Tax Day is an ideal moment to reflect on the growing cost of government. Government spending and the federal debt continue to rise, driven largely by federal health programs. Unfortunately, a substantial share of government health program spending is lost to waste, fraud, and abuse—as recent scandals in Minnesota, California, Indiana, New York, Florida, and Colorado demonstrate. Each year, more than $100 billion in federal Medicaid spending is likely improper, while improper and phantom enrollment continues to plague the Affordable Care Act (ACA) exchanges.
At the National Press Club on April 28, Paragon has invited Dr. Oz for an event focused on the Trump administration’s efforts to reduce improper payments, waste, and fraud in government health programs. The event will also feature a panel with Sen. Ron Johnson and Rep. John Joyce. Both chair key congressional oversight subcommittees dedicated to protecting federal programs for the most vulnerable. You can register for our in-person event here.
In today’s newsletter, I highlight the growing share of federal income tax revenue consumed by health programs, discuss evidence showing the persistence of improper enrollment in the Obamacare exchanges, preview Ryan Long’s testimony before the Senate HELP Committee on policies to reduce prescription drug costs through generic drug and biosimilar competition, and recap our virtual event on the evidence around banning smartphones in schools.
Federal Health Program Spending Consumes Nearly Two-Thirds of Relevant Federal Taxes
According to the Centers for Medicare and Medicaid Services, total national health expenditures reached $5.3 trillion in 2024, or 18 percent of GDP, with federal health care spending at $1.7 trillion. Federal policies influence much of this remaining spending. Last week, I joined Jeffrey Tucker to discuss employer-provided health insurance, the ACA, alternative coverage plans, and how government policies have driven up health care prices.
On Tax Day, Americans should consider not just how much they pay in federal income taxes, but where that money is going. As a new Paragon PIC shows, federal spending on health care programs consumed roughly 62 percent of all individual federal income taxes, corporate federal income taxes, and Medicare payroll tax revenue in 2025—up from 29 percent in 2000 and 17 percent in 1975. This high percentage shows how growth in federal health programs is crowding out other priorities while contributing to large annual deficits and a rapidly growing national debt.
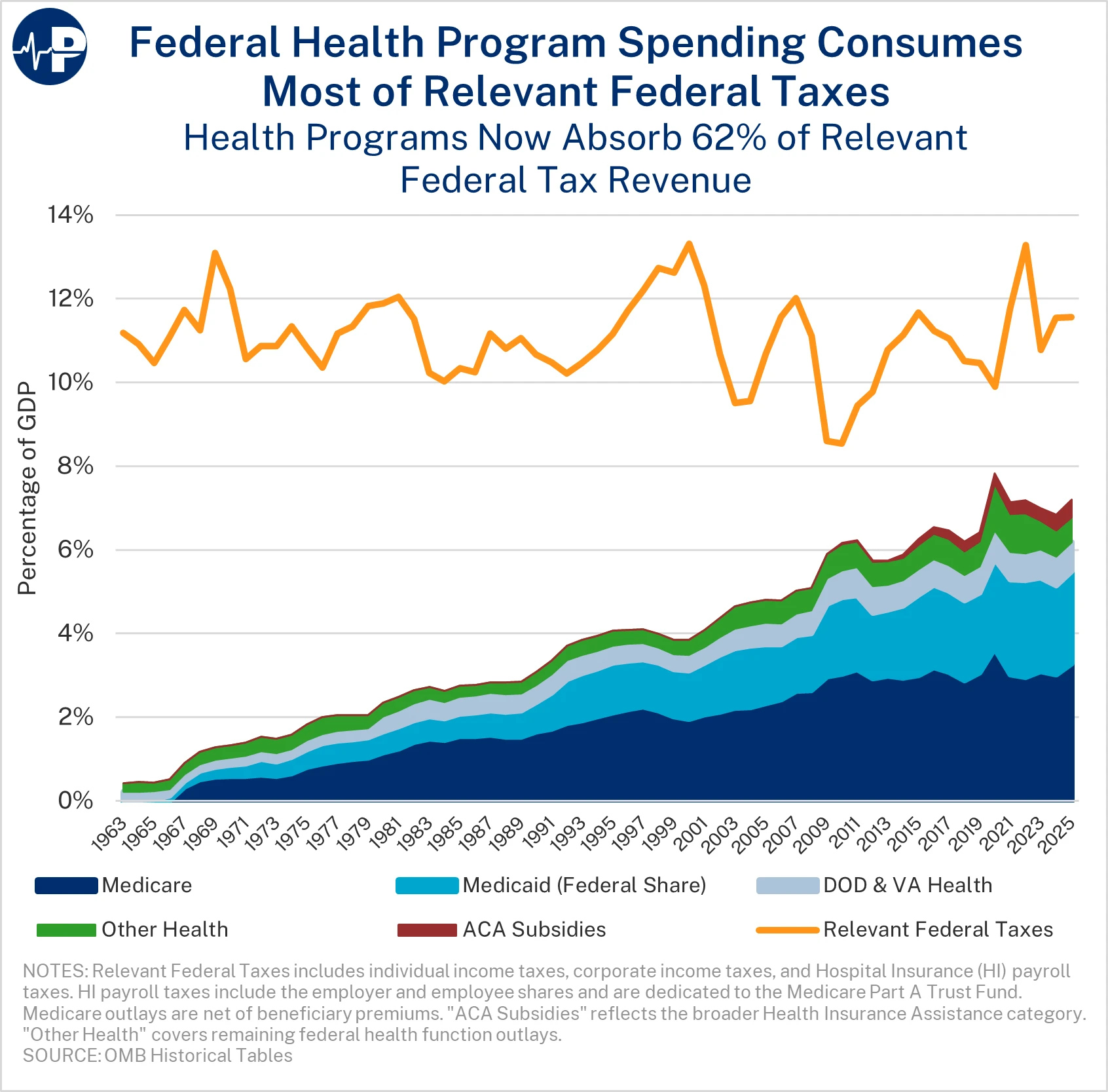
The PIC includes the Medicare Part A (hospital insurance) payroll tax revenue because it is dedicated to financing Part A. Part A payroll taxes cover only a fraction of total Medicare costs as Parts B (outpatient expenditures) and D (prescription drugs) are funded primarily through general revenue. Medicare costs continue to escalate, as do costs in other programs—particularly Medicaid and Affordable Care Act subsidies.
The Persistent Obamacare Enrollment Fraud
A new Paragon PIC demonstrates continued problems with the integrity of the Obamacare exchanges—namely an increase in the percentage of enrollees claiming income between 100 and 150 percent federal poverty level (FPL). In 2026, a staggering 56 percent of all sign-ups in states using the federal exchange—and 46 percent of all sign-ups nationally—claimed income in this narrow range. That is the highest national proportion ever recorded in the 100 to 150 percent FPL income range, up dramatically from 30 percent in 2020. Enrollees in the 100 to 150 percent FPL income range qualify for the largest subsidies, imposing substantial costs on taxpayers. (The data in the PIC is limited to federal exchange states because enrollment data by FPL category was not consistently available for state-based exchanges over the last decade.)
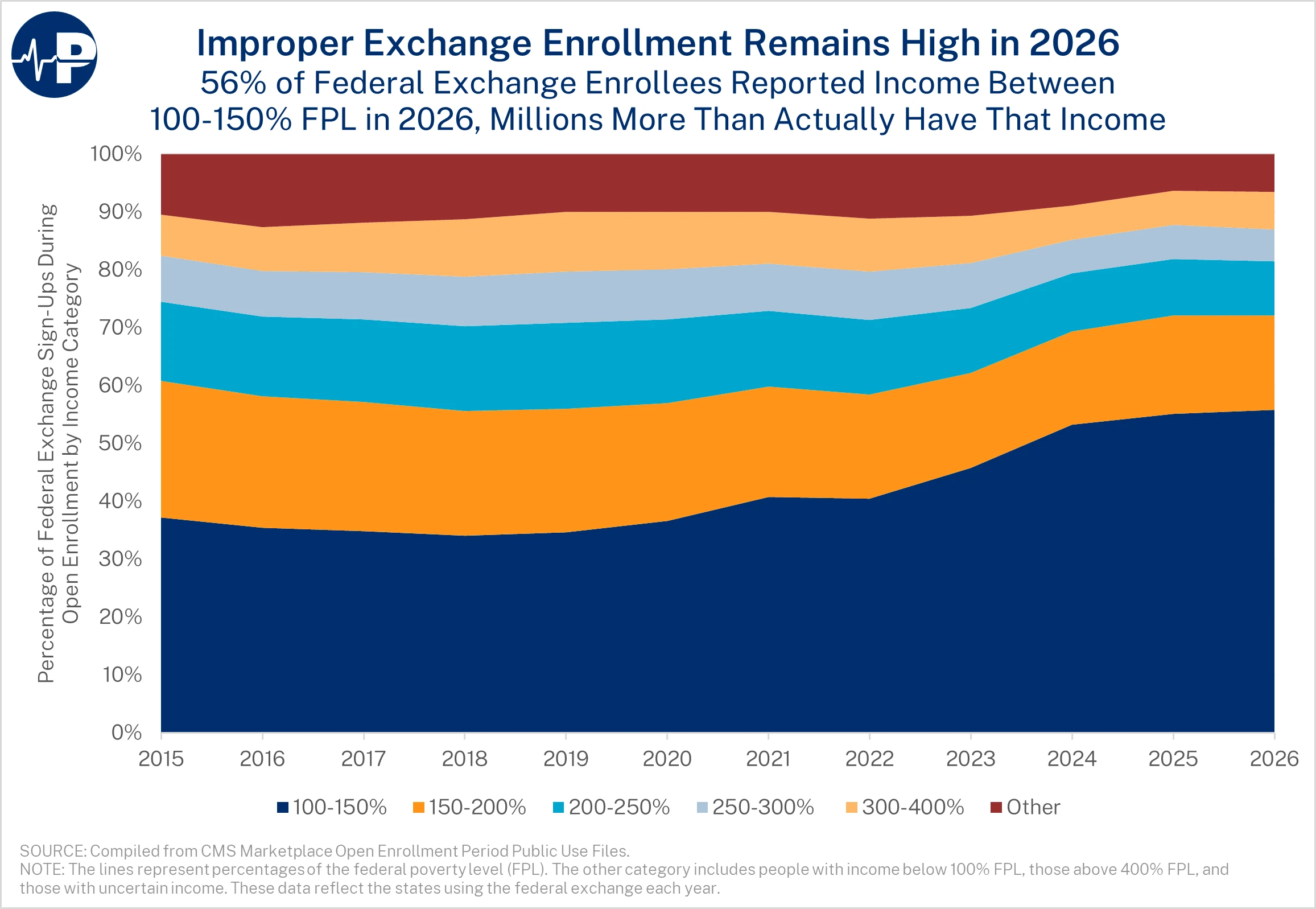
In 2025, we estimated that 6.4 million more enrollees claimed income in this range than had such income. Improper enrollment soared with COVID-era subsidy boosts that made 94 percent actuarial value plans fully subsidized for individuals claiming income in this category. Insurers received massive subsidy payments on behalf of people improperly enrolled, many of whom were phantom enrollees—individuals without knowledge of their enrollment or fictitious individuals created by unscrupulous brokers and enrollment intermediaries. Weak program integrity measures—as evidenced by the Government Accountability Office successfully enrolling 23 of 24 fictitious applicants into fully subsidized coverage—compounded the problem.
Extensive automatic re-enrollment and continued policies that permit widespread fully subsidized bronze and gold plans contribute to a climate where improper and phantom enrollment continues to flourish. I discussed the massive fraud, improper enrollment, and phantom enrollment in the Obamacare exchanges in a recent Washington Post podcast, along with the key 2027 Notice of Benefit and Payment Parameters (NBPP) reforms to expand consumer choice and curtail improper enrollment.
Improper enrollment existed before the COVID-era subsidy boosts due to incentives to misreport income, which benefited insurers, intermediaries, and enrollees aware of their enrollment. The misreporting of income to claim more subsidies grew substantially with the COVID-era subsidy boosts, as demonstrated by the increase in the percentage of federal exchange enrollees claiming income between 100 and 150 percent FPL during open enrollment.
Ryan Long Testifying before the Senate HELP Committee on Drug Costs
Tomorrow (Thursday, April 16) at 10 a.m., Paragon’s senior research fellow Ryan Long will testify before the Senate HELP Committee on generic drugs, biosimilars, and prescription drug costs.
In his testimony, Ryan highlights how generics and biosimilars have delivered substantial savings—more than $3 trillion in the past decade—while identifying policy barriers that continue to limit their full potential. He emphasizes that although biosimilar approvals have accelerated, with 90 products approved since 2016 and significant recent cost savings, adoption remains constrained by misaligned incentives in the pharmaceutical supply chain, particularly rebate structures that favor higher-cost branded drugs.
Ryan’s testimony underscores the success of the Hatch-Waxman framework and subsequent FDA reforms in improving generic drug approvals, noting that generics now account for 90 percent of prescriptions but only a small share of total drug spending. Ryan points to continued progress in reducing approval times and expanding access to complex generic drugs. At the same time, he identifies gaps in utilization, especially among Medicare Low-Income Subsidy beneficiaries, where current cost-sharing structures reduce incentives to choose lower-cost generics.
Ryan also focuses on structural issues that undermine competition, including the 340B program’s “buy low, sell high” incentives, which discourage the use of generics and biosimilars. He also highlights the importance of expanding over-the-counter access and modernizing regulatory pathways to improve access and reduce costs. His recommendations center on aligning incentives to support lower-cost alternatives, strengthening competition, and ensuring that savings from generics and biosimilars are more fully realized by patients and taxpayers.
Brian Blase, Ph.D., is the President of Paragon Health Institute. Brian was Special Assistant to the President for Economic Policy at the White House’s National Economic Council (NEC) from 2017-2019, where he coordinated the development and execution of numerous health policies and advised the President, NEC director, and senior officials. After leaving the White House, Brian founded Blase Policy Strategies and served as its CEO.
https://paragoninstitute.org/newsletter/taking-stock-of-government-health-program-costs-on-tax-day/
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.