Despite lawmakers’ success in introducing legislation to address the issue, one U.S. farmer raised a red flag that China is still infiltrating "many, many acres" in rural America.
"They're tapping into the American food structure and this country. And we should be looking at that as food security, people," National Black Farmers Association President John Boyd Jr. said on "Cavuto: Coast to Coast" Tuesday, "because they're tapping into American farms and tapping into the hog industry, all of these industries that China is quietly taking over here in the United States."
Farmers have voiced their concerns for more than two years over Chinese-owned companies purchasing large swaths of rural farmland in states like Oklahoma, Minnesota, North Carolina and Virginia.
U.S. Department of Agriculture (USDA) data from 2021 indicates that China controls an estimated 383,000 acres of U.S. farmland, with their investments reportedly generating $1.9 billion that year.
Chinese-backed companies with big bucks are also outbidding American farmers for new land, according to Boyd Jr.
National Black Farmers Association President John Boyd Jr. claimed Chinese companies are out-bidding American farmers for land on "Cavuto: Coast to Coast" Tuesday, June 27, 2023. (Fox News)
"Persons like myself who can maybe pay $4,000 or $5,000 an acre, some of these farms are being run up to $15,000 and $20,000 an acre," Boyd Jr. explained. "Now, how many American farmers that you know in the United States can afford $20,000 an acre for good farm ground? Because I can't."
The fourth-generation Black farmer criticized the Biden administration for being "asleep at the wheel" as China continues gaining land access adjacent to sensitive infrastructure and military bases.
"While we are losing farms, this administration hasn't done anything to stop farm foreclosures in this country. We have many of our members who are, right now, facing farm foreclosure, but we had $1 billion to help Chinese farmers and other entities in Russia," Boyd Jr. said.
"But they can come over here and purchase our farmland and purchase our infrastructure and tap into the American government here," he added. "Something is terribly wrong with this."
In May, Republicans and Democrats teamed up to introduce a bill that would block foreign adversaries like China from buying U.S. farmland, titled the "Protecting America’s Agricultural Land from Foreign Harm Act."
In addition to stopping people and companies linked to the Chinese Communist Party from buying U.S. farmland, the bill would block similar purchases out of Iran, North Korea and Russia and prohibit actors associated with the oppressive regimes from participating in certain programs directed by the USDA.
According to Congress’ legislative process tracker, a summary of the bill is still in progress and, thus, has not yet passed in either chamber to make its way onto the president's desk.
Boyd Jr. called out lawmakers for working "not aggressively" enough in order to pass and enact the law – and protect farmers, their land and businesses.
"U.S. senators and leaders in Congress, they need to put legislation in place to stop China from buying American farm ground and to stop them from buying American companies, and taking over the United States to quietly put a real strong foothold on the United States," the farmer said. "We’re not doing enough to stop this."
The Supreme Court struck down President Biden's student loan forgiveness plan Friday, adding a layer of uncertainty to those straddled with payments.
For more than three years, federal student loan borrowers have not had to make monthly payments. But that pandemic-era pause is coming to an end this fall, setting up a financial shock for millions of Americans and the big-name stores where they shop.
About 44 million borrowers in the U.S. were affected by the payment pause, which initially began in March 2020 at the onset of the COVID-19 pandemic. The Biden administration extended the pause for the eighth time in November but will not do so again as part of the bipartisan debt ceiling deal approved by Congress.
Payments, which will resume Aug. 30, can be substantial. The average monthly bill hovers between $200 and $299 per person, although it is even higher for some borrowers, according to most recent Federal Reserve data.
Collectively, borrowers will resume paying about $10 billion a month, according to a recent analysis from JPMorgan.
The resumption of these payments will likely force households to cut back on spending in other areas, particularly retail, according to a note from UBS analyst Jay Sole.
"Inflation and the overall macro environment has caused U.S. consumers to defer many discretionary purchases over the past 18 months," Sole wrote in the note. "Apparel has proven to be the category consumers defer most often.
"Interestingly, market research of 1,392 U.S. consumers with student loans shows this trend is even more pronounced among this group. We believe this indicates student loan consumers will reduce spending on apparel in a big way when they have to start paying off their student loan debt."
A number of brands and retailers could be negatively affected by the spending reduction, including American Eagle Outfitters, Carter's, Crocs, Foot Locker, Canada Goose, Gap, Nordstrom, Nike, Steve Madden, Under Armour and Victoria's Secret, according to UBS.
UBS is not alone in its warning of trouble for retail.
JPMorgan analyst Chris Horvers said Target sales could face a hit once student loan repayments begin in early September because Target caters to millennials, who carry a large share of student loan debt.
"Target over-indexes to the millennial customer and, should student loan payments come back on, the company is more exposed than others in our coverage," Hovers wrote in the note. "Buy-side client expectations are in the $6-8 million per month consumer outflow range should this happen, per our conversations, which represents a potential 1-2 point [comparable] headwind to retail spending."
Biden's broader student loan forgiveness plan, which SCOTUS blocked, had proposed the elimination of $10,000 in student loan debt for individual borrowers who earned less than $125,000 in either 2020 or 2021 or married couples who made less than $250,000 annually in those same years. If a qualifying borrower also received a Pell grant while enrolled in school, they would be eligible for up to $20,000 in debt forgiveness.
"There are millions of Americans — millions of Americans in this country who feel disappointed and discouraged, or even a little bit angry, about the court’s decision today on student debt. And I must admit I do too," Biden said Friday afternoon.
The White House plans to push forward a new plan to erase student loan debt.
German scientists have uncovered startling evidence that a substantial portion of the batches of the Pfizer-BioNTech COVID-19 vaccine deployed in the European Union may in fact have consisted of placebos – and that the German regulator knew this and did not subject them to quality-control testing.
The scientists, Dr. Gerald Dyker, Professor of Organic Chemistry at the Ruhr University Bochum, and Dr. Jörg Matysik, Professor of Analytical Chemistry at the University of Leipzig, are part of a group of five German-speaking scientists who have been publicly raising questions about the quality and safety of the BioNTech vaccine (as it is known in Germany) for the last year and a half.
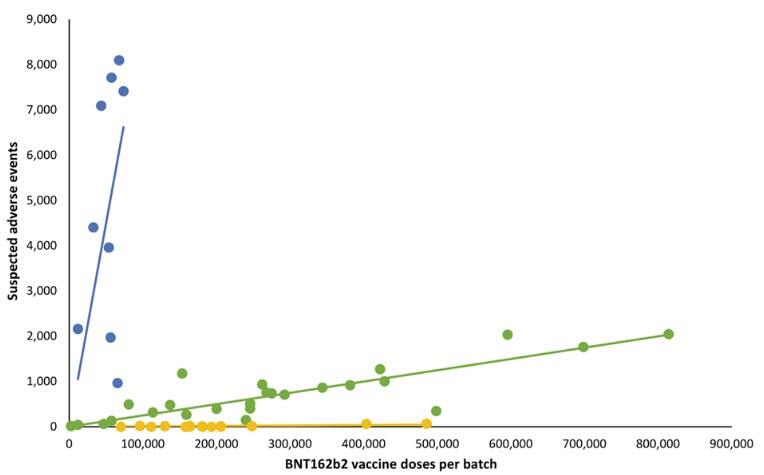
They recently appeared on the Punkt.Preradovic online programme of the German journalist Milena Preradovic to discuss batch variability. Their starting point was the recent Danish study showing enormous variation in the adverse events associated with different batches of the Pfizer-BioNTech vaccine, or BNT162b2 per its scientific codename. The below figure from the Danish study illustrates this variation.
It shows that the batches used in Denmark, which are represented by the points in the graph, essentially break down into three groups.
The ‘green batches’ clustered around the green line have a moderate or moderately-high level of adverse events associated with them. In the discussion with Preradovic, Gerald Dyker takes the example of the green point furthest to the right.
As he explains, it represents the batch that was the used the most in Denmark, with somewhat over 800,000 doses having been administered. These 800,000 doses are associated with around 2,000 suspected adverse events, which gives a reporting rate of one suspected adverse event per approximately 400 doses. As Dyker puts it, “That’s not a small amount if we compare to what we know otherwise from influenza vaccines.” According to Dyker’s calculation, the green batches account for more than 60% of the Danish sample.
There are then the ‘blue batches’ clustered around the blue line, which are obviously associated with an extraordinarily high level of adverse events. As Dyker notes, no more than 80,000 doses of any of the blue batches were administered in Denmark – suggesting that these especially bad batches may perhaps have been quietly pulled from the market by public health authorities.
Nonetheless, these batches had as many as 8,000 suspected adverse events associated with them. Eight thousand out of 80,000 doses would give a reporting rate of one suspected adverse event for every 10 doses – and Dyker notes that some of the blue batches are indeed associated with a reporting rate of as high as one suspected adverse event for every six doses!
On Dyker’s calculation, the blue batches represent less than 5% of the total number of doses included in the Danish study. Nonetheless, they are associated with nearly 50% of the 579 deaths recorded in the sample.
Finally, we have the ‘yellow batches’ clustered around the yellow line, which, as can be seen above, barely gets off the x-axis.
On Dyker’s calculation, the yellow batches represent around 30% of the total.
Dyker notes that they include batches comprising some 200,000 administered doses which are associated with literally zero suspected adverse events.
As Dyker puts it, “malicious” observers might note that “this is how placebos would look”.
And malicious observers might be right.
For Dyker and Matysik compared the batch numbers contained in the Danish study with publicly available information on the batches approved for release, and they made the startling discovery that almost none of the harmless batches, unlike the very-bad and not-so-bad batches, appear to have been subject to any quality-control testing at all.
Unbeknownst to most observers, it is precisely the German regulatory agency, the Paul Ehrlich Institute (PEI), which is, in principle, responsible for quality control of all the Pfizer-BioNTech vaccine supply in the EU. (The institute is named after the German immunologist and Nobel Prize winner Paul Ehrlich, not, of course, the Stanford biology professor of the same name.)
This reflects the fact that the actual legal manufacturer of the vaccine, as well as the marketing authorisation holder in the EU, is the German company BioNTech, not its more well-known American partner Pfizer.
Dyker and Matysik found that the PEI had tested and approved for release all the very bad ‘blue’ batches, the overwhelming majority of the not-so-bad ‘green’ batches, but almost none of the harmless ‘yellow’ batches – as if the PEI knew in advance that these batches were unproblematic.
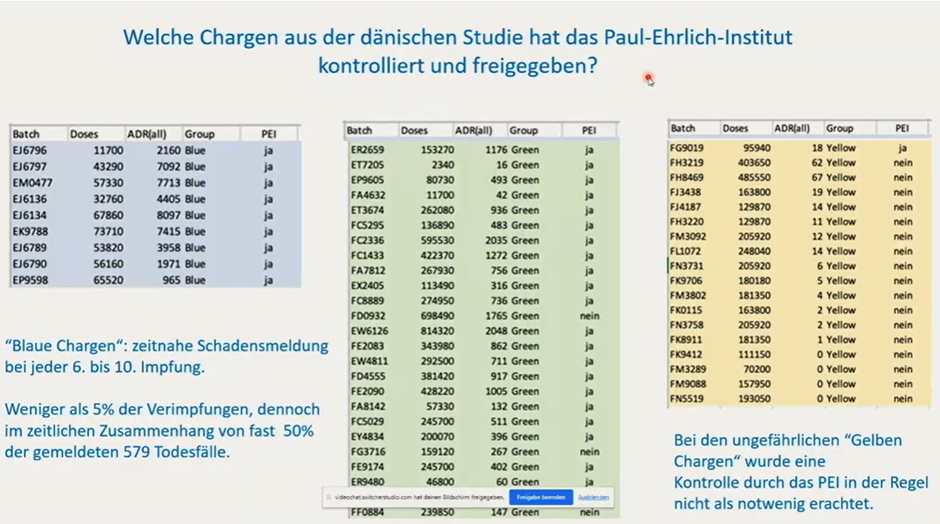
This is shown in the below slide from Dyker’s presentation during the Punkt.Preradovic interview. The title reads: ‘Which batches from the Danish study did the Paul Ehrlich Institute test and approve for release?’
In the PEI column of each of the tables, “ja” means, of course, that the batch was tested, “nein” means that it was not. Note that only the first batch in the ‘yellow’ table was tested.
The caption under that table reads: “The PEI did not generally regard testing of the harmless ‘yellow batches’ as necessary.”
As Dyker put it, with notable restraint, “this would support the initial suspicion that they are maybe in fact something like placebos”.
Or, in short, to paraphrase the German scientists’ findings on the variability of the Pfizer-BioNTech batches, it would appear that the good was bad, the bad was very bad, and the very good was saline solution.
* * *
(The full Punkt.Preradovic interview with Gerald Dyker and Jörg Matysik is available here in German. The above translations are by your writer. A full, presumably machine-translated, English version of the interview is also available on the Punkt.Preradovic webpage.)
Robert Kogon is a pen name for a widely-published financial journalist, translator and researcher working in Europe. Subscribe to his Substack and follow him on Twitter.
Pat Furlong was sitting in her home office in Middletown, Ohio, last Thursday, refreshing a Food and Drug Administration web page ad nauseam, when the phone rang. She answered and burst into tears.
The FDA had just approved the first gene therapy for Duchenne muscular dystrophy, her friend and the therapy’s architect, Jerry Mendell, told her. It was a culmination of advocacy work Furlong began 39 years prior, after her own sons were diagnosed with the fatal muscle-wasting disease.
She thought back to them, Christopher and Patrick, and trips they had taken in 1992 to Memphis, where researchers were experimenting with implanting immature muscle cells into Duchenne patients. She was full of hope then. One of that year’s radio hits was Marc Cohn’s “Walking in Memphis,” and Furlong kept hearing the song’s central line in her head: You’ve got a prayer in Memphis.
Then the study failed. The cells did nothing. Within four years, Furlong had buried both sons, both still teenagers.
“And then yesterday, my thoughts went back there, too,” Furlong said in an interview the morning after the approval. “We have a prayer. You know, it’s not Memphis, but we do have a prayer.”
For Furlong and an entire generation of parents, the approval of Sarepta Therapeutics’ gene therapy, Elevidys, is an ecstatic moment, but one laced with pain. They mobilized for years to lay the groundwork, raising money for basic research, meeting with lawmakers, lobbying the FDA and educating biotech CEOs. Their sons participated in study after study, establishing foundational knowledge both Sarepta and regulators relied on.
Yet largely, those sons will not benefit. Some, like Furlong’s, have died. Others are now in their late teens and twenties and have already lost most of their muscle function.
Sarepta’s gene therapy might help preserve muscle, but it can’t rebuild what’s lost.
“It’s heartbreaking,” said Jennifer McNary, the mom of two men with Duchenne, both of whom rely on wheelchairs.
McNary, whose 2016 lobbying for an earlier, controversial Sarepta drug shifted the agency’s attitude toward rare diseases, calls this group the “legacy moms.” Mindy Cameron, the mom of a 21-year-old man living with Duchenne, calls these older boys and men the “lost heroes.”
“It’s a lot of joy, a lot of pride,” said Cameron, describing her emotions. “But I didn’t pay the ultimate price, my son did. And life is getting hard for him.”
They know there are limits to Elevydis. The $3.2 million drug, designed to deliver a miniaturized form of dystrophin, the gene broken in Duchenne, is not a cure and is only approved for (most) 4- and 5-year-olds, with a broader approval possibly coming for other ambulatory patients next year.
Yet they know it means that if a young boy is diagnosed today, his family will likely not receive the same punch-in-the-gut prognosis they all did: There’s no treatment, take them home, love them, come back when they need wheelchairs.
Their efforts over 30-plus years are a case study in the profound power and limits of modern disease advocacy. Beginning with Furlong, they created one of the most powerful disease movements since the AIDS crisis. That movement birthed a gene therapy for one of the most common rare diseases, something most regarded as science fiction. But science-fiction still came too slow, the pace of drug discovery always trailing the pace of Duchenne.
Nevertheless, many stayed involved through the decision, working with the younger, less experienced parents to help convince the agency they needed access to this treatment.
“This is perhaps the beauty and the pain and all of that of advocacy, right?” said Furlong. “You learn a diagnosis, you join a group that you didn’t want to join, that you didn’t know about, that you’d hope, in retrospect, that you never learned about. And then you become part of that community that wants the best not only for your children, but for someone else, because you’ve seen this.”
Each started in search of a cure for their son, believing they could beat the predictions textbooks laid out for the hundreds of children diagnosed every year.
Pat Furlong reads to her sons, Patrick and Christopher.COURTESY PAT FURLONG
When Furlong began, there were no treatments. There weren’t even clinical trials. She was a former nurse, though. She knew medicine. So she tracked down the scientist behind an old research paper and convinced him to start one. She offered funds from a loan she took out and assured her sons were included.
It failed. Almost everything did. After Memphis, she founded a nonprofit, Parent Project Muscular Dystrophy, to bring the field’s top minds together — and raise the kinds of funds required for better research. She wheedled, pleaded and occasionally lied, telling scientists a top luminary was coming to a conference to make sure they showed up.
And then, in a seven-month-span in 1995 and 1996, both Christopher and Patrick died. She was left in her Middletown home stewing in grief, angry at the world. She was broken, she said. A nurse whom medicine had failed.
The phone rang. It was Lee Sweeney, one of those scientists Furlong had lobbied. Stay, he said, you can do something important.
“It can be your get even strategy,” he told her.
In years that followed, PPMD secured hundreds of millions of dollars in funding for care centers and research, including some of the earliest work on gene therapy. They met with the FDA repeatedly, running surveys and writing guidance documents to explain what the community needed and the risks they were willing to take. When Jerry Mendell was ready to begin testing what would become Elevydis around 2016, Furlong raised the $2.4 million he needed for the trial.
Other moms traced similar arcs. Before Debra Miller started CureDuchenne, a venture philanthropy group, she was just trying to cure her son Hawken, now 26. But as a public charity, they couldn’t focus solely on Hawken and his particular mutation.
“The integrity issue takes over — that I’m not just here for my son, I’m here for all the families,” she said. She’d meet those families and “fall in love with those kids too.”
They grew used to disappointment, to being left behind by companies that shifted focus or concentrated on younger patients. CureDuchenne invested in or gave money to companies developing treatments for Hawken’s mutation. Then they’d pivot to different mutations for business or chemistry reasons and Miller would have no recourse.
Nostrums such as shock therapy and stem cells rose and fell, dividing the community in their wake.
Research trials generated hope but came with strict criteria. Companies wanted patients with the most muscle left to save. Mindy Cameron’s son, Christopher, enrolled in observational studies to help researchers understand the disease for future generations. But he was often just slightly too sick to be eligible for treatment studies.
In 2018, he was rejected from a trial testing a different gene therapy in older boys, and Cameron left Duchenne advocacy.
“It was like getting the whole diagnosis over again,” she said.
She did HIV work for a year and came back.
“I knew too much to do anything else,” she said.
When Sarepta started a trial on a mutation-specific drug in 2011, Jennifer’s McNary’s younger son, Max Leclaire, was eligible for treatment studies. Her older son, Austin Leclaire, wasn’t.
“This has been the theme of Austin’s life,” said McNary.
By 2020, McNary had stepped away from Duchenne work. Her efforts in 2015 to secure approval for that drug despite limited evidence — after she watched Max benefit in a trial, while Austin continued to decline — stoked tremendous backlash but altered the agency’s attitude toward patient demands. Afterwards, she consulted for companies and nonprofits hoping to do the same in other diseases. (She has also consulted for Sarepta.)
She returned after hearing chatter about a Sarepta gene therapy trial for older boys, the earliest in an ongoing effort to obtain wider approval. Per usual, Max was deemed eligible. Austin was not.
When it became clear FDA reviewers were skeptical of the company’s data, noting the only placebo-controlled trial failed (Sarepta attributes it to a study anomaly), she and Furlong worked with parents of younger kids to help the new parents communicate to the FDA how much they believed the treatment benefited their sons.
In May, those parents showed videos at a hearing of outside advisers: Boys with Duchenne walking up stairs with relative ease, riding bikes, playing sports. McNary thought of Austin, who has never once jumped.
“It’s a little bit of a kick in the gut,” she said. At the same time, “you’re so happy for the people who are you? Right? These are younger me. These are people who, you know, deserve all of the happiness.”
Their lobbying and those videos, combined with early data, persuaded FDA biologics chief Peter Marks to overrule his own reviewers and give the drug accelerated approval for a limited age group. Technically, it can be taken off the market if a confirmatory study delivers negative results later this year.
If that study is positive, however, and the agency both keeps the current approval and expands it to older ambulatory boys, advocates expect the community and their movement will change.
Cameron wonders if it’ll fracture. The pre-gene therapy population and the post. She wonders if the next generation will understand what they went through, what they did.
The face of the advocate community will likely change, too, becoming more and more the boys and men themselves.
“Is it still going to be called CureDuchenne? Is it still going to be called Parent Project?” asked Cameron.
That process has already begun, as a broadly improved standard of care has allowed many patients to live into adulthood. For them, knowing a next generation may face different odds has been heartening.
“It’s a whole new world,” said Buddy Cassidy, a 33-year-old man with Duchenne who served as the patient rep on the FDA advisory hearing, adding that he hopes it will help usher in therapies for other rare diseases as well.
At the same time, he has also been working on supporting patients as they transfer into adulthood, assuring they can go to college and receive the services and accommodations they need to live an independent life.
Austin Leclaire, who lives with Max in an apartment attached to McNary’s house, hopes to get the treatment eventually, if Sarepta can secure wider approval. But they know its benefits may be minimal. McNary thinks it might have helped stabilize Max, allowing him to lift groceries and cook.
At 21, Christopher Cameron, needs round-the-clock-care and lacks the muscle strength to blow his nose, but he’s a college student and an aspiring screenwriter and just this month, he and his family got back from an Alaska cruise, as part of his goal to see all 50 states. Mindy doesn’t know if he would get the therapy if it’s ever approved for the non-ambulatory, given the risks it might hold for sicker patients, but she’s glad it’s his decision now, not hers.
Some of the legacy moms are ready to hand off the baton to the next generation of parents and men. The next fight “will take new, less exhausted people,” McNary said.
Others aren’t slowing down. The Parent Project Muscular Dystrophy’s annual conference began Thursday. There is still so much to be done, Furlong said, ticking off a list.
How do they ensure everyone who is eligible gets access to the therapy, particularly boys who will soon turn 6 years old? How do they make it available to people who are currently ineligible because they have antibodies against the virus used to deliver the gene? How do they make it available around the world? How do they make even more effective drugs?
“It’s full speed, full speed, we can slow down when we’re assured that we have treatments for every single individual touched by a dystrophin-related disease,” she said. “Then we can slow down. But I don’t see that happening anytime soon.”
In 1983, I flew home from college to be with my mother as she woke up from a mastectomy. She opted out of breast reconstruction, choosing to “go flat” instead.
When I was diagnosed with breast cancer in 2017 and had bilateral mastectomies, I had more reconstruction options than my mother did.
I chose the option that was the best fit for me: DIEP flap, which uses a person’s own tissue to recreate the breast. Researchers have called it “the gold standard for reconstructive options.” According to a 2017 study, it supports better well-being, has fewer complications, and helps people recover more quickly, with less hospitalization time, compared with other procedures that use muscle tissue. In 2020, more than 23,000 patients — almost one in five people who had reconstruction that year — chose DIEP flap.
But fewer people may have that choice going forward. Recently, at the request of insurance companies, the Centers for Medicare and Medicaid Services has announced that it is ending the medical billing code for DIEP flap. If that change takes effect, most patients won’t be able to get the reconstructive care they need. It’s imperative that CMS retain the code to ensure access to DIEP flap reconstruction.
Breast implants are the most common alternative to natural reconstruction. They are the right choice for some, but not everyone. Implants can cause more health problems, and they are not an option for people who need radiation. Implants also risk complications, including rupture, and require replacement about every decade.
I joke that when I was choosing my breast surgeon, I was Goldilocks — I saw four doctors before finding “the one.” None of the first three asked what I wanted post-mastectomy, nor took time to discuss the pros and cons of different reconstruction procedures. I had to do my own research to discover DIEP flap was an option.
Since 1998, all insurance plans have been required to cover breast reconstruction under the Women’s Health and Cancer Rights Act. The WHCRA has improved access to breast reconstruction: Within two years of the WHCRA becoming law, women’s ability to access breast reconstruction increased by 36 percent. Later studies suggest that, in at least 22 states, reconstruction access continued to rise by 62 percent between 2009 and 2014.
Despite this progress, research shows that there are significant reimbursement disparities between implants and natural reconstruction. Across all forms of insurance, reimbursement rates are higher for breast implants, which are simpler and faster to provide, making them more lucrative for surgeons and saving insurance companies money in the short term.
To better align these financial incentives, in 2006, CMS established a reimbursement code for surgeons to submit to insurers for performing a DIEP flap. It fairly compensated them for providing this more complex procedure. Thanks to this policy and my health insurance, I could afford to choose DIEP flap reconstruction.
Today, in the Washington, D.C., region, where I live, this kind of reconstruction may cost between $11,909 to $27,985 per breast if you don’t have insurance, according to procedure-only cost estimates by FAIR Health. For people with insurance, the out-of-pocket costs drop to about $4,820 to $9,098 per breast. Implants are not as expensive, though again, patients may have to pay for replacement procedures in the future. For those without coverage in the D.C. area, implants can cost $4,195 to $6,276 per breast, falling to $1,804 to $2,022 with insurance.
Now, CMS plans to eliminate the unique code next year, approving a request by the Blue Cross Blue Shield Association. (Blue Cross Blue Shield happens to be my insurer.) The association reasoned that the unique code was temporary, and that other codes should cover this procedure. The problem is that other codes include surgeries that are easier — and cheaper — to provide, so they would not render reimbursements reflecting the complexity of providing DIEP flap. Already, some insurers have announced they will stop reimbursing doctors for it. While the billing code may not require insurers to pay for DIEP flap, it is necessary to give surgeons a greater chance of being paid for their skill and time providing the procedure. It is an important incentive for providers to continue offering DIEP flap to patients.
Without payment for the complexity of the DIEP flap procedure, fewer surgeons will offer it as an option for insured patients. This change has no medical basis and does not reflect the best patient outcomes. Eliminating the code will make this option inaccessible for most people who need breast reconstruction. DIEP flap will become available only to those who can pay for it on their own — and most won’t be able to.
Almost half of adults in the U.S. struggle with health care costs. Breast cancer treatment specifically poses “catastrophic or significant” economic burdens on nearly half of patients. Decades of gender, racial, and economic inequality worsen this insecurity. This DIEP flap access issue will hit Black women the hardest, as we are more likely than other groups to choose it when we seek reconstruction.
Thanks to grassroots advocacy by patients and health care professionals, CMS hosted a public meeting on June 1 to seek input. Feedback from providers and patients was overwhelmingly in support of maintaining the code to ensure access to DIEP flap reconstruction. During the session, agency leaders acknowledged our concerns and appeared receptive to our request. CMS will announce its final decision this August.
I hope agency officials take to heart one main message I heard at the June 1 meeting: Breast reconstruction is a deeply personal issue. Every patient who wants reconstruction should be able to decide, with their doctor, what option to pursue. CMS must preserve the DIEP flap reimbursement code as a vital first step to ensuring we have this control.
In the future, leaders should look to resolve other challenges facing breast cancer patients. For example, patients who have a mastectomy deserve to know about all their options. Do we want to go flat, like my mother, or have reconstruction? If we want reconstruction, what are our choices? I should not have had to interview four surgeons, or rely on my own research, before learning all my options.
I became a patient advocate when my mother was diagnosed. I have mourned loved ones lost and I have cared for fellow survivors. We have our hands full dealing with cancer. We shouldn’t have to fight to keep a benefit we’ve had for nearly two decades, one which is a vital part of quality care.
Lisa D. T. Rice, M.S., is a breast cancer survivor and vice chair of the National Coalition for Cancer Survivorship.
The Florida Department of Health issued a statewide alert after four people in Sarasota contracted malaria in locally transmitted cases, coming a day after the U.S. Centers for Disease Control and Prevention issued a similar notice for Florida and Texas.
“All individuals have been treated and have recovered. Malaria is transmitted through infected mosquitoes,” Florida’s Department of Health stated in a release issued June 27.
The agency stated that ground and airborne spraying that targets mosquitos will be carried out around Sarasota, which is near Tampa, to mitigate transmission.
“Effective treatment is readily available through hospitals and other health care providers,” the department stated. “Individuals in this area with symptoms of fever, chills, sweats, nausea/vomiting, and headache should seek immediate medical attention.”
It also advised the public to control the breeding of mosquitoes by eliminating any standing water, which is where mosquitoes lay their eggs.
This close-up photograph shows a mosquito in Montlouis-sur-Loire, central France, on Oct. 21, 2022. (Guillaume Souvant/AFP via Getty Images)
“Drain water from garbage cans, house gutters, buckets, pool covers, coolers, toys, flowerpots, or any other containers where sprinkler or rainwater has collected,” the alert said.
Locals should also take precautions while outdoors by using bug spray, avoiding infested areas, and wearing long sleeves and pants if possible.
Malaria is caused by a parasite, Plasmodium vivax, that spreads via mosquito bites, with the largest number of deaths occurring in tropical places such as sub-Saharan Africa. Malaria can be transmitted only by infected mosquitoes, not other people.
Symptoms include chills, fever, tiredness, headache, muscle aches, vomiting, diarrhea, and nausea, and anemia and jaundice may also occur. If left untreated, infected individuals could develop more serious complications and die.
According to the World Malaria Report, released by the U.N. World Health Organization, there were about 247 million cases of malaria in 2021, while the estimated death toll for that year was 619,000. The WHO African Region had the highest share, accounting for about 95 percent of cases and 96 percent of deaths, it said.
Malaria was mostly eliminated in the United States in 1951 after officials sprayed the pesticide DDT and drained swamps in rural areas. DDT was ultimately banned in 1972 in the United States but is still used in African countries.
CDC Issues Notice for 2 States
Earlier this week, the Centers for Disease Control and Prevention (CDC) stated that the cases in Florida and one in Texas mark the first local spread of malaria in the United States in about 20 years.
For the first time in nearly six years, health reform legislation that’s friendly to patient choice, transparency, and market competition has passed the House of Representatives.
It was nearly six years ago when late Sen. John McCain tragically gave a thumbs down to continuing the process of advancing patient-centered health reform legislation when he shut down the Repeal and Replace effort.
Nancy Pelosi controlled the gavel for four years, but now that Speaker Kevin McCarthy is in charge, he and dozens of other House leaders are seizing the health reform agenda once again with fresh ideas and a new approach.
Two measures are teed up, appropriately acronymed PATIENT and CHOICE.
On June 21, the House of Representatives passed the CHOICE Arrangement Act (stands for Custom Health Option and Individual Care Expense arrangements). The bill was jointly drafted by the Ways & Means and the Education and the Workforce committees to expand more affordable and flexible health coverage options, including codifying and expanding Association Health Plans and Health Reimbursement Arrangements. It passed 220-209.
One reason for this progress is that the legislative process is going through “regular order” for the first time in years.
That means that a Member proposes a legislative idea, hearings are held, and the relevant subcommittee considers and reports the bill to the full committee. The full committee then debates the measure and, if approved, it goes to the Floor for a vote, after passing through the Rules Committee which decides the process for offering amendments.
This is what’s happening now, straight out of Civics 101.
Strong-Arm Nancy Pelosi didn’t do it this way. Legislation emitted from the Speaker’s office, and Members were expected to fall in line.
Debate in this session of Congress is more raucous, granted, but it also is much more engaged and productive. The new strategy seems to be paying off.
The three major committees with jurisdiction over health policy issues have produced a dizzying number of smaller bills, many with bi-partisan support, that are combined into these larger bills to advance choice and competition in the health care space. How refreshing it is!
That said, health care clearly has moved off center stage, but that ironically presents an opportunity to get more done. We’re not talking about a big Repeal and Replace effort—which never would pass in the Senate and probably not the House at this point—but rather a series of important improvements that, together, can lead to meaningful change.
How much of the legislation will get through the Democrat-controlled Senate? Hard to know, but the House is engaged in the health care space to tee up bills that will make positive changes when/if the political forces are favorably aligned.
So just to give you a sense of the action taking place and bills that are being moved forward, here is a bit more detail:
The Ways and Means and Education and the Workforce committees worked together to send four important health reform measures to the floor for passage.
The CHOICE Act recognizes the difficulties small businesses have in providing health coverage to their workers and gives new options to businesses in vulnerable small group markets. The bill includes the Self-Insurance Protection Act and would codify access to more, and more affordable, insurance coverage options through Association Health Plans.
It also would codify and improve the Individual Coverage Health Reimbursement Arrangements that would allow employers to give employees more options of selecting health coverage outside the workplace with tax-preferred dollars.
Energy and Commerce Committee: The PATIENT Act that is expected to hit the House floor after Congress returns from recess incorporates 15 separate sections focusing primarily on lowering health costs, including:
Requiring hospitals, health insurers, and clinical diagnostic laboratories to make accessible price information available to patents and consumers
Addressing ownership arrangements in the health sector that are creating monopolies across the nation that eliminate competition and increase costs
Lowering drug costs by protecting patients from complex and hidden pricing practices.
“One of the greatest challenges the health care market faces is rapid consolidation, which obscures the prices and quality of services. Thanks to Federal Government overreach, Americans are missing new opportunities to increase innovation, raise the quality of care, and access affordable drug prices,” said Chairman Bob Good, R-VA. “Patients and consumers should have all the information necessary for them to make the best health care choice possible.”
So the drought has ended. Conservatives are engaged and focused on health reform—building on the strong platforms already in law and expanding options for patients and employers. Hopefully the Senate will see merit in these initiatives and follow suit.
Grace-Marie Turner heads the Galen Institute which has been working for more than 25 years to promote policies that put doctors and patients in charge of health care decisions.




{kind=link}