A plurality of Americans (42%) have no opinion or have never heard of gender ideology.
Republicans are the only group who have a majority with an opinion (62% unfavorable).
WHY IT MATTERS –While the embrace of gender ideology by our major institutions is an issue of intense conversation amongst right-leaning voters, the rest of America is not as engaged.
Candidates and activists who want to build a majority coalition must be careful not to talk past their audience.
HOW TO USE THIS DATA – The report offers language for defining gender ideology and an example of how to build a large majority opposed to its overreach.
This report builds on our earlier research on gender ideology in schools and the military.
Click on the image below to read the full report, including charts with demographic breakdowns…or read the summary below.
A plurality of Americans (42%) have never heard of gender ideology or have no opinion.
This is particularly true among those voters in America’s New Majority who are undecided on the generic ballot (59%) and leaning Democrat but are persuadable (58%).
Among all voters, more have an unfavorable opinion than have a favorable opinion of gender ideology (39%-19%).
Republicans are the only group who have a majority with an opinion (62% unfavorable).
Gen Z (31%) and Democrats (30%) have the highest portion of voters with a favorable opinion of gender ideology.
Once defined, 53% of Americans have an unfavorable opinion of gender ideology, compared to 30% with a positive opinion.
The largest negative shift in net favorability once gender ideology is defined occurs with Republicans (-15%) and Asians (-8%).
The largest positive shift in opinion toward gender ideology once it is defined occurs with the Left Minority (+21%), Gen Z (+18%), and Democrats (+13%).
The shift in net favorability is larger among America’s New Majority (-11%) than among all voters (-3%).
Key target groups of voters in America’s New Majority had a negative shift in opinion, including those who are undecided on the generic ballot (-7%) and those leaning Democrat but are persuadable (-4%).
Like the issue of abortion, there is much stronger opposition to using taxpayer dollars to promote gender ideology in government agencies than there is negative opinion about gender ideology itself.
64% oppose using federal tax dollars to promote gender ideology.
This includes majorities of Independents (68%), Swing Voters (68%), Asians (64%), Hispanics (60%), and Millennials (55%).
Only Democrats have a plurality in favor (41%).
75% of voters in America’s New Majority oppose using taxpayer dollars to promote gender ideology in government agencies – larger than among all voters (64%).
This includes majorities among voters in America’s New Majority who are undecided on the generic ballot (56%) or leaning Democrat but are persuadable (59%).
Even stronger opposition to using taxpayer dollars to promote gender ideology in foreign countries.
69% oppose federal tax dollars being used to promote gender ideology in foreign countries.
This includes majorities of Independents (73%) and Swing Voters (73%).
Only Gen Z narrowly favors (43-40%).
79% of voters in America’s New Majority oppose federal tax dollars being used to promote gender ideology in foreign countries.
This includes majorities among the key target groups in America’s New Majority – those who on the generic ballot are undecided (60%) or leaning Democrat but are persuadable (71%).
Following the French Revolution, the British philosopher Edmund Burke signaled a note of caution, warning that the desire for progress, uninhibited by convention, can lead to disaster. Revolutions in the name of lofty ideals—liberty, equality, science—can yield their opposites. A revolution in our time merits similar consideration: the transformation of human sexuality and, in particular, the rise of so-called transgender medicine.
The gender surgery program at Oregon Health & Science University, a public teaching hospital in downtown Portland, provides a productive tableau for analysis. The program is led by Blair Peters, a self-described “queer surgeon” who sports neon-pink hair, uses “he/they” pronouns, and specializes in vaginoplasty (the creation of an artificial vagina), phalloplasty (the creation of an artificial penis), and “non-binary” surgeries, which nullify the genitals altogether. Peters and his colleagues have pioneered the use of a vaginoplasty robot, which helps efficiently castrate male patients and turn their flesh into a “neo-vagina.”
Business is booming. According to Peters, OHSU’s gender surgery clinic has “the highest volume on the West Coast,” and his robot-assisted vaginoplasty program can accommodate two patients per day. His colleague Jens Berli, who specializes in phalloplasty, boasts a 12- to-18-month waiting list for a consultation and an additional three- to six-month waiting list for a surgical appointment.
This openness marks a revolution in manners and morals. In the past, transgender theorists acknowledged that their surgical transformations were disturbing and anti-normative. “I find a deep affinity between myself as a transsexual woman and the monster in Mary Shelley’s Frankenstein,” wrote the male-to-female transgender theorist Susan Stryker in 1994. “I will say this as bluntly as I know how: I am a transsexual, and therefore I am a monster.”
Such views no longer prevail. Today’s transgender medical providers conceal the barbarity of their practices in euphemisms. They are not postmodern Dr. Frankensteins but providers of “life-saving, gender-affirming care.” The model patient is no longer the middle-aged autogynephile but the troubled teenager, sold a new identity, mediated through technology, that promises to resolve deep-seated sexual anxieties—and advance the political cause of transgender activists.
The dismal metaphysics that lies beneath OHSU’s castration machines is academic queer theory, which holds that human beings are mere vehicles of “performativity” and that their nature can be molded and reshaped at will. In other words, the queer theorists argue, there is no “human nature” that cannot be transcended or obliterated through the application of culture and science.
OHSU’s castration machines must be seen in this light. The university’s doctors and surgeons believe that they can harness the advances of modern medical science to sublate the basic categories of human sexuality and replace them with a variety of synthetic forms: the artificial phallus; the artificial vagina; the dual phallus-vagina; nullification of both.
The technique for the robot-assisted vaginoplasty is gruesome. According to a handbook published by OHSU, surgeons first cut off the head of the penis and remove the testicles. Then they turn the penile-scrotal skin inside out and, together with abdomen cavity tissue, fashion it into a crude, artificial vagina. “The robotic arms are put through small incisions around your belly button and the side of your belly,” the handbook reads. “They are used to create the space for your vaginal canal between your bladder and your rectum.” The illustrated surgical literature is a catalog of horrors—peruse at your own risk.
This procedure is plagued with complications. OHSU warns of wound separation, tissue necrosis, graft failure, urine spraying, hematoma, blood clots, vaginal stenosis, rectal injury, fistula, and fecal accidents. Patients must stay in the hospital for a minimum of five days following the procedure, receiving treatment for surgical wounds and having fluid drained through plastic tubes. Once they are home, patients must continue on transgender hormone treatments and manually dilate their surgically created “neo-vagina” in perpetuity; otherwise, the tissue will heal, and the cavity will close.
One question provokes particular dread: Are the surgeons at OHSU using these machines on children? The answer appears to be yes. In an interview, Peters acknowledged that, in recent years, he has seen “a lot of adolescents presenting for surgical intervention” and that he has performed genital surgeries, including the robot-assisted vaginoplasty, on “a handful of puberty-suppressed adolescents.” Peters further stated that OHSU is “just putting [its] first series together” related to adolescent vaginoplasty and that “no one has published on it yet.” (When reached for comment, OHSU declined to respond.)
All this grisly detail is obscured through manipulative language. To the general public, Peters and his colleagues present their case in therapeutic terms—gender, affirmation, trauma, care, health, joy—and wrap themselves in the movement’s light blue, pink, and white flag. By comparison, the old transgender theorists were more honest. They saw themselves in Frankenstein and, in their struggle to overcome natural limits, brushed against them.
We can return to Burke for a final word. Besides his analysis of revolution, Burke’s other major contribution to the history of ideas was his theory of the sublime. The sublime, he argued, did not stimulate love, but terror. The vast darkness, the brewing storm, the dangerous tyrant—all elicited a complex reaction of astonishment and fear, especially that of human finitude.
Transgender surgery provokes a similar sentiment: awe of the mechanical mastery, horror at the raw human barbarism. But when the haze of emotions passes, the true nature of these interventions is revealed—they are a work of pure hubris, part of a scientific revolution that has sought to transcend all moral bounds. The revolution’s works, like Dr. Frankenstein’s, will inevitably leave behind a profound human tragedy.
Someone (who needs to remain anonymous) was able to obtain the death certificates from Minnesota for all deaths that occurred from 2015 to the present, which presented the opportunity to see if the CDC is being entirely honest about the US death data. Unsurprisingly, the CDC is not.
As we shall document, the CDC is concealing references to a covid vaccine on Minnesota death certificates (that are exceedingly rare to begin with because of widespread medical establishment denialism of vaccine adverse side effects). In almost every death certificate that identifies a covid vaccine as a cause of death, the CDC committed data fraud by not assigning the ICD 10 code for vaccine side effects to the causes of death listed on the death certificate.
Background
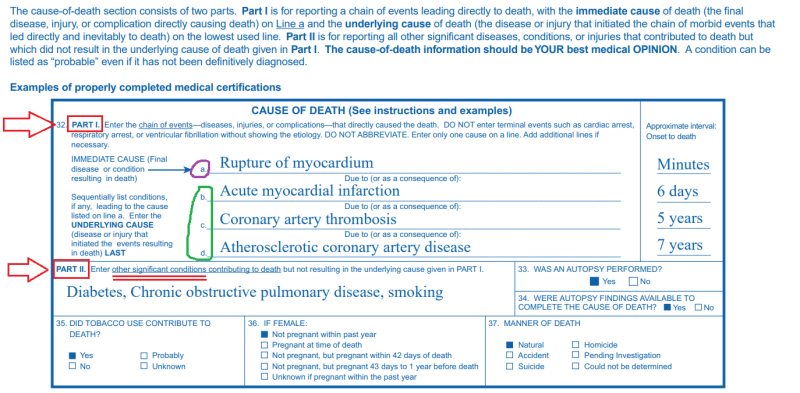
When someone dies, there is a death certificate that is filled out for official/legal purposes. Death certificates contain a lot of information (some states include more than others), including the causes of death (CoD).
Causes of death refer to the medical conditions that ultimately played some role in the demise of the decedent. To qualify as a CoD, a condition only needs to contribute to the medical decline of the decedent in some way, but doesn’t have to be directly responsible for whatever ultimately killed the person. If someone had high blood pressure, and subsequently suffered a heart attack that led to cardiac arrest which killed them, all three conditions qualify as CoD. On the other hand, this unfortunate fellow’s ingrown toenail is not a cause of death, because it in no way contributed to their demise.
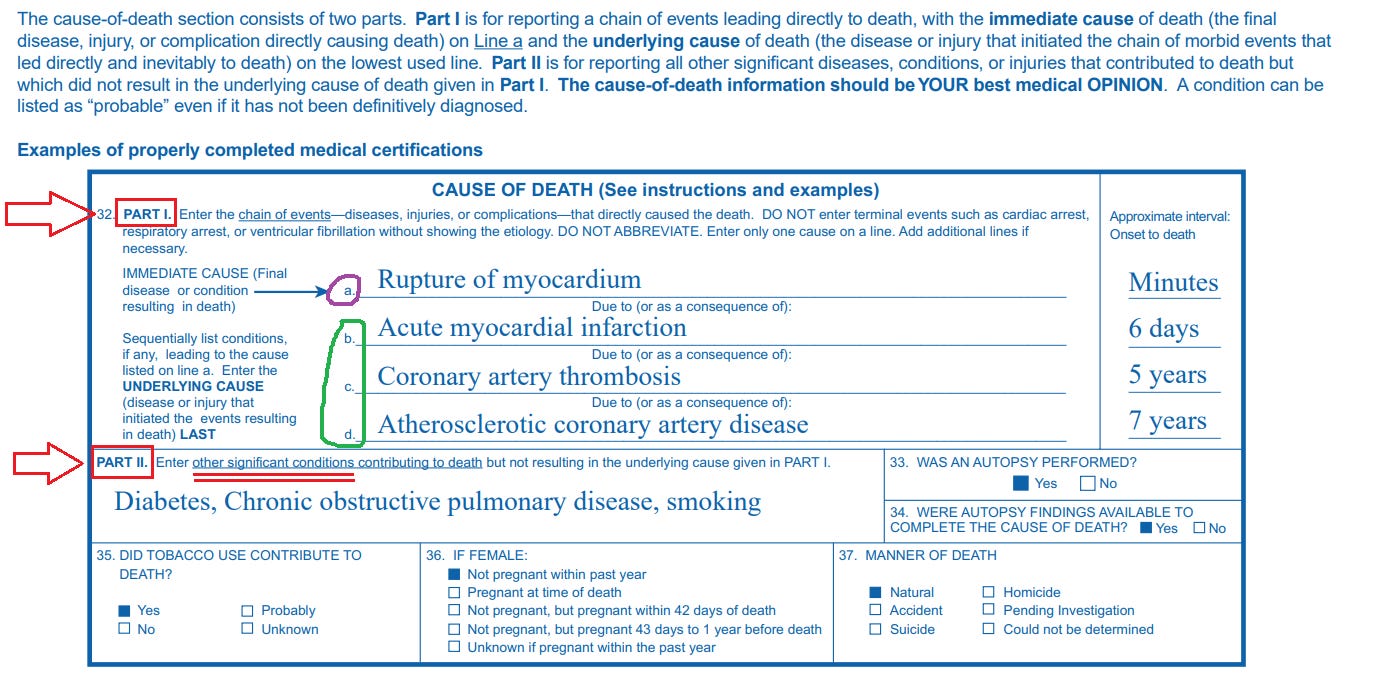
This is from the CDC’s own guidance explaining how to properly fill out CoD’s on a death certificate (you don’t need to understand the difference between Cause A, B, etc for this article):
The critical thing to keep in mind is that the person filling out the death certificate writes a text description of the CoD’s, but doesn’t assign the ICD 10 codes for the CoD’s.
That’s the CDC’s job.
ICD 10 Coding System for CoD’s
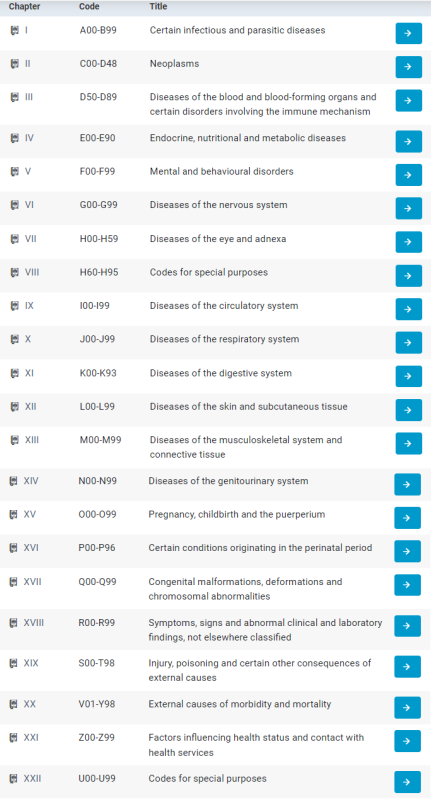
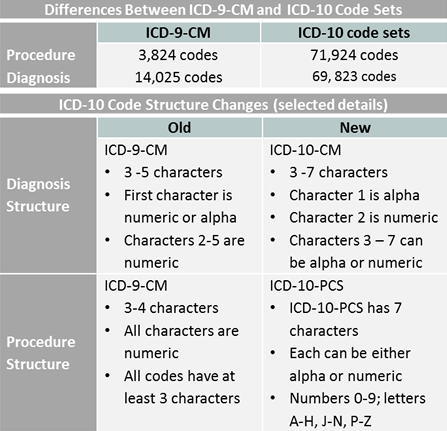
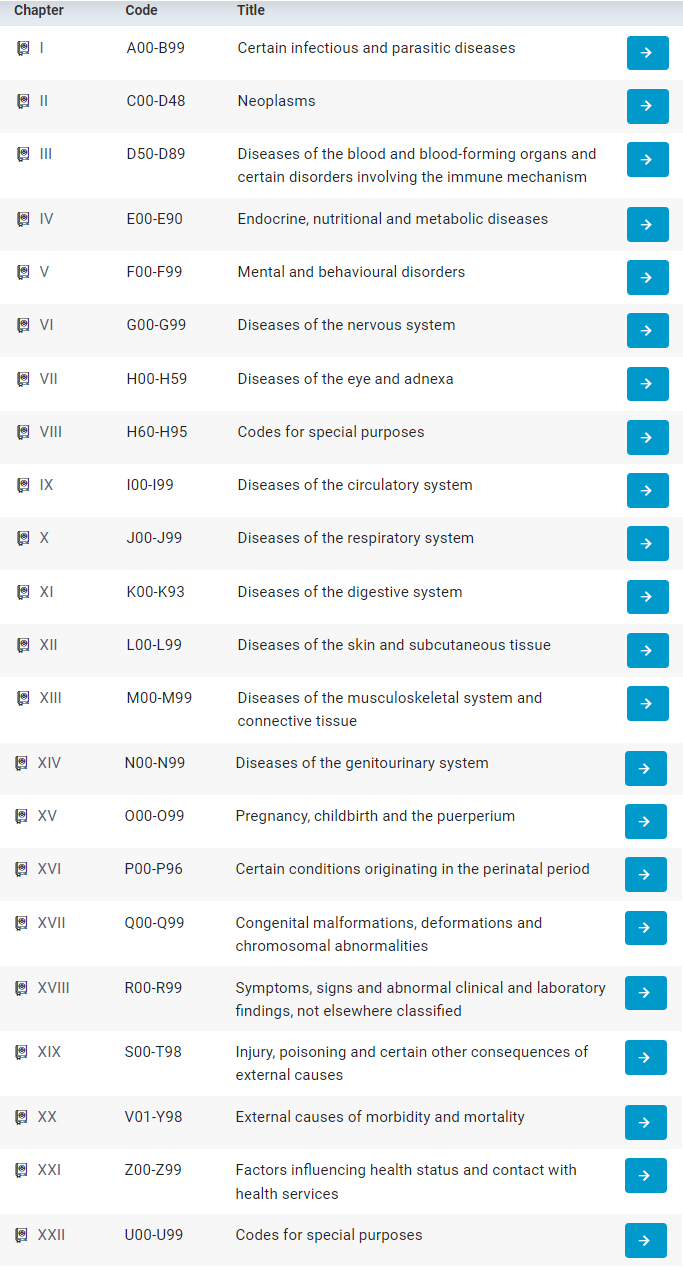
There is a fancy coding system that is used to classify the many thousands of medical conditions that can play a role in death known as the International Classification of Diseases. Every few years, it is updated/revised to keep up with new medical (or bureaucratic) developments, as new conditions are discovered and old conditions are reorganized or reclassified.
The current iteration of the ICD that was used for the deaths we’re looking at is the ICD 10 (that’s the 10th version). It is basically a hierarchical classification system:
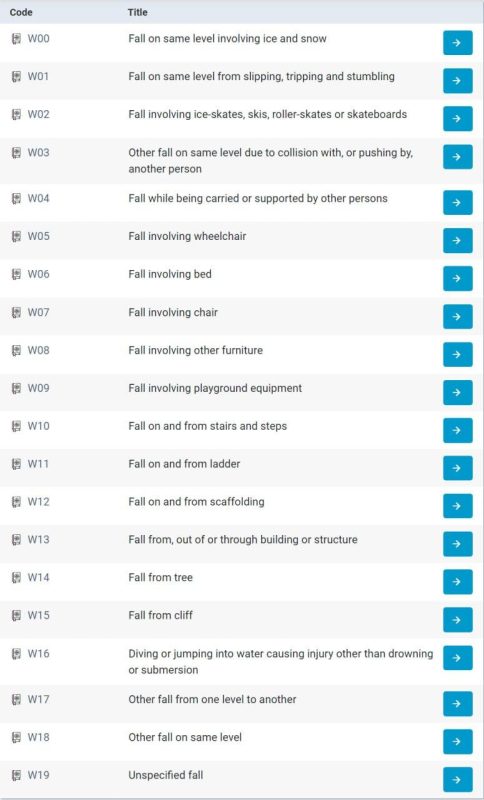
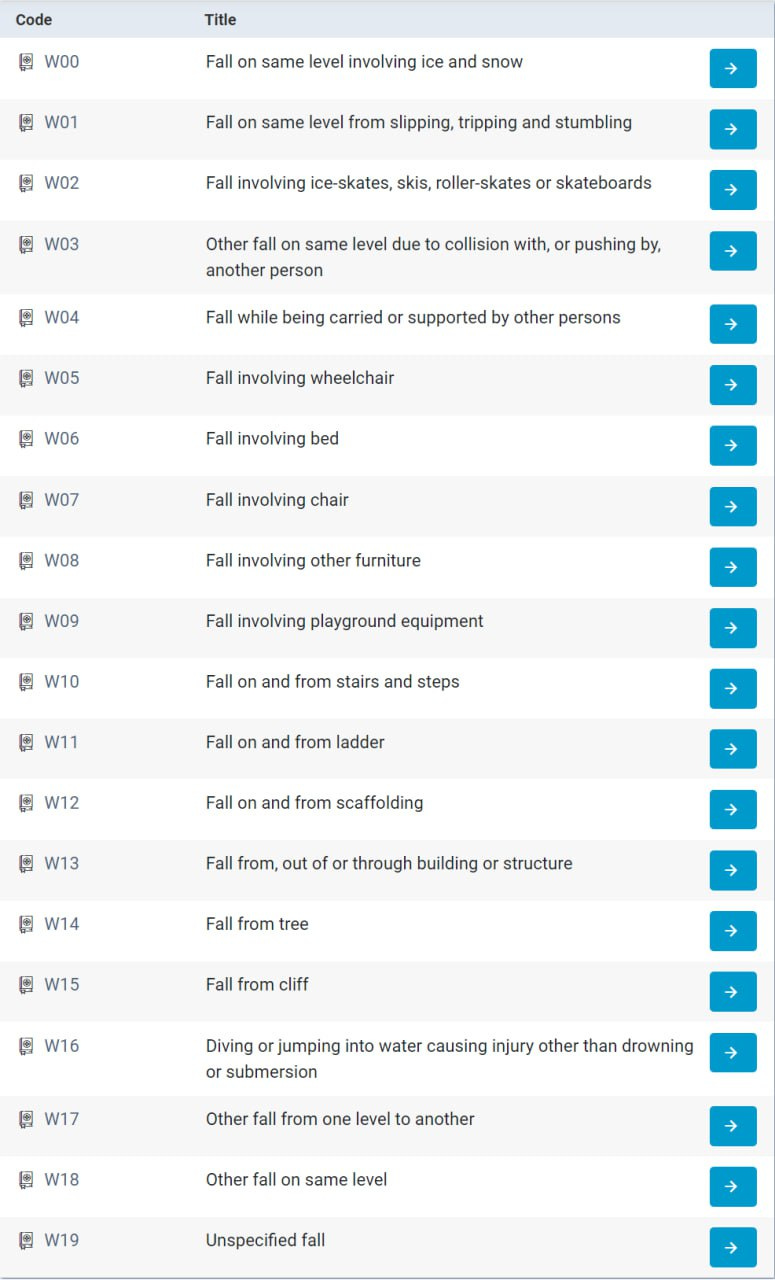
There are codes for practically every random weird thing you can think of:
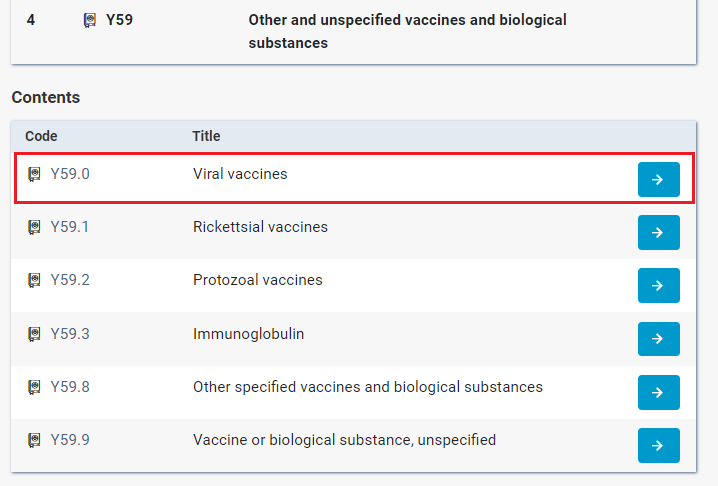
These are categories themselves – a code can go as 7 characters long:
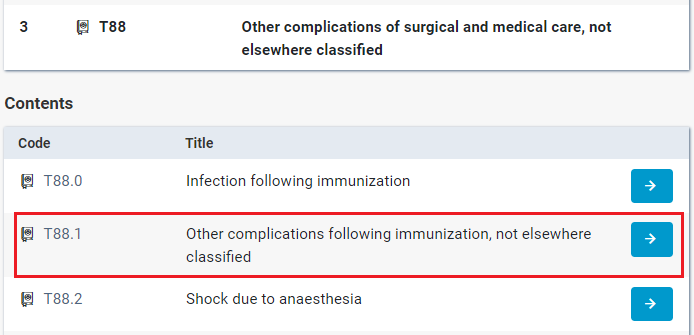
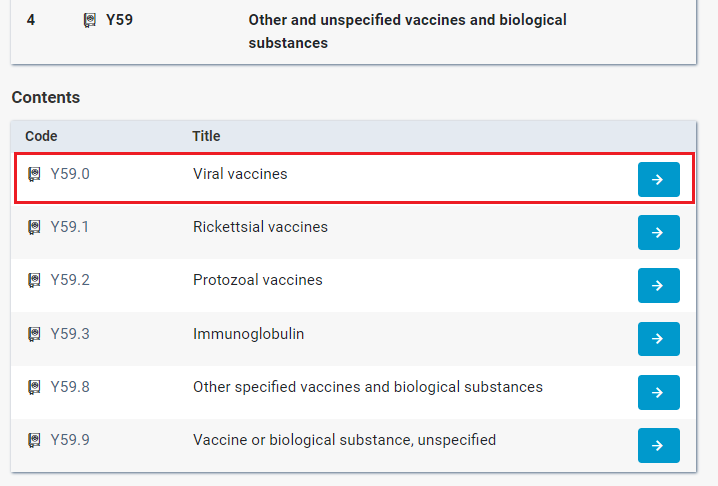
(There are other ICD 10 codes for various specific complications or side effects of vaccines, but the point remains that an ICD 10 code for vaccine side effects exists.)
CDC – Centers for Data Concealment
The CDC receives the death certificates from the various states and applies ICD 10 codes. This is primarily done with a secret algorithm, with a tiny percentage of cases adjudicated by CDC staff when the algorithm is unable to confidently assign an ICD code to the text description written on the actual death certificate (such as confounding spelling or a text description that does not make much sense). I confirmed this with a biostatistician who works for a DoH in a US state (I’m leaving out which one because I want to preserve my persona grata status). The individual who obtained the MN death certificates likewise confirmed with state officials that the ICD codes in their data were assigned by the CDC.
What a death certificate identifying a covid vaccine as a CoD *should* look like
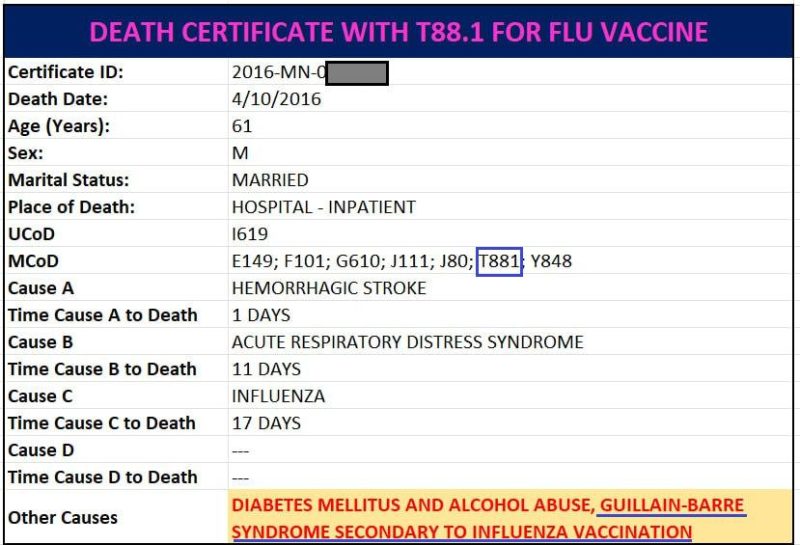
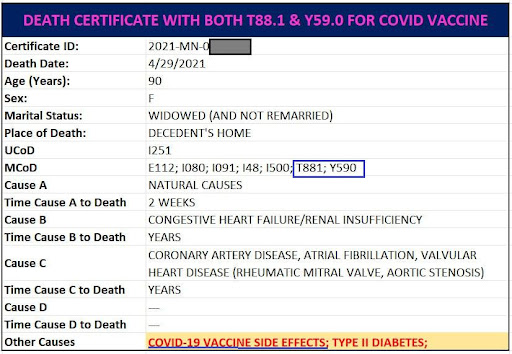
There are three death certificates in the MN tranche that contain either T88.1 or Y59.0. One is for a flu vaccine reaction, and – surprisingly – the other two are for a covid vaccine.
Note – when used below:
UCoD (Underlying Cause of Death) refers to “the disease or injury that initiated the train of events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury.”
MCoD (Multiple Causes of Death) refers to “the immediate cause of death and all other intermediate and contributory conditions listed on the death certificate.” (everything else)
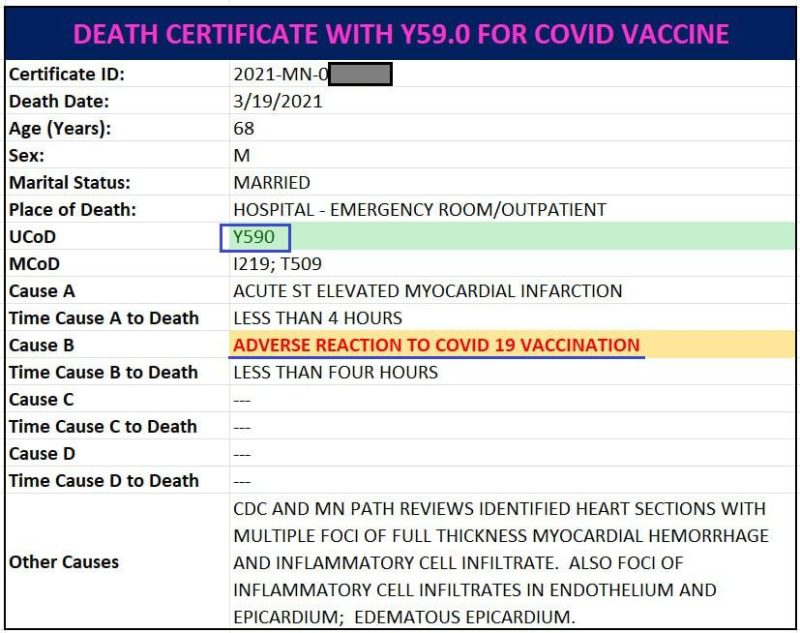
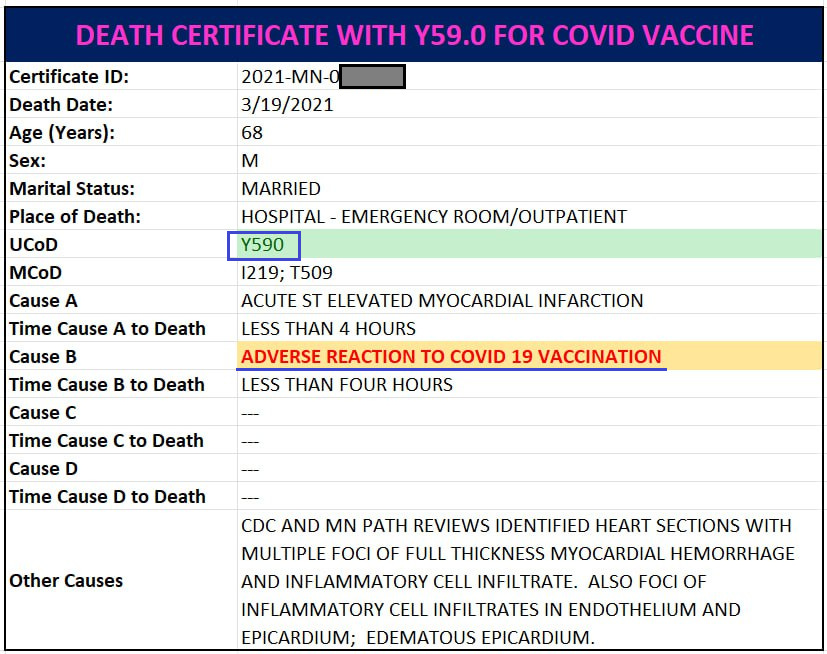
The first death certificate contains a covid vaccine ICD (below), and it looks like the CDC was trapped and could not avoid putting it on without fundamentally rewriting the death certificate, because the vaccine complication is unambiguously listed as the UCoD (this death certificate is saying the person was killed by a heart attack caused by the covid vaccine within minutes of injection):
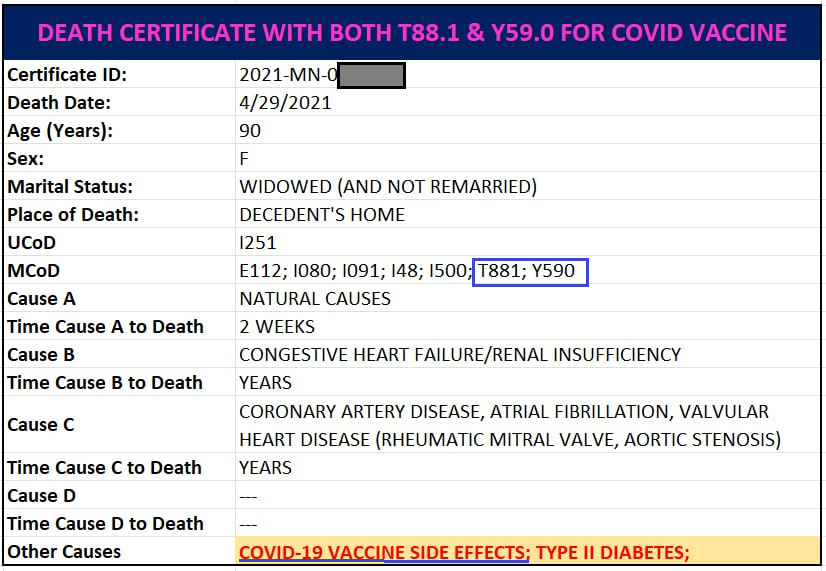
The second death certificate the CDC deigned to assign a vaccine ICD (and not only one but *BOTH* vaccine ICD codes(!!)) feels like perhaps a rogue CDC employee was working that day and snuck it in:
In any event, as we can clearly see, both T88.1 and Y59.0 are indeed appropriate for when a covid vaccine is listed as a CoD. Thus the CDC cannot claim that there was no official ICD 10 code that could be used to designate covid vaccines (or any other excuse).
The FRAUD:
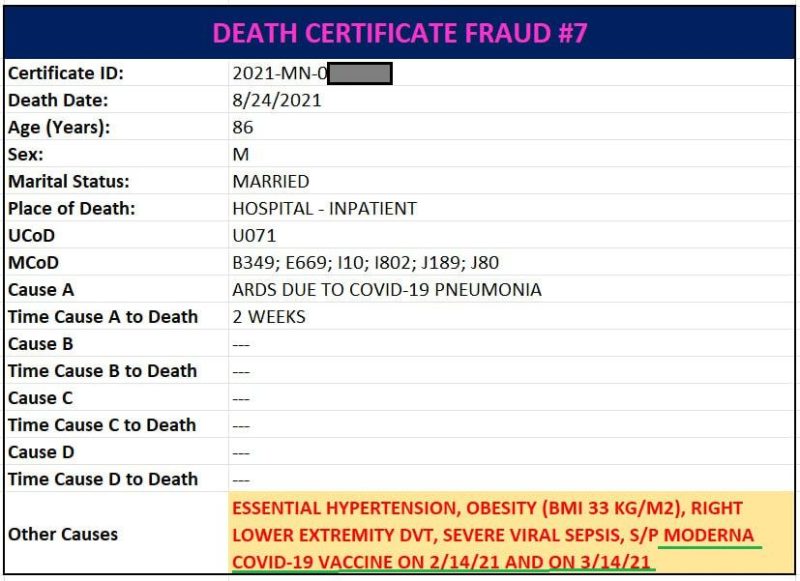
With that introduction, below are 7 death certificates from Minnesota that identify a covid vaccine as a cause of death where the CDC omitted the corresponding ICD 10 code identifying a vaccine side effect when the CDC assigned ICD codes to the death certificates.
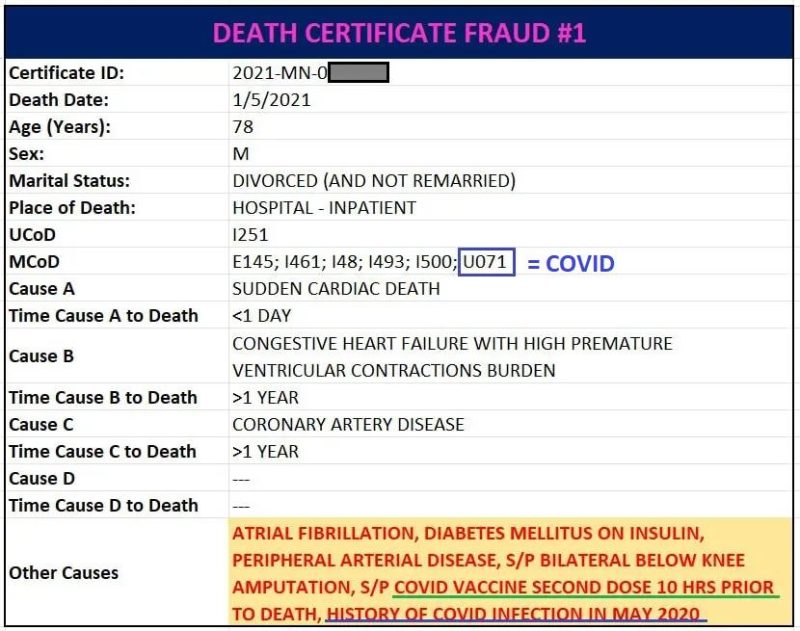
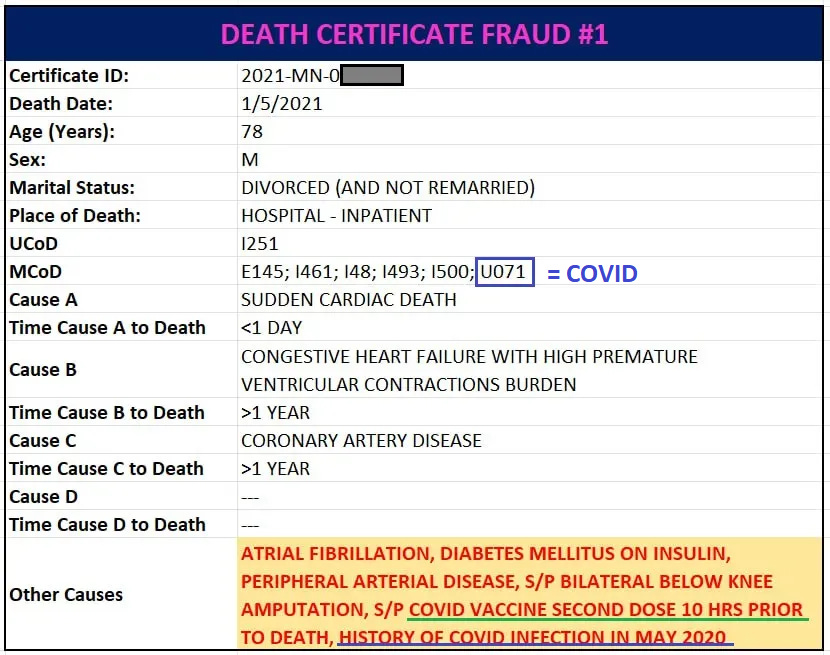
The first fraudulently filled out death certificate offers a crucial detail highlighting not only the fraud but the naked double standards for assigning CoD’s.
This death certificate identifies both a covid vaccine and covid itself as contributory CoD’s (in the last row highlighted in yellow, vaccine underlined in green, covid in blue):
“covid vaccine second dose 10 hrs prior to death”
“history of covid infection in May 2020” (about 7-8 months prior to death)
Any remotely objective person would presume that if a condition that occurred 7 months prior without any clear link to the actual death still nevertheless meets the standard for being identified as a CoD, then surely a condition or event that occurred a mere TEN HOURS before death identified by the doctor filling out the death certificate merits inclusion as a CoD.
Yet, the CDC assigned U70.1 – “COVID-19, virus identified” – for covid, but neglected to assign T88.1 or Y59.0 for the covid vaccine.
A second point to highlight is that we see that anything mentioned as a CoD, even in the context of “history of” that had (presumably) been long resolved, is a legitimate CoD insofar as assigning an ICD 10 code and epidemiological data are concerned.
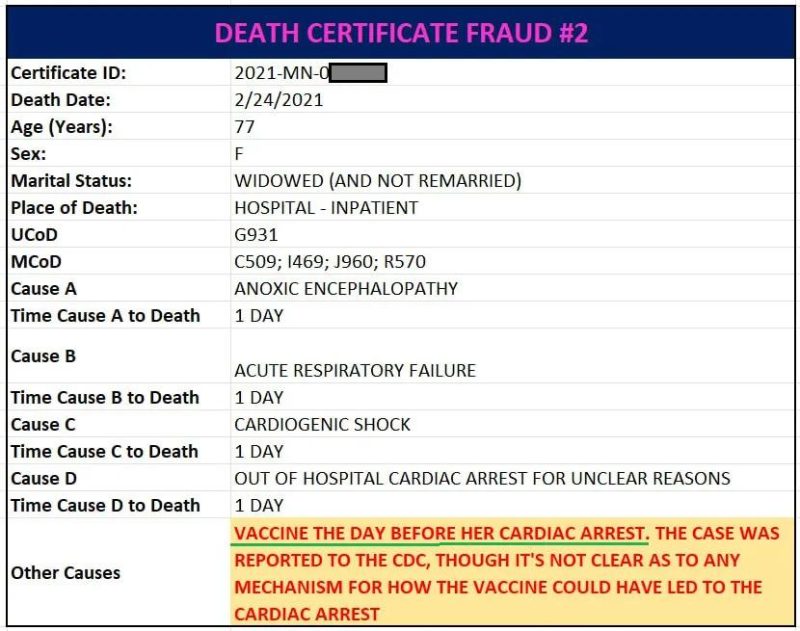
This decedent suffered a cardiac arrest that ultimately led to her death *ONE DAY* after being vaccinated.
(For the record, I am not bothered by the “though it’s not clear as to any mechanism for how the vaccine could have led to the cardiac arrest” line. This death occurred February 24, 2021 – well before there was any sort of public awareness about the multiple plausible mechanisms by which the vaccine could cause heart damage. So to me, whoever filled out the death certificate was a gutsy fellow willing to identify a covid vaccine on a death certificate that had his name on it.)
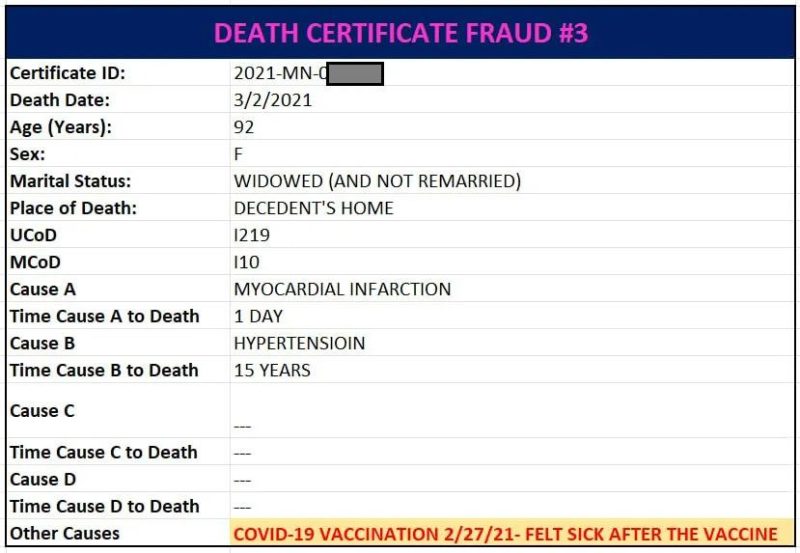
Fraudulent Death Certificate #3
This death certificate doesn’t merely identify a covid vaccine, it explains that the decedent “felt sick after the vaccine” and died 4 days later from a heart attack. Yet, no T88.1 or Y59.0.
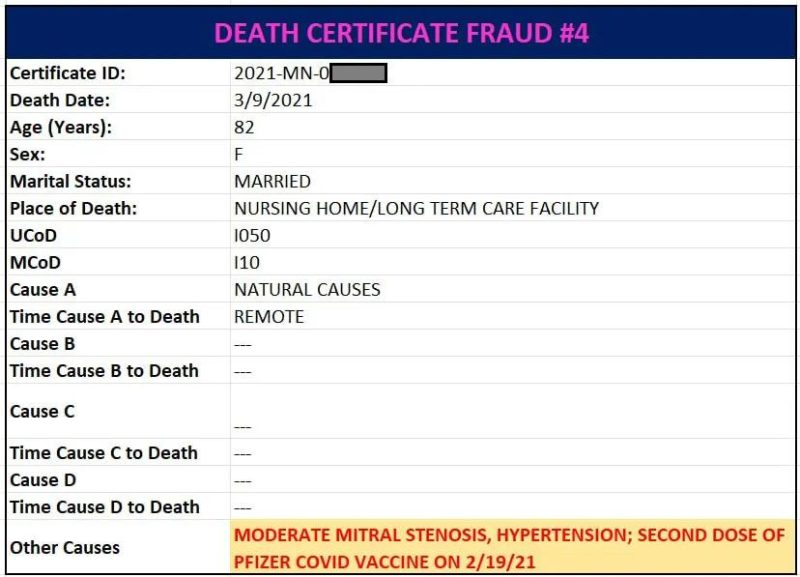
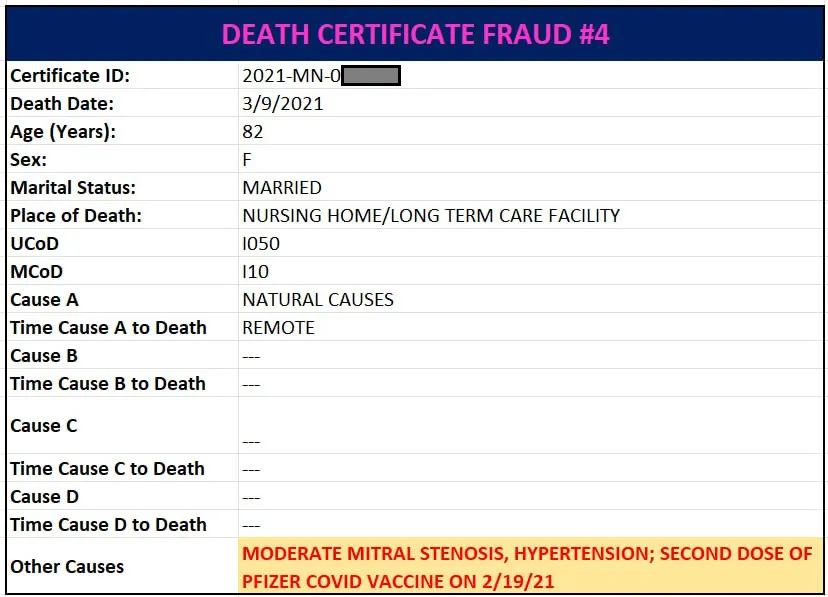
This death certificate provides that the decedent received her second dose of Pfizer 18 days prior to her death.
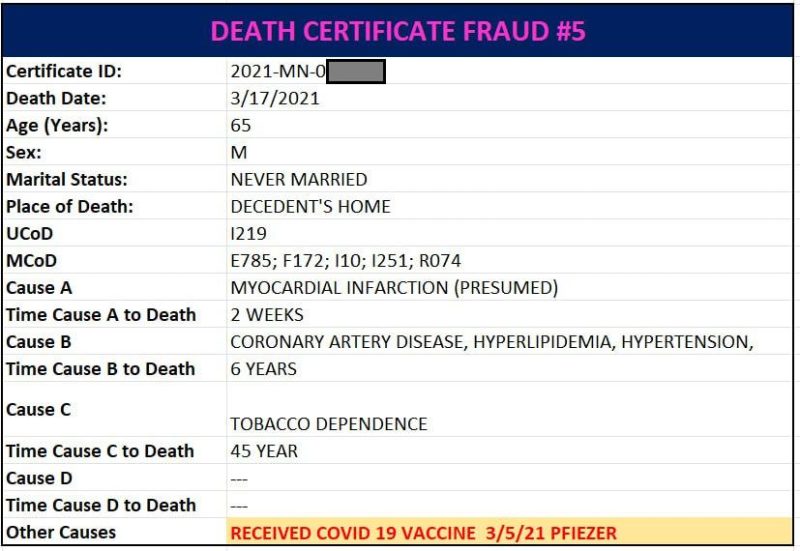
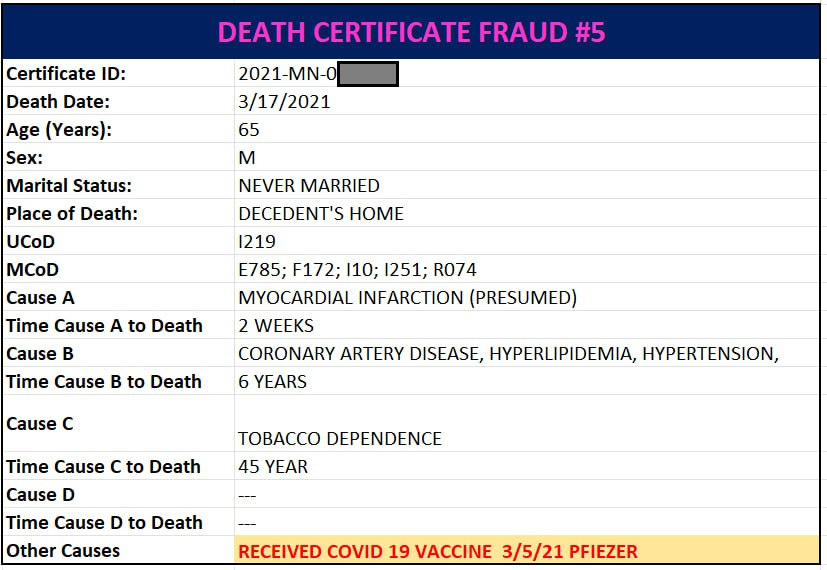
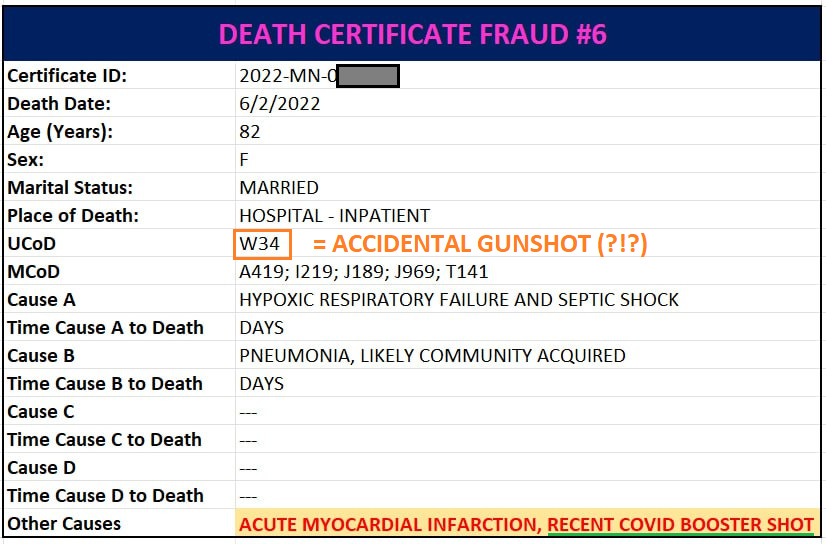
Here we have a 65-year-old male who was killed by a heart attack 12 days after getting vaccinated.
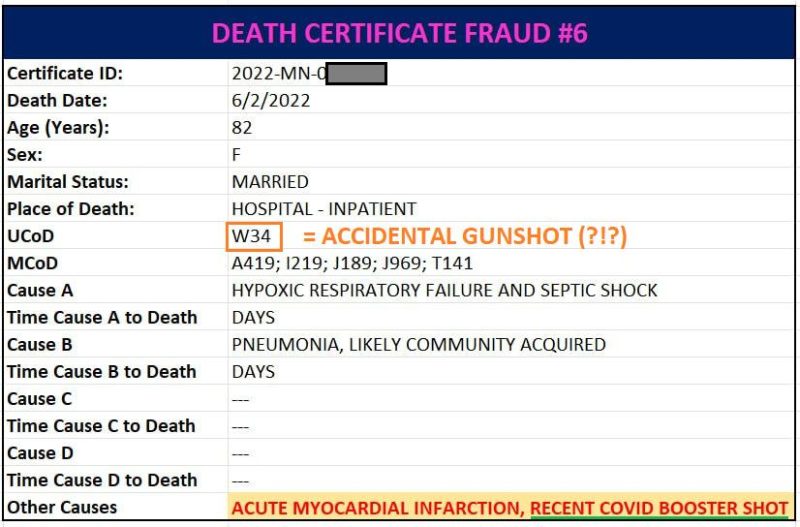
This case is especially noteworthy. Someone involved with this death informed me that the family had to pressure the coroner to put the recent covid booster on the death certificate. A family member also filed a VAERS report themselves, after the patient’s doctors declined to do so.
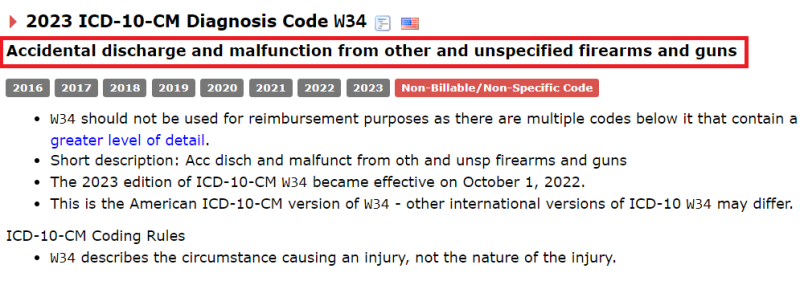
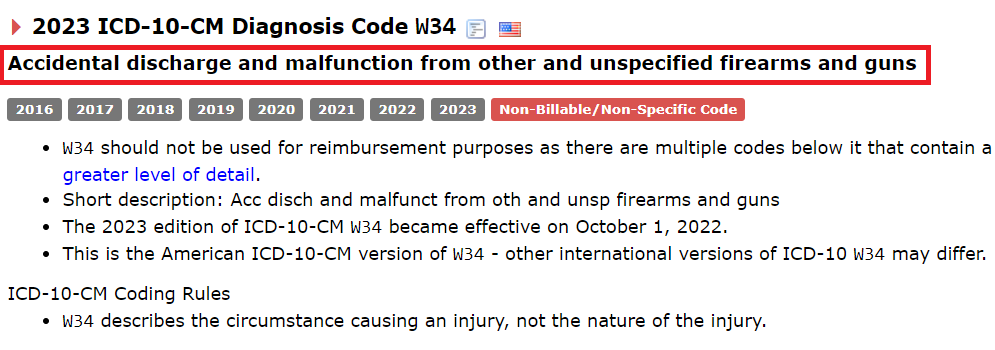
Furthermore, the CDC applied W34 as the UCoD. What is W34 for?
‘accidental discharge and malfunction from other and unspecified firearms and guns.’
There is no mention of any firearms mishaps on the death certificate.
One would have to wonder how such an errant code came to be, especially on a death certificate that contains other ICD 10 shenanigans. It is unlikely that ‘Y590’ or ‘T881’ would be ‘misspelled’ or algorithmically mixed up with ‘W34.’
Perhaps if there were no other instances of fraudulent omittance of vaccine ICD codes on other death certificates, and the CDC wasn’t in the habit of routinely assigning U07.1 for a covid infection that resolved a year ago, the failure to include T88.1 or Y59.0 here could be excused.
At minimum, this death certificate should contain T88.0 – ‘Infection following immunization’ – to document the breakthrough infection (which is a subject for a separate article as this seems to be fairly widespread).
Additional Observations
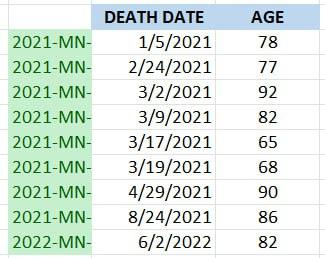
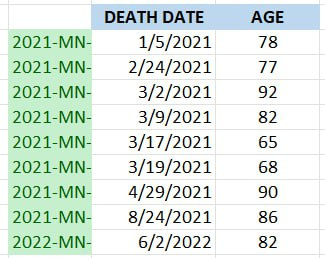
The following table shows the date of death and age for all 9 death certificates shown above that identified a covid vaccine as a CoD:
It is striking that 7/9 died before May 2021. This is odd – if anything, the deaths should skew later, not earlier. Vaccine adverse events were denied – with maximum prejudice and then some – for many months before the medical mainstream has finally (begrudgingly) started to acknowledge that the covid vaccines can trigger potentially lethal pathologies (in exceedingly rare instances to be sure).
The clustering of death certificates mentioning a covid vaccine at the beginning of the rollout suggests that ‘administrative’ interference likely played a role in discouraging coroners from mentioning a covid vaccine on death certificates.
Another noteworthy tidbit here is the age of the decedents: every single one is a senior citizen, and the average age of the decedents is 80. This is important to highlight because whereas young people “dying suddenly” stands out, there has been much less attention or acknowledgement of the covid vaccine’s devastating toll upon the old and frail, where deaths – even those that occur in close proximity to vaccination – are readily attributed to prior health conditions.
Finally, the actions of the CDC call into question whether the CDC is altogether qualified or trustworthy enough to be the steward of the nation’s epidemiological data. The CDC manages many of the datasets that underpin whole fields of study. If the CDC is willing to fraudulently alter data (or even if the CDC is just too incompetent to avoid corrupting data), all data under the aegis of the CDC is potentially suspect, especially if it relates to a controversial political or social issue. The implications of this are disturbing, to say the least.
Mallinckrodt PLC (MNK) shares surged in the extended session Thursday after the Dublin-based drug maker and distributor said it was open to proposed transactions as it keeps delaying a payment under an opioid settlement. Shares rallied as much as 15%, and were last up around 9% in late Thursday activity, following a 5.3% decline top close Thursday at $1.08 a share. Mallinckrodt said its board is "actively evaluating the company's capital needs in light of its obligations under its opioid settlement and its long-term debt, and is considering options, including transactions that have been proposed by holders of various series of the company's indebtedness and other company stakeholders, as well as the viewpoints of various parties in interest." Last week, the company made a late interest payment, as it tries to keep up with payments in a $1.7 billion settlement, and delayed the payment of $200 million once again because of its capital position and financial obligations.
Food delivery apps DoorDash and Grubhub filed suit Thursday seeking an emergency ruling to block a city-mandated wage hike for drivers set to take effect next week, new court papers show.
The controversial pay hike slated for July 12 is part of the City Council’s 2021 mandate on minimum hourly wages for food app delivery drivers.
Under a new plan pushed by the Department of Consumer and Worker Protection, drivers must get paid a minimum of $17.96 an hour — and by April 1, 2025, when the plan is fully phased-in, the minimum hourly pay will be $19.96 an hour. The apps can choose to pay per trip, hours worked or whatever formula that equals an average pay of the minimum wage,
But the food delivery apps argue the plan could amount to their drivers getting paid as much as $33.27 an hour for time spent on an active delivery; they’re suing the agency to block the hike from taking effect.
The apps called the pay raise “onerous” and said it “threatens to single out and punish” DoorDash and Grubhub — and also threatens the industry as consumers will likely have to pay $5.18 more per order, which will hurt restaurants and ultimately hurt the drivers who would wind up with less business, according to a Manhattan Supreme Court lawsuit Thursday.
The hike would “reconfigure the nature of this industry, and squelch innovation and flexibility, by imposing onerous minimum-pay requirements in the name of worker protection — likely harming the very workers they purport to protect,” the suit charges.
The delivery services say the way the city calculated the pay raise was flawed, and also claimed it didn’t properly explain its reasoning.
“Bad policies cannot go unchallenged, and we will not stand by and let the harmful impacts of this earnings standard on New York City customers, merchants, and the delivery workers it was intended to support go unchecked,” a DoorDash spokesperson said.
The apps say the hike is “onerous” and say it will hurt the industry as a whole.UCG/Universal Images Group via Getty Images
“We – and others – clearly and repeatedly warned the city that using such a flawed process to underpin its rulemaking would have lasting and harmful impacts for all New Yorkers who use these platforms, but the approach that DCWP took was sadly not one that reflected this, and has left us no choice but to take our concerns to court,” the statement concluded.
The suit wants a temporary restraining order to block the July 12 hike from taking effect — at least until the entire case is decided. Ultimately the delivery app giants want to overturn the pay hike.
The suit says the food delivery apps are in support of fair pay for drivers but claim a new formula should be used to determine what the minimum pay should be.
The city-mandated minimum wages will be rolled out gradually until 2025.UCG/Universal Images Group via Getty Images “Delivery workers, like all workers, deserve fair pay for their labor, and we are disappointed that Uber, DoorDash, GrubHub, and Relay disagree,” Commissioner Vilda Vera Mayuga said in a statement.
“The minimum pay rate will help uplift thousands of working New Yorkers and their families out of poverty,” the commissioner said. “We look forward to the court’s decision and to apps beginning to pay these workers a dignified rate starting July 12th.”



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}