection is important to estimate accurately, since 94% of the global population is younger than 70 years and 86% is younger than 60 years.
Emphasis added.
94% of the global population is younger than 70 years old.
6% of is older than 70 years old.
86% is younger than 60 years old.
This is relevant because restrictions overwhelmingly impacted the 86-94% of people who are younger than 60 or 70 years old.
Ioannidis and his co-writers reviewed 40 national seroprevalence studies that covered 38 countries to come to determine their estimates of infection fatality rate for the overwhelming majority of people.
Importantly, those seroprevalence studies were conducted before the vaccines were released, meaning the IFR’s were calculated before whatever impact vaccines had on younger age groups.
So what did they find?
The median infection fatality rate for those aged 0-59 was 0.035%.
This represents 86% of the global population and the survival rate for those who were infected with COVID pre-vaccination was 99.965%.
For those aged 0-69, which covers 94% of the global population, the fatality rate was 0.095%, meaning the survival rate for nearly 7.3 billion people was 99.905%.
Those survival rates are obviously staggeringly high, which already creates frustration that restrictions were imposed on all age groups, when focused protection for those over 70 or at significantly elevated risk would have been a much more preferable course of action.
But it gets worse.
The researchers broke down the demographics into smaller buckets, showing the increase in risk amongst older populations, and conversely, how infinitesimal the risk was amongst younger age groups.
They added that “Including data from another 9 countries with imputed age distribution of COVID-19 deaths yielded median IFR of 0.025-0.032% for 0-59 years and 0.063-0.082% for 0-69 years.”
These numbers are astounding and reassuringly low, across the board.
But they’re almost nonexistent for children.
Yet as late as fall 2021, Fauci was still fear-mongering about the risks of COVID to children in order to increase vaccination uptake, saying in an interview that it was not a “benign situation:”
“We certainly want to get as many children vaccinated within this age group as we possibly can because as you heard and reported, that this is not, you know, a benign situation.”
It’s nearly impossible for any illness to be less of a risk, or more “benign” than a 0.0003% risk of death.
Even in October 2021, during that same interview with NPR, Fauci said that masks should continue on children as an “extra step” to protect them, even after vaccination:
And when you have that type of viral dynamic, even when you have kids vaccinated, you certainly – when you are in an indoor setting, you want to make sure you go the extra step to protect them. So I can’t give you an exact number of what that would be in the dynamics of virus in the community, but hopefully we will get there within a reasonable period of time. You know, masks often now – as we say, they’re not forever. And hopefully we’ll get to a point where we can remove the masks in schools and in other places. But I don’t believe that that time is right now.
Nothing better highlights the incompetence and misinformation from Dr. Fauci than ignoring that pre-vaccination, children were at vanishingly small risks from COVID, that vaccination uptake amongst kids was entirely irrelevant since they do not prevent infection or transmission, and that mask usage is completely ineffective at protecting anyone. Especially for those who didn’t need protection in the first place.
The CDC, “expert” community, World Health Organization, media figures — all endlessly spread terror that the virus was a mass killer while conflating detected case fatality rates with infection fatality rates.
Yet now we have another piece of evidence suggesting that the initial WHO estimates were off by 99% for 94% of the world’s population.
Just for some perspective, here’s the difference visually portrayed between what the WHO claimed and what Ioannidis found:
Whoops
Even if the lockdowns, mask mandates, capacity limits and shuttered playgrounds worked, the dangers of the virus were so minuscule that the collateral damage instantly and immediately outweighed any potential benefit.
Economic destruction, increased suicide attempts due to seemingly indefinite isolation, horrifying levels of learning loss, increasing obesity amongst kids, plummeting test scores, increased poverty and hunger, supply chain problems, rampant inflation; all of it is a direct result of policies imposed by terrified, incompetent “experts.”
Their estimates were hopelessly, catastrophically wrong, yet they maintained their unchallenged sense of authority for multiple years, and still receive awards, praise, increased funding and a sense of infallibility amongst politicians and decision-makers.
If sanity and intellectual honesty still existed, these estimates would be front page news for every major media outlet in the world.
Instead, because the media and their allies in the tech, corporate, and political classes promoted and encouraged lockdowns and restrictions while censoring dissent, it’s ignored.
Nothing could be more perfectly COVID than that.
Ian Miller is the author of“Unmasked: The Global Failure of COVID Mask Mandates.”His work has been featured on national television broadcasts, national and international news publications and referenced in multiple best selling books covering the pandemic. He writes a Substack newsletter, also titled “Unmasked.”