The World Health Organization has recommended dropping a component of many flu vaccines because the viruses it protects against appear to have beendriven into extinctionin the Covid-19 pandemic.
A family of viruses known as influenza B/Yamagata has not been seen since March 2020, when flu circulation worldwide declined to very low levels in the face of the onslaught of Covid and the protections people took to avoid contracting it. Flu transmission eventually resumed, but of the tens of thousands of influenza B viruses detected and subtyped in the years since, B/Yamagata viruses have not been seen.
“Right now there really isn’t any benefit to having Yamagata in the vaccine,” said David Wentworth, director of the WHO’s Collaborating Centre for the Surveillance, Epidemiology and Control of Influenza at the Centers for Disease Control and Prevention, who was on the expert panel that made the recommendation.
The decision was applauded by influenza virologist Florian Krammer, of Mount Sinai School of Medicine in Manhattan. “Why would you include something that’s not around?” he asked.
The recommendation was made following a weeklong meeting of flu experts from around the world who gather twice a year at the WHO to study circulating flu viruses to advise on what future versions of flu shots should protect against. This week’s meeting was to recommend what viruses should go into the 2024 Southern Hemisphere’s winter shot.
In addition to the fact that there is no benefit to including B/Yamagata viruses in the vaccine at this point, there is a theoretical risk of doing so, a report from the meeting noted. Manufacturers must grow B/Yamagata viruses for inclusion in the vaccines. In most flu shots — the types that are injected — those viruses are killed at a point in the manufacturing process. But a leak from a manufacturing plant could theoretically release B/Yamagata viruses into the world. Likewise, the intranasal flu vaccine FluMist — made by AstraZeneca — contains live but weakened flu viruses. Those viruses, too, could theoretically reintroduce the virus family to the world.
The committee urged regulatory bodies to work with flu vaccine manufacturers to remove the B/Yamagata component from vaccine formulation “as soon as possible.”
“Here we’re balancing the absence of circulation of the B/Yamagata lineage virus with a theoretical risk that we are manufacturing and using a component that’s not necessary,” said Kanta Subbarao, director of the WHO’s Collaborating Centre for Reference and Research on Influenza at the Peter Doherty Institute for Infection and Immunity in Melbourne, Australia.
B/Yamagata viruses haven’t been seen since late March 2020. The rapid and global implementation of social distancing measures, masking, and the profound early reduction in international travel resulted in a substantial reduction in flu transmission. There was virtually no flu season in the winter of 2020-21.
“The other ones — H1, H3, and Victoria — made it through. But there was also a huge bottleneck and Yamagata was not lucky enough to make it through,” said Krammer.
For many low- and middle-income countries, the recommendation will not lead to any change. Many still use trivalent vaccine — a three-in-one shot that protects against influenza A viruses H1N1 and H3N2, plus one of the flu B viruses. In recent years, that would have been the B/Victoria lineage, the only B viruses still circulating.
In countries that moved to quadrivalent flu vaccines a number of years ago, the recommendation may lead to changes in flu vaccine manufacturing, but it won’t be immediate, the experts warned at a press conference the WHO called to announce the outcome of the week’s discussions. Changing the composition of a vaccine requires regulatory approval, which in the case of the United States means signoff from the Food and Drug Administration.
Wentworth said the FDA has been discussing the possibility of recommending removal of the B/Yamagata component from flu vaccines. But whether that’s easy or difficult to do will depend on whether flu vaccine manufacturers still have licenses for former trivalent formulations. STAT reached out to the FDA for comment on the issue, but has not yet heard back.
“Basically it’s going to be different between different companies — whether or not they retained their trivalent license and in which form it was retained, and whether their processes have changed, even though they have their old license,” Wentworth said. “It’s not something that you can do in one day. It’s going to take time. And that’s why our suggestion was to really forecast to the manufacturers and the regulatory authorities that they can start working on this process and try to expedite the process where it makes sense, for safety, etc.”
The experts stressed there is no disadvantage to individuals of getting a quadrivalent vaccine at this point, but no advantage from the B/Yamagata component either.
The flu shots currently used in the United States employ a quadrivalent formulation.
Next week, 50 medical experts from the Karolinska Institutet in Stockholm will meet to award the 2023 Nobel Prize for Physiology or Medicine. The vote takes place on Oct. 2, but betting-minded scientists are already beginning to make their picks for who might take home the gold.
Seasoned Nobel prognosticators will point out that the medicine prize often cycles between super-basic molecular biology and inventions that actually cure people. Last year’s award for paleogenomics falls more toward the former, suggesting an advance with a more clinical focus could well be in the Nobel Assembly’s sights this year. There are many compelling candidates, including the mRNA technology that helped halt the Covid-19 pandemic. But the explosive impact of metabolism-correcting, weight-moderating drugs like Ozempic, Wegovy, and Mounjaro also has some prize forecasters wondering if perhaps the discoveries that have led up to these treatments might find their way to the Nobel spotlight.
Maybe that’s just recency bias talking. These drugs, based on the GLP-1 hormone, seem to be everywhere at the moment — helping people control their diabetes and lose weight, and offering hope that they might also reduce the risk of cardiovascular disease or even, one day, treat drug and alcohol addiction. Many researchers STAT has spoken to in recent months while covering this medical revolution have noted that it has Nobel promise, if not this year, then sometime soon.
Then the question obviously becomes, who gets it? These blockbuster drugs didn’t appear overnight. The journey from discovery of the GLP-1 hormone to treatments for diabetes and then obesity was a long and stuttering one, spanning more than four decades and involving hundreds of researchers across academia and the pharmaceutical industry.
“Certainly this class of drugs, both what they’ve already done and their potential, is enormous and worthy of a consideration around these large prizes,” said Randy Seeley, director of the Michigan Nutrition Obesity Research Center, who has followed the development of these drugs and has consulted for companies making them. But “how you attribute credit is really complicated.”
Other prestigious awards have already gone to a trio of scientists involved in generating some of the earliest insights about the GLP-1 hormone. Historically, the Nobel Prize Assembly has also tended to lean toward honoring basic research. And, as critics have pointed out over the years, by elevating just one, two, or at most, three researchers, the Nobels distort the history of science “by personalizing discoveries that are truly made by groups of individuals.”
That reality hangs heavy especially over a decision about GLP-1 and other gut-hormone based drugs, given how much additional science had to be done to convert the hormones to effective, and then even more effective, drugs. All of the steps from discovering the hormone, to the translational work, to making the drugs “were necessary to get us to the place that we are,” Seeley said. “Which was the hardest, which was the most innovative? I don’t know.”
There was also a lot of luck along the way, like the finding that targeting GLP-1 receptors could lead to substantial weight loss. And there’s no way to assign credit for that. “We’re doing things with these drugs that don’t mimic the biology,” said Seeley. “So understanding the biology alone didn’t get us there, but it was absolutely necessary before we could move on to the next phase.”
Each new leap in understanding may not be prize-worthy in isolation, but with each one, the door cracked open wider, expanding the number of people who could benefit from GLP-1 and other gut-hormone-based treatments. And that, Nobel or not, is worth understanding.
Fish guts and rat organs: The discoverers of GLP-1
It was the summer of 1979. “My Sharona” was on all the radio stations, Ridley Scott’s “Alien” had just premiered, and off the coast of Cape Cod, a deep-sea trawler was on the hunt for a slimy creature of another kind: the American anglerfish.
Much to his relief, Richard Goodman didn’t have to go out in a boat to nab his wide-mouthed quarry. By the time he arrived in Woods Hole, after a two-hour drive from Boston, a local fisherman would have a handful of the slick-skinned seabed dwellers lined up and waiting for him on the docks at the Marine Biological Laboratory. One by one, the spectacled young doctor carefully sliced them open with a scalpel, then from the sticky tissue surrounding their guts, plucked out dozens of lima bean-sized lumps of flesh and dropped them into a flask of liquid nitrogen. Inside each one was an endocrinologist’s goldmine: hundred of thousands of copies of the instructions for making metabolic hormones.
Only a few years before, scientists in Boston and California had come up with revolutionary new techniques for isolating genes and finding out how they worked. Recombinant DNA technology promised to bring bodily processes into molecular resolution, and biomedical research labs all across the country were rushing to learn these freshly minted methods. The lab where Goodman worked at Massachusetts General Hospital was one of the top places applying them to the study of hormones, and its leader, Joel Habener, had amassed serious funding to go after as many as possible.
The new technology made it possible to take mRNA — the messages cells use to produce proteins — and turn it into DNA, which could then be sequenced, and even spliced into bacteria to create biomolecular factories. It turned a six-month process into something you could do in an afternoon. The trick, though, was you needed a lot of mRNA.
Goodman was interested in a hormone called somatostatin, which is produced in the brain and the pancreas. But the brain proved too noisy; too many other peptides being produced. The pancreas was better — it only made a few things besides somatostatin, namely insulin and glucagon and only in one kind of cell, the islet cells. In humans and other mammals, the islets, true to their name, are dispersed throughout the pancreas like a far-flung archipelago. It might take months just to get enough mRNA to start experiments.
So Goodman turned to the anglerfish, which conveniently packs its islet cells into fleshy packages called Brockmann bodies that are big enough to be visible to the human eye.
Pretty soon he was growing colonies of bacteria spliced with bits and pieces of fish DNA and screening them with radioactive probes to identify the one carrying the gene for somatostatin. Not long after he’d successfully done that, a new postdoc named P. Kay Lund with an interest in gut peptides arrived in the lab. Using Goodman’s anglerfish DNA-containing bacterial library, Lund identified for the first time the genetic sequence for the precursor to glucagon, a hormone that increases blood sugar. But she and Goodman soon realized the sequence didn’t stop there.
What they had discovered, and published in a 1982 paper, is that the gene for the glucagon precursor actually contained the code for three peptides: glucagon, and two novel hormones expressed in the gut. A year later, a team led by Graeme Bell at Chiron Corporation in California cloned and sequenced the versions found in humans and other mammals, which they dubbed GLP-1 and GLP-2, for glucagon-like peptides.
Goodman describes his own contributions to the GLP-1 story as “trivial.” During that early era of molecular biology, people were identifying new genes and peptides all the time. The really profound thing, he said, was to make the next leap and ask, “What does GLP-1 actually do?”
There were a couple of groups of researchers, some in Boston and some in Denmark, who jumped.
In 1983, Svetlana Mojsov, a chemist with a background in glucagon and an interest in GLP-1, joined Mass General’s endocrine unit. An expert in peptide synthesis, she hypothesized that the active structure of GLP-1 was actually a smaller fragment of the full molecule, a truncated version she called GLP-1(7-37). In a series of laborious experiments with rat tissues, she discovered that this molecule naturally existed in the gut, right where she expected it to be.
Starting in 1964 with Neil McIntyre’s seminal study at Hammersmith Hospital in London, researchers had observed that when people eat sugar, they experience higher insulin levels than when they get sugar injected into their bloodstream. This suggested that the gut must secrete an insulin-stimulating substance in response to meals. In the 1970s, researchers identified a hormone called GIP they thought fit the bill, but it turned out not to be the full story. With GLP-1 (7-37), Mojsov believed she had found the so-called “missing incretin.”
As she was writing up a paper on these findings, a postdoc in Habener’s lab, Gerhard Heinrich, reached out to her. He had more data on the genetic sequence and wanted to combine their findings, which they did in a paper published in September 1986.
Meanwhile, Mojsov had also begun supplying peptides and other reagents to another Habener postdoc assigned to unraveling the GLP-1 mystery, an endocrinologist named Dan Drucker. He had also found GLP-1 (7-37) in experiments in cell lines. In February of 1987, Mojsov, Weir, and Habener published another paper showing GLP-1(7-37) stimulated insulin secretion in rat pancreases. Drucker’s data were published a few months later, in May. (Mojsov’s contributions were downplayed for decades, but she’s now started to fight for recognition.)
Around this same time, a University of Copenhagen team led by Jens Juul Holst published a report that came to the same conclusions.
The Danish team’s first experiments were failures. When they synthesized a peptide from the newly discovered GLP-1 gene sequence and dripped it into the isolated pancreas of a live pig, nothing happened. Puzzled, they turned to a colleague, Thue Schwartz, who had recently returned to Copenhagen from a postdoc with Donald Steiner at the University of Chicago, where he learned the same types of peptide sequencing techniques Mojsov excelled in. There, he had discovered a hormone called pancreatic polypeptide, which had a rather unique cleavage pattern. He hypothesized that something similar might be happening with GLP-1, which he and Holst said led the Danish group to independently hone in on the 7-37 fragment.
From all the data the two groups had gathered, GLP-1, specifically the 7-37 version, was starting to look like a big deal. If it was really and truly a hormone that could increase glucose-dependent insulin secretion, then it had potential to treat diabetes. The big test would be to put it into people. And that wound up happening faster than any of the researchers involved in its initial discovery ever expected.
According to Holst, in the summer of 1987, he attended a party with Stephen Bloom, an endocrinologist then at Hammersmith. And whether it was the drinks or the belief that his team had a big enough lead that someone like Bloom, who’d never worked with GLP-1 before, couldn’t catch up, Holst spoke freely about the molecule’s therapeutic potential. Not six months later, in December of that year, Bloom’s team had proof that GLP-1 had passed the first big test.
For the generation of biotech executives who presided over the burgeoning industry’s first few decades, GLP-1 was the multibillion dollar idea that got away. Some tried and failed to turn it into a drug, most didn’t even get that far, and almost no one saw the gila monster spit coming.
In the summer of 1980, a young gastroenterologist named Jean-Pierre Raufman arrived at the National Institutes of Health eager for an interesting fellowship project. He got paired up with John Pisano, a somewhat eccentric biochemist known around the NIH for his collection of venoms — many of which he acquired from local amateur zoologists responding to his ads in the Washington Post with plastic bags filled with buzzing wasps and hornets.
Pisano sent Raufman on a venom-mining expedition, which yielded about 20 of his most intriguing samples, including from vipers, cobras, and the gila monster, a large black lizard native to the American Southwest that chews the venom in its saliva into victims with powerful jaws and deeply grooved teeth.
Raufman’s job was to drip these poisons one at a time into dishes of guinea pig pancreas, and then measure how much of a carb-digesting enzyme called amylase the cells secreted. The idea was to find substances that might be able to alter human physiology. “I didn’t know if there would be anything in it, but it certainly sounded intriguing,” he said.
After seeing the gila monster venom spur a huge spike in amylase, Raufman began to focus on better understanding exactly what was in it. Over the next few years he and his collaborators at NIH identified several new peptides and hormones they published in obscure journals.
Out of the gila monster venom they fished out a 39-amino acid peptide they named exendin-4.
Exendin-4 was totally new to science and yet curiously familiar. It was shaped almost exactly like GLP-1. But unlike GLP-1, which lasts less than a minute in the bloodstream before degrading, exendin-4 remains active for more than two hours. It was, they thought, a recipe for a potential blockbuster of a diabetes drug. But in the ’90s, they found themselves a bit ahead of their time.
That somebody was a small San Diego-based biotech startup named Amylin Pharmaceuticals, led by long-time former Eli Lilly veteran, Joseph Cook. Amylin licensed Eng’s lizard peptide in 1996, and developed a synthetic version, exenatide. Within three years, its studies found that one week of exenatide in diabetic mice could normalize blood glucose levels.
Further clinical testing showed it to be both effective and safe. In 2005, exenatide received FDA approval to treat diabetes under the name Byetta. It was a huge hit.
In blogs and early online communities, users adoringly referred to the drug as Lizzie, or Gilly — homages to its reptilian origins — as they waxed rhapsodic about its ability to not just control their blood glucose, but also melt pounds off their bodies. Gray markets sprang up to supply Byetta as a fad-diet drug, a preview to the current Wegovy and Ozempic craze.
But the important thing is that the little gila monster peptide had shown that GLP-1 receptor agonists were a viable approach for treating diabetes. “It gave the field the confirmation that we were on the right track,” said Holst.
By then, Danish pharmaceutical company Novo Nordisk had already begun a clinical trial of its own GLP-1 receptor agonist, which went by the name liraglutide. Scientists within the company believed it could be better than Byetta, and though they were testing it as a diabetes treatment, internally, they were discussing its potential for an even more widespread public health concern: obesity.
At the Hagedorn Research Institute, an academic center embedded within Novo Nordisk, a cell biologist named Ole Dragsbæk Madsen had been giving rats tumors made from islet cells to study how the cells matured and turned on insulin gene expression. But then something disturbing happened. As the animals got older and the tumors got larger, the rats began to eat less and less until they had wasted away completely.
It was as though the tumors were emitting an appetite suppressant powerful enough to kill. When Madsen’s team inspected the tumors, they found they were pumping the animals with huge amounts of GLP-1.
Lotte Bjerre Knudsen, a Novo Nordisk researcher, saw that data and thought that GLP-1 looked like it turned off appetite just as well as it could crank up insulin secretion. “So I was thinking, why on Earth shouldn’t I suggest that you could actually do both of those things at the same time with one drug?”
The winning molecule, called liraglutide, entered clinical testing in 2000 as an injectable drug to treat diabetes, and would eventually be approved by the FDA, as Victoza in 2010. But even as far back as 1995, as Knudsen’s team was screening some of their early designs in mice, they saw that in addition to increasing insulin secretion, GLP-1 agonists made them eat less.
In the mid-1990s, there was a lot of debate about what was behind this effect. Researchers had been finding GLP-1 receptors in places outside the pancreas — including the vagal nerve, which connects the gut to the brain. Based on human experiments, Holst hypothesized that GLP-1 caused slower emptying of the stomach, which sent a signal through the vagal nerve signifying fullness.
The FDA approved liraglutide as Saxenda in 2014 and semaglutide as Wegovy in 2021. Knudsen, who is now a chief scientific adviser at Novo Nordisk, told STAT that based on mouse studies her team has conducted, the more dramatic weight loss is most likely a result of the fact that semaglutide’s chemical structure makes it easier to slip into the brain, particularly into areas involved with signaling feelings of fullness.
While the exact mechanism behind Wegovy’s effectiveness remains a bit murky, the impact of the drug is already clear. Wegovy has generated demand so explosive it has promptedmanufacturing shortages,insurer pushback, andsocial media banson celebrities and influencers promoting it. In 2022, prescriptions in the U.S. for Wegovy, Ozempic — which is approved for diabetes but often prescribed off-label for weight loss — and similar obesity drugshit 9 million.
Cultural mavens have dubbed this the age of Ozempic and Wegovy, but actually, the treatments are already starting to fade. Pharmaceutical companies are quickly moving past drugs that target just GLP-1 and now going after additional hormone targets in the hopes of achieving even greater weight loss.
Eli Lilly’s Mounjaro, which is awaiting regulatory approval to treat obesity, activates receptors for GLP-1 and a similar hormone called GIP and leads to about 20% weight loss. Lilly is also developing a “triple G” drug, which additionally targets glucagon. It induced 24% weight loss in a recent trial, the greatest amount seen yet with an obesity treatment.
This next frontier of obesity drug development stems in large part from the work of Matthias Tschöp and Richard DiMarchi.
Fast forward to 2003. Tschöp was newly an associate professor of medicine at the University of Cincinnati when he received a phone call from DiMarchi, an experienced peptide chemist. They had met at Lilly, where DiMarchi was the executive responsible for endocrine research. DiMarchi had just left the company and become a professor of chemistry at Indiana University, and also wanted to develop obesity treatments that combine multiple drug targets.
They began a two-decade-long collaboration, with DiMarchi making new compounds and Tschöp conducting biological tests.
They started with a list of over a dozen gut hormones that could be potential targets. One that they homed in on was glucagon.
DiMarchi and Tschöp continued to probe other combinations, and another hormone they settled on was glucose-dependent insulinotropic polypeptide, or GIP.
GIP is similar to GLP-1 in that it’s considered an “incretin,” a gut hormone that triggers insulin secretion, but products based on GIP had disappointed as drug candidates for diabetes. Additionally, there had been data showing that mice with GIP receptors knocked out didn’t gain as much weight on a high-fat diet, suggesting to the field that blocking GIP could be a way to treat obesity.
Still, the researchers wanted to try to activate GIP. DiMarchi created new dual agonists, targeting GLP-1 and GIP receptors, and in mice, they found these compounds to be more effective at weight loss than existing drugs that target just GLP-1. The dual agonists also lowered blood sugar and increased insulin secretion in mice, monkeys, and humans. The results suggested that activating GLP-1 receptors could be “the gate opener for releasing additional GIP power,” Tschöp said. This study was published in 2013.
Similar to the story of GLP-1 drugs, the weight loss effects of targeting glucagon and GIP could have only been achieved with drugs that could chronically activate hormone receptors across the body, drugs with effects that are more potent and widespread in the body than the natural hormones that are secreted. That shows how important a role chemical formulation and drug design play beyond just understanding the biological effects of natural hormones, DiMarchi said.
“If we had similarly invested in the chemical optimization of other endocrine hormones, would we have similarly gotten spectacular results? How much has been left on the cutting [room] floor because the tests were with molecules that were not suitably optimized to show what we’ve seen with the state-of-the-art medicinal agents?” he said. “That is the huge opportunity that is before us right now.”
The release of commodity market-sensitive reports released by the U.S. Department of Agriculture (USDA) and other government agencies will be suspended if Congress fails to provide the government with funding for the fiscal year starting Sunday.
During shutdowns, nonessential government employees are typically furloughed, or placed on temporary unpaid leave. Workers deemed essential, including those dealing with public safety, food safety, and national security, keep working.
Private exchange operators such as the CME Group are generally not affected. But routine government reports have in the past been delayed until the government reopens.
"Market reporters will pause USDA's market news reports that help farmers, ranchers, commodity traders, and buyers determine the market value of goods, creating uncertainty in the marketplace with detrimental ripple effects for farmers who need to sell their products," a USDA spokesperson said.
Below is a schedule of key reports planned for release in October and how they may be affected, depending on how long a shutdown lasts.
Monday, Oct. 2:
Weekly U.S. grain export inspections data, released by USDA's Agricultural Marketing Service each Monday at 11 a.m. ET (1500 GMT), will not be published, according to the USDA spokesperson. Inspections reports were released during the 2019 shutdown as some personnel continued to work.
Monthly reports on U.S. grain crushings and fats and oils, including U.S. soy crushings, released by USDA's National Agricultural Statistics Service (NASS) on the first business day of each month at 3 p.m. ET (1900 GMT), would also be suspended.
A weekly U.S. crop progress report, released by USDA's NASS each Monday at 4 p.m. ET (2000 GMT), would be suspended, according to the USDA spokesperson. Farmers and traders rely on the report for harvest progress and crop condition data.
Wednesday, Oct. 4:
The U.S. Energy Information Administration said on Friday that a government shutdown would not have any immediate impact on the release schedule for its weekly oil inventory data, which includes figures on production and stocks of corn-based ethanol. The EIA releases its report each Wednesday at 10:30 a.m. ET/1430 GMT.
Thursday, Oct. 5:
Weekly U.S. export sales data, released by USDA's Foreign Agricultural Service each Thursday at 8:30 a.m. ET (1230 GMT), would be suspended. Multiple weeks of export sales data delayed by two previous government shutdowns were later released in single, combined reports once the government reopened.
USDA Under Secretary for Trade and Foreign Agricultural Affairs Alexis Taylor told reporters on Thursday the export sales report "is not produced while the government is shut down." Taylor said the report "is a critical tool for market intelligence for our exporters and for our industry in the United States."
Friday, Oct. 6:
The U.S. Commodity Futures Trading Commission's weekly Commitments of Traders reports, which detail the size of positions in options and futures, will not be published if there is a shutdown, a CFTC spokesperson said. When the reports were disrupted during the last shutdown, CFTC backfilled the data over a period of weeks after the government reopened. Released each Friday at 3:30 p.m. ET (1930 GMT).
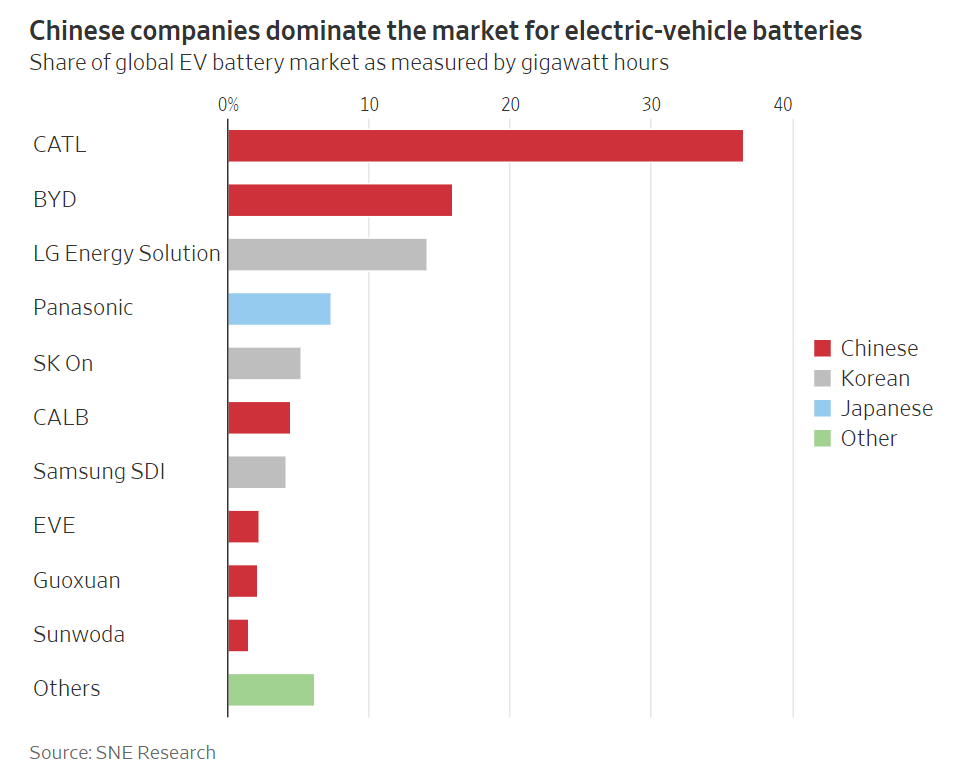
In a battle between GM and Ford, $7,500 in tax credits are at stake depending on Biden’s definition of “foreign entity of concern.” The exclusion aims to reduce US reliance on Chinese batteries and materials to make them.
EV image from SNE Research via the Wall Street Journal
In June, Ford Chief Executive Jim Farley pitched visiting members of Congress on the company’s plans for a $3.5 billion battery factory. Using Chinese battery technology at the Michigan plant, he argued, was a smart way for the U.S. to catch up with China’s expertise.
Later the same day at the General Motors CEO Mary Barra and her team had a different message for the lawmakers: Ford’s plans could be the harbinger of Chinese domination of U.S. car manufacturing.
Ford, with its plans to license Chinese technology to make cheaper, iron-based batteries in Michigan, has lobbied for a more flexible interpretation of the “foreign entity” rule. If its planned batteries aren’t eligible for the car-buyer subsidy, Ford executives have indicated they could scale back the investment; on Monday, the company paused construction of the new battery plant.
“This is not about GM vs. Ford,” a GM spokeswoman said. She said GM wants clarity and for the rules to follow the intent of the Inflation Reduction Act, which created the new tax-credit requirements.
Robbie Orvis, a senior director at Energy Innovation, a think tank on climate issues, said the tax credit—and the “foreign entity of concern” rule—will shape how many electric cars are sold in the U.S. in the next 10 years.
Ford hoped to get ahead by licensing technology from China’s Contemporary Amperex Technology Co. Ltd., known as CATL, to make lithium-iron-phosphate batteries at an industrial scale in the U.S. for the first time. They are much cheaper than other alternatives, reducing the production cost of the car.
Biden’s Self-Made Dilemma
Biden is guaranteed to upset someone. That’s what happens when you interfere in the free markets, taking sides.
Congressional members from Michigan have lined up behind GM. So did Senator Joe Manchin.
The infrastructure isn’t ready in either case, and inflation is sure to rise.
What About Materials?
Compounding the issue, “foreign entity of concern” also applies to the materials that go into the batteries.
Not only will Ford pay royalties to China for the battery technology, a strict definition of “foreign entity of concern” should apply to both GM and Ford over the minerals needed.
General Motors’ announcement on Tuesday that it plans to invest $650 million into Lithium Americas to secure access to lithium is the first of what surely will be more to come, according to Simon Moores, the CEO of Benchmark Mineral Intelligence.
“EV companies, especially the auto majors, have learnt the hard way over the last five years that scaling batteries — giga factories — is much easier and quicker than scaling mining,” Moores said.
It takes two years or more to build a giga factory and 10 years-plus to finance and build a lithium mine, Moores said.
Does the 10 years to build a mine factor in delays caused by clean energy NIMBY hypocrites who will fight new mines every step of the way?
Regardless, assume a giga factory is up and running in two years. Where precisely are the refined minerals for that giga factory coming from?
Once again, subsidies hinge on the definition of “foreign entity of concern”.
And where is the giga factory located. Will the giga factory use union labor driving up the cost?
What About Consumer Concerns?
Lost in the battle over “foreign entity of concern” ought to be the concern “how many people don’t want EVs crammed down their throats?”
No one is taking legitimate consumer concerns like price, insurance, number of reliable chargers, charging times, inflation, and even hurricane evacuations into proper consideration.
Are You Concerned?
You should be. Concern is the word of the day starting with government mandated EV solutions, regulations that will ban gas stoves, looting, and piss poor public education in big cities.
Oppenheimer initiated coverage on Fusion Pharmaceuticals IncFUSN, citing the company's pipeline as among the best in the space with alpha-emitter-based targeted radionuclide therapies (TRTs), with three currently in clinical development.
The analysts Jeff Jones and Kyle Yang have initiated with an Outperform rating and a price target of $13.
The company's candidates are making their mark in the well-established yet competitive field of metastatic castration-resistant prostate cancer (mCRPC) and are also exploring more innovative targets applicable to various solid tumors.
The opportunity for FPI-2265, as an alpha-emitter, to compete directly against beta-emitter treatments for patients could provide over 2x upside to Oppenheimer's current valuation.
The interim Phase 2 data from FPI-2265 in mCRPC patients, anticipated 1Q24, is expected to have a potential impact.
The analyst underscores that Novartis AG'sNVS recent supply challenges accentuate the crucial role of a well-managed supply chain in meeting the strong demand for Targeted Radiation Therapies (TRTs).
FUSN's management's expertise in isotope supply, coupled with the company's substantial investments in numerous suppliers, is viewed as a pivotal factor in cementing its robust standing in the market.
Professional societies agreed that U.S. centers performing pediatric and congenital heart surgery should be formally reorganized into two tiers with volume requirements designed to maintain surgical quality.
The first tier, the Comprehensive Care Centers, should house services to optimize comprehensive and high-complexity care, including neonatal open-heart surgery and pediatric heart transplant. Each center should perform at least 200 index pediatric heart surgeries per year and have at minimum three surgeons, among other requirements.
The second tier is the Essential Care Centers that can handle less complex cases and ventricular assist device placement in older children in emergent cases. A minimum 75 index cases per year is recommended at each center, where there should be at least two working surgeons.
In both center types, a congenital cardiac surgeon should be available 24 hours a day, 7 days a week, every day of the year, and have the ability to be in the hospital within 60 minutes of being called (ideally within 30 minutes in most geographic locations), according to a consensus statementopens in a new tab or window from a group led by Carl Backer, MD, a surgeon at Cincinnati Children's Hospital Medical Center, director of the American Board of Thoracic Surgery (ABTS), and past president of the Congenital Heart Surgeons' Society (CHSS).
The recommendations were published in the World Journal for Pediatric and Congenital Heart Surgery, Annals of Thoracic Surgery, and Journal of Thoracic and Cardiovascular Surgery.
Essential and Comprehensive Care Centers are urged to establish paired relationships for collaboration and patient transfer. It is recommended that both tiers participate in the Society of Thoracic Surgeons Congenital Heart Surgery Database, share outcomes transparently, and participate in quality and safety programs.
"In the last several years there have been multiple news stories regarding poor outcomes at different congenital heart centers. These reports have led to understandable concern and confusion on the part of patients and their families about whether their own institution is providing safe, quality care," said co-author David Overman, MD, of the Mayo Clinic-Children's Minnesota Cardiovascular Collaborative in Minneapolis and president of the CHSS, in a press release.
"[O]ur specialty, for the first time, has put forward recommendations for all congenital heart surgery centers," he said. "These guidelines will allow patients and families to better understand what they should expect at their institution and will drive improvement of outcomes across all centers."
The U.S. currently has over 150 congenital heart surgery centers, many low-volume and in close geographic proximity to each other. Approximately 35% of centers perform at least 250 index cases a year, while about 45% perform fewer than 150 annually, according to estimates from the Society of Thoracic Surgeons.
The new recommendations set standards that may make it hard for some existing congenital heart programs to keep running. The authors estimated that 14 out of the 95 currently reporting centers would not meet the 75-case yearly threshold for Essential Care Centers. However, volume exceptions may be made for centers in less-populated states that otherwise would not have a single Comprehensive Care Center.
The ABTS currently requires surgeons to log 50 congenital cardiac surgeries a year for maintenance of certification. Meanwhile, a recent Society of Thoracic Surgeons surveyopens in a new tab or window showed that of 201 practicing congenital heart surgeons who responded, a quarter reported performing fewer than 50 pediatric cases per year.
Until recently, 1-year fellowships have required candidates to perform a minimum of 75 major pediatric congenital cardiac surgeries as primary surgeons. Many graduated just barely exceeding that threshold -- raising concerns that trainees needed more cases and longer fellowships before entering the workforce.
On July 1, the ABTS started requiring candidates for congenital cardiac surgery fellowships to complete 2 consecutive years in a single accredited program and complete 150 major cases (with a minimum of 50 major cases in the first year of training).
The consensus statement was endorsed by the CHSS, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Academy of Pediatrics, American College of Cardiology, American Heart Association, American Society of Echocardiography, American Society of Extracorporeal Technology, Congenital Cardiac Anesthesia Society, Pediatric & Congenital Electrophysiology Society, Pediatric and Congenital Interventional Cardiovascular Society, Pediatric Cardiac Intensive Care Society, Pediatric Heart Transplant Society, Society of Pediatric Cardiovascular Nurses, and World Society for Pediatric and Congenital Heart Surgery.
Disclosures
Backer reported relationships with the Congenital Heart Surgeons' Society and the American Board of Thoracic Surgery.
Co-authors reported relationships with industry and various societies and councils.
Primary Source
Annals of Thoracic Surgery
Source Reference: opens in a new tab or windowBacker CL, et al "Recommendations for centers performing pediatric heart surgery in the United States" Ann Thorac Surg 2023; DOI: 10.1016/j.athoracsur.2023.08.016.
Socialist Rep. Jamaal Bowman (D-NY) pulled the fire alarm in a House office building Saturday as Democrats tried to delay a vote on aRepublican stopgap spending bill, according to the GOP-controlled Administration Committee.
The wild incident in the Cannon Building was caught on camera and confirmed by several witnesses, according to Politico.
Bowman “pulled a fire alarm in Cannon this morning,” a panel spokesperson told the outlet. “An investigation into why it was pulled is underway.”
Staten Island GOP Rep. Nicole Malliotakis’ office told The Post they would move to have Bowman expelled from the chamber.
“NY Democrat Jamaal Bowman literally pulled a fire alarm to stall and prevent our efforts to force a vote to keep the federal government open. Pathetic. Criminal investigation needs to happen,” said upstate GOP Congressman Nick Langworthy.
The wild incident in the Cannon Building was caught on camera.Rep. Nicole Malliotakis said they would move to have Bowman expelled from the chamber.EPA
Creating a false fire alarm is a misdemeanor in the District of Columbia and punishable by up to six months in jail.
“This is the United States Congress, not a New York City high school. To pull the fire alarm to disrupt proceedings when we are trying to draft legislation to AVERT A SHUTDOWN is pathetic…even for members of the socialist squad,” Malliotakis wrote on X, formerly Twitter.