The FDA designates Arena Pharmaceuticals’ (NASDAQ:ARNA) APD418 for Fast Track review for the treatment of decompensated heart failure (a sudden worsening of signs and symptoms, including difficulty breathing, fatigue and swelling in the legs and feet).
Fast Track status provides for more frequent interaction with the FDA review team and a rolling review of the marketing application.
The company says Phase 1-stage APD418 is a β3-adrenergic receptor (AdrR) antagonist and cardiac myotrope designed to improve cardiac contractility without the unwanted effects on heart rate, blood pressure and myocardial oxygen consumption associated with inotrope therapies.
The 2-year lull in the U.S. listing of Chinese biotechs is expected to end this week, with the upcoming IPO of I-Mab.
The IPO Terms
Shanghai-based I-Mab, a clinical-stage biopharma company, has filed to offer 7.41 million ADSs representing 17.04 million ordinary shares in an IPO, according to an amended filing with SEC.
The company expects to price the offering between $12 and $15 per ADS. It has applied for listing its ADSs on the Nasdaq under the ticker symbol IMAB.
At the midpoint of the price range, the offering is expected to raise gross proceeds of $100 million.
Jefferies and CICC are the lead underwriters for the IPO, with China Renaissance and Huatai Securities serving as co-managers.
The Company
I-Mab is focused on the development of biologics, primarily for cancers and autoimmune disorders. The company has a rich pipeline, with five licensed assets, which are in varying stages of clinical trials.
These apart, the company also has a few proprietary compounds in development either in pre-clinical or early-stage clinical trials.
The most-advanced compound in its pipeline is TJ202, a differentiated CD38 antibody it has licensed from Morphosys Ag MOR 2.91%. TJ202 is being evaluated for multiple myeloma or autoimmune disorders.
Source: F1/A filing
The Finances
I-Mab generates revenues from licensing and collaboration and is yet to turn in a profit.
For the 9-month period ended Sept. 2019, the company reported revenues of $4.197 million, down about 31% year-over-year. The net loss for the period widened from $6.11 per share to $21.49 per share.
The Culinary Health Center is a beige, two-story office building on Las Vegas’ east side, miles from the casino glitz of the Strip and not much to look at by Sin City standards. The surprise is what happens inside, and how it gets paid for, which would probably make most American workers’ jaws drop.
On a recent Friday, the parking lot was full as union members and their families visited the facility for primary and pediatric checkups, dental procedures and eye tests and eyeglasses, almost all of which are offered at no cost. There’s no emergency room, but X-ray, ultrasound and CT scan equipment awaited use in the building’s 24-hour urgent-care wing, free of cost to union members, along with a pharmacy that offers free generic medications.
In the hallways, there are few markings indicating the facility is operated on behalf of the Culinary Workers Union Local 226, which represents 60,000 hotel and casino workers in the early-caucusing and general election swing state of Nevada. But there’s a phrase printed on the front door symbolizing the powerful union’s pride in its unique healthcare setup: “Exclusively ours.”
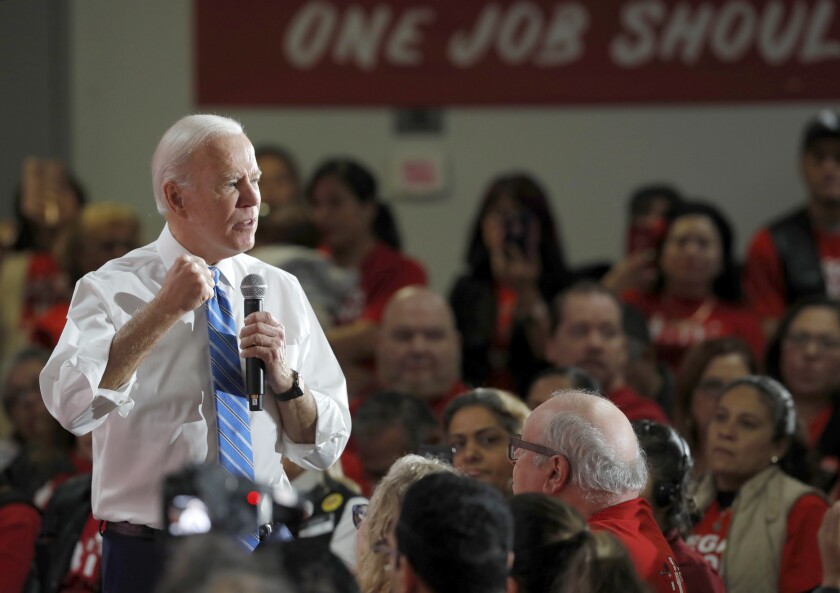
Joe Biden addresses a town hall meeting at the Culinary Workers Union Local 226 in Las Vegas.
(Steve Marcus / Las Vegas Sun)
“I love it. I love it. Everything, one-stop shop. Great doctors,” Kimberly Williams, 45, a guest room attendant at the Bellagio for 15 years and a volunteer organizer for the union, said of the center. “I have had other insurance before, but I believe my Culinary insurance is the best, and I want to keep that.”
The labor movement has long pushed for more comprehensive government healthcare in the U.S. But to see why some unions are nervous about talk of “Medicare for all” in the 2020 Democratic presidential primary, there’s no better place to start than the Culinary Union, whose parent union, Unite Here, has waged aggressive strikes and contract campaigns with employers to secure a level of affordability, accessibility and autonomy over healthcare coverage that would be unrecognizable to most Americans.
Instead of receiving health insurance directly through their employers, Culinary Union workers and many Unite Here members across the country receive health insurance through Unite Here Health. It’s a multi-employer nonprofit trust jointly run by Unite Here and by unionized companies that have agreed, however grudgingly, to sign on to the fund and its union-negotiated plans — which put the overwhelming burden of paying for healthcare onto companies, not workers.
American workers, on average, pay for 18% of the cost of a single-coverage plan and 29% for a family-coverage plan, with employers picking up the rest, according to a recent survey by the Kaiser Family Foundation. Unite Here Health, by comparison, gets just 3% of its funding from union workers, according to the union’s financial statements. (Some other unions have similarly structured multi-employer plans.) Unite Here Health also operates the Culinary Health Center and other facilities in Chicago and Atlantic City.
So as Democratic presidential candidates court the support of the Culinary Union, which is famed for the effectiveness of its election turnout operations in Nevada, the union has not been subtle in sharing its skepticism about the type of Medicare-for-all platforms advanced by Sen. Bernie Sanders of Vermont and Sen. Elizabeth Warren of Massachusetts. Those proposals, which aim to replace private employment-linked insurance plans with universal government insurance, would almost certainly reduce the amount of control some unions have over their health insurance.
Sen. Elizabeth Warren with Carmen Ramos, who became emotional during a town hall meeting at the Culinary Workers Union Local 226 headquarters in Las Vegas.
(Yasmina Chavez / Las Vegas Sun)
“If you’re telling anybody that they have to give up something they like for something they don’t know, that’s a pretty hard sell,” D. Taylor, the president of Unite Here, said in an interview.
The healthcare question has been posed at every town hall that Democratic candidates have held at the Culinary Union’s headquarters in Las Vegas.
“My brothers and sisters of the Culinary have been fighting for this health insurance for 84 years, fighting hard, and we’re still doing it,” Cristhian Barneond, a cook and a shop steward at the Cosmopolitan hotel, told Warren during her appearance on Dec. 9. “My question for you is, what is your plan to make sure we keep our Culinary health [insurance] intact?”
Warren said she had toured the Culinary Health Center and was “knocked out” by the arrangement. “What you’ve got is something I want to see replicated all around America,” Warren said of the union’s clinic. “The part that changes is the money and where the money comes from.”
Sanders, who has an even more aggressive Medicare-for-all plan, got a skeptical reception from some Culinary workers in Las Vegas on Dec. 11.
“We love our Culinary healthcare,” Elodia Muñoz, who went on strike for more than six years at the Frontier Hotel and Casino in the 1990s, told Sanders. “We want to keep it. I don’t want to change it. Why should I change it?”
“We have in this country a dysfunctional, broken and cruel healthcare system,” Sanders replied. But as he elaborated on his plan, chants from the audience interrupted, “Union healthcare! Union healthcare!” multiple times, drawing a rebuke from the union’s president. (“If you want to heckle, go outside to heckle,” Taylor told the chanters afterward.)
Sanders powered through and said his plan would result in higher wages for union workers, with employers no longer diverting dollars toward private health insurance programs with large or inefficient overheads.
Former Vice President Joe Biden had a much easier time in his Dec. 11 appearance: He, like Mayor Pete Buttigieg of South Bend, Ind., favors a more moderate plan to create a public option that would not replace the Culinary Union’s insurance plan.
“You’re gonna get to keep it with me,” Biden interrupted a cook from Margaritaville, who was winding up to ask Biden the same question every other candidate has gotten.
“Where I come from, I don’t like people telling me what I have to choose,” Biden said. Union members “who have busted their neck, walked on picket lines, gave up pay, took hits in order to get significant healthcare available, you get to keep it under my plan. You don’t have to give it up.”
Nia Winston, president of Unite Here Local 24 of Detroit, reacts during a town hall meeting with Sen. Bernie Sanders at the Culinary Workers Union Local 226 in Las Vegas.
(Krystal Ramirez / Las Vegas Sun)
Universal health insurance systems spread around the world after World War II, but not in the U.S., where private, employer-provided insurance flourished instead. This system has come under political strain in recent years as insurance costs have risen faster than wages, which has also forced many unions to fight losing battles against contracts that would increase healthcare costs for their members.
The Culinary Union has won and maintained its provisions through decades of strikes and bargaining. In 1984, 17,000 Culinary members from 32 Las Vegas Strip resorts went on strike for almost a year, a period during which 900 strikers were arrested. Another strike, at the Frontier Hotel and Casino, began in 1991 and lasted for more than six years.
Last year, employers under contract with Unite Here unions paid more than $1 billion in contributions into the union’s healthcare trust, compared with just $28.8 million from union members. Culinary Union workers don’t have premiums or deductibles, but they have certain copays and pharmaceutical costs, according to Culinary Union spokesperson Bethany Khan, who said the Culinary Health Center’s pharmacy fills about 20,000 prescriptions monthly.
In other words, the union in effect has its own private version of the single-payer system, with hotels and casinos, rather than the government, functioning as the single payer.
Although the Culinary Union is respected for its gains, labor activists who support Medicare for all still think universal governmental coverage would be more efficient, comprehensive and stable than such multi-employer plans, which are also offered by some other unions, including SAG-AFTRA and the Writers Guild of America.
“A lot of these funds, they cover precarious workers, construction workers, actors, people in film production, and they provide good benefits, but large numbers and large percentages of their members don’t qualify for their benefits because they don’t work enough hours,” said Mark Dudzic, coordinator of the Labor Campaign for Single Payer, a union coalition pushing for a Sanders-like Medicare-for-all plan.
Unions would also no longer have to bargain over whether employers’ dollars should go toward healthcare instead of wages or other benefits. “I think you could really construct much better advantages if you didn’t have to put all this money into basic healthcare,” Dudzic said.
In an interview Saturday, Sanders acknowledged that “there were a few people who objected” at his Culinary Union town hall but noted that he got a standing ovation at the end of the event.
“We have many unions who support Medicare for all, some who are reluctant,” Sanders said. But he thinks he can still make his case to union members by persuading them that under Medicare for all, “they’re not going to have to spend half of their negotiating sessions protecting the healthcare that they have, and they’re not going to have to give up wage increases in order to maintain or improve their healthcare benefits.”
Despite the Culinary Union’s reluctance on Medicare for all, Taylor, the Unite Here president, praised each of the Democrats who have passed through, and he made clear that he didn’t want it perceived that his union was fighting progressive changes on healthcare that would benefit less-fortunate workers.
“Just so we’re clear for all media, the healthcare system in this country has to change,” Taylor said during Warren’s event. “Healthcare should be a right and not a privilege, and no one should go without it.”
Schrödinger, which provides a software platform for life sciences and materials research, filed on Friday with the SEC to raise up to $100 million in an initial public offering.
The New York, NY-based company was founded in 1990 and booked $77 million in revenue for the 12 months ended September 30, 2019. It plans to list on the Nasdaq under the symbol SDGR. Morgan Stanley, BofA Securities, Jefferies, and BMO Capital Markets are the joint bookrunners on the deal. No pricing terms were disclosed.
Early morning blue light exposure therapy can aid the healing process of people impact by mild traumatic brain injury, according to new research from the University of Arizona.
“Daily exposure to blue wavelength light each morning helps to re-entrain the circadian rhythm so that people get better, more regular sleep. This is likely true for everybody, but we recently demonstrated it in people recovering from mild traumatic brain injury, or mTBI. That improvement in sleep was translated into improvements in cognitive function, reduced daytime sleepiness and actual brain repair,” said William D. “Scott” Killgore, psychiatry professor in the College of Medicine – Tucson and lead author on a new study published in the journal Neurobiology of Disease.
Mild traumatic brain injuries, or concussions, are often the result of falls, fights, car accidents and sports participation. Among other threats, military personnel can also experience mTBI from exposure to explosive blasts: Shockwaves strike the soft tissue of the gut and push a burst of pressure into the brain, causing microscopic damage to blood vessels and brain tissue, Killgore said.
“Your brain is about the consistency of thick Jell-O,” he said. “Imagine a bowl of Jell-O getting hit from a punch or slamming against the steering wheel in a car accident. What’s it doing? It’s absorbing that shock and bouncing around. During that impact, microscopic brain cells thinner than a strand of hair can easily stretch and tear and rip from the force.”
Those with a concussion or mTBI might can momentarily seen stars, become disoriented, or even briefly lost consciousness following the injury; however, loss of consciousness doesn’t always happen and many people who sustain a concussion are able to walk it off without realizing they have a mild brain injury, according to Killgore. Headaches, attention problems and mental fogginess are commonly reported after head injuries and can persist for weeks or months for some people.
Few, if any, effective treatments for mTBI exist. The U.S. Army Medical Research and Development Command funded the research to find alternatives to medicinal methods of mTBI recovery.
“About 50% of people with mTBI also complain that they have sleep problems after an injury,” Killgore said.
Recent research has shown that the brain repairs itself during sleep, so Killgore and his co-authors – John Vanuk, Bradley Shane, Mareen Weber and Sahil Bajaj, all from the Department of Psychiatry – sought to determine if improved sleep led to a faster recovery.
In a randomized clinical trial, adults with mTBI used a cube-like device that shines bright blue light (with a peak wavelength of 469 nm) at participants from their desk or tables for 30 minutes early each morning for six weeks. Control groups were exposed to bright amber light.
“Blue light suppresses brain production of a chemical called melatonin,” Killgore said. “You don’t want melatonin in the morning because it makes you drowsy and prepares the brain to sleep. When you are exposed to blue light in the morning, it shifts your brain’s biological clock so that in the evening, your melatonin will kick in earlier and help you to fall asleep and stay asleep.”
People get the most restorative sleep when it aligns with their natural circadian rhythm of melatonin – the body’s sleep-wake cycle associated with night and day.
“The circadian rhythm is one of the most powerful influences on human behavior,” Killgore said. “Humans evolved on a planet for millions of years with a 24-hour light/dark cycle, and that’s deeply engrained in all our cells. If we can get you sleeping regularly, at the same time each day, that’s much better because the body and the brain can more effectively coordinate all these repair processes.”
As a result of the blue light treatment, participants fell asleep and woke an average of one hour earlier than before the trial and were less sleepy during the daytime. Participants improved their speed and efficiency in brain processing and showed an increase in volume in the pulvinar nucleus, an area of the brain responsible for visual attention. Neural connections and communication flow between the pulvinar nucleus and other parts of the brain that drive alertness and cognition were also strengthened.
“We think we’re facilitating brain healing by promoting better sleep and circadian alignment, and as these systems heal, these brain areas are communicating with each other more effectively. That could be what’s translating into improvements in cognition and less daytime sleepiness,” Killgore said.
Blue light from computers, smartphones and TV screens often gives blue light a bad rap. But according to Killgore, “when it comes to light, timing is critical. Light is not necessarily good or bad in-and-of-itself. Like caffeine, it all comes down to when you use it. It can be terrible for your sleep if you’re consuming coffee at 10 o’clock at night, but it may be great for your alertness if you have it in the morning.”
He and his team plan to continue their research to see if blue light improves sleep quality and how light therapy might affect emotional and psychiatric disorders. Killgore believes that most people, whether injured or healthy, could benefit from correctly timed morning blue light exposure, a theory he hopes to prove for certain in future studies.
The vast majority of patients with knee osteoarthritis in the United States who are considered appropriate for total knee replacement do not receive the surgery in a timely manner, whereas many who are not appropriate candidates have the knee replacement anyhow — prematurely, with both scenarios carrying important risks, new research shows.
“Our study suggests that there is a potentially large number of patients with knee osteoarthritis in the US who could benefit from total knee replacement but do not undergo the procedure,” the authors report.
The study, published this week in the Journal of Bone and Joint Surgery, is believed to be the first of its kind to prospectively assess the timeliness of knee replacement among a large number of patients with knee osteoarthritis.
“With nearly 1,000,000 total knee replacements being performed in the US each year, the present study provides important impetus for future efforts directed at measuring and improving timely utilization of total knee replacement,” the authors say.
The research included patients who had knee osteoarthritis or were at risk of the condition from two large prospective cohort studies — the Osteoarthritis Initiative (OAI), conducted from February 2004 to May 2006 at four clinical sites, and the Multicenter Osteoarthritis (MOST) study, evaluating patients from April 2003 to April 2005 at two sites.
Of a total of 8002 knee osteoarthritis cases identified in the two studies, 3417 knees met inclusion criteria for the analysis.
After a follow-up of up to 8 years, only 9% of those considered to be potentially appropriate for total knee replacement received total knee replacement surgery within a “timely” manner, defined as within 2 years of becoming potentially appropriate for the surgery.
Meanwhile, 90.7% of those considered “potentially appropriate” for the surgery did not have the replacement in a “timely” manner.
In addition, among the 1114 total knee replacements that were performed, 26.4% were considered to be “likely inappropriate” and therefore premature.
The criteria for the appropriate timing of knee replacement surgery was based on evidence-based recommendations that consider factors including age, symptomatology, radiographic knee osteoarthritis severity, number of knee compartments involved, and knee stability.
Key factors associated with an increased risk of not having a knee replacement when appropriate included being African American (odds ratio [OR], 2.81), and the likelihood of having premature total knee replacement surgery was lower among participants with a body mass index above 25 kg/m2 (OR, 0.33) and those with depression (OR, 0.37).
Among the knees considered potentially appropriate but not replaced, nearly half (42.5%) of patients had severe symptoms, defined as combined Western Ontario and McMaster Universities [WOMAC] Pain and Physical Function scores of 34 or above.
In addition to the sustained pain, the delay in knee replacement when the surgery is considered appropriate can lead to a cascade of undesired events, lead investigator Hassan Ghomrawi, PhD, MPH, said in a news release.
“When people wait too long, two things happen,” said Ghomrawi, who is an associate professor of surgery at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“The osteoarthritis causes deterioration of their function. Some of them wouldn’t be able to straighten out their legs, affecting their walking and mobility,” he said. “When you can’t get exercise, you can start to develop other health problems such as cardiovascular problems. You may also become depressed. The overall impact can be huge.”
Secondly, the surgery itself may provide less benefit if delayed.
“You don’t get as much function back when you wait too long; your mobility is still reduced vs somebody who had it in a timely fashion,” Ghomrawi said.
Undergoing total knee replacement too early, in addition to likely providing little to no benefit, can mean exposing patients to the numerous risks that are associated with a major surgery.
Since total knee replacement is elective, a host of demographic, socioeconomic, and sociocultural factors can all come into play in determining whether, and when, a patient has the surgery, even in the context of pain, the authors write.
“While it is reasonable to assume that a subset of such patients have sensible reasons for not undergoing total knee replacement (for example, medical contraindications or the need to delay surgery because of the responsibility of caring for others, eg, a spouse or parent), the rest actually may benefit from surgery.”
Evidence points to several specific reasons for the higher rates of delays among African Americans, including research that indicates a greater likelihood of having lower expectations of surgery, the authors add.
“In addition, physician networks in communities with higher proportions of black residents are more likely to be smaller and more insular, which may result in lower utilization of and poorer access to total knee replacement,” they say.
“Understanding the reasons and barriers resulting in delay in those subpopulations is important, as the superiority of total knee replacement over nonoperative management has been demonstrated.”
The study was funded by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health. The authors have disclosed no relevant financial relationships.
Journal of Bone and Joint Surgery. Published January 13, 2020.Abstract
Goop, Gwyneth Paltrow’s lifestyle brand, is coming to your living room via Netflix with “The Goop Lab,” where Gwyneth and her crackerjack team look at various wellness topics.
Now, I want to make it clear that I like Gwyneth Paltrow. If Gwyneth wants to invite me to the Oscars, I’m in. Party at her Brentwood estate? Sign me up.
But Goop… See, Goop bothers me a bit. Here’s why.
Goop is not your typical lifestyle brand hawking makeup and 10 tips to make sex outstanding. I mean, it is. But a huge part of its business model relies on selling products based on dubious health claims. You may remember the kerfuffle that resulted from Goop’s “jade vaginal eggs” marketed to improve sexual functioning.
Image source: Goop
Currently, the site sells a variety of herbal remedies in very classy, medical-appearing packaging. Here is Goop’s “Perfect Attendance” supplement, which purports to offer “immune support.” Note the careful avoidance of terms that would imply that it is intended to treat, cure, or prevent any disease, which would subject the substance to FDA scrutiny.
And, honestly, the size of that market is an indictment against the conventional medical industry. For many conditions—I’m looking at you, low back pain—conventional therapy is limited, costly, or has significant side effects. Doctors don’t have enough time to really get to know their patients, to understand what’s going on beneath the surface level. CAM providers offer more than weird lotions and energy manipulation; they offer a sympathetic ear, hope, and understanding.
And yes, some patients heed that siren song of CAM—side effect–free curative treatments—and forgo conventional therapy. This is a problem.
A study published in JAMA Oncologymatched 258 cancer patients who used CAM to 1032 who did not. Seven percent of the CAM group refused surgery, 34% refused chemotherapy, and 53% refused radiotherapy. Perhaps not surprising, 5-year survival was significantly lower in the CAM group.
So, yes, there are some people who avoid necessary care because they pursue a care modality that appears safer to them—and they pay the price for it.
There are other adverse effects of CAM therapies.
A study in the New England Journal of Medicineexamined emergency department (ED) records and determined that about 23,000 ED visits per year are due to adverse effects of supplements, often because of the cardiovascular effects of weight-loss or energy products.
But people end up in the ED all the time for problems with conventional medications, too. In reality, most people integrate herbs and supplements into the rest of their medical routine without adverse effects.
Better regulation and oversight would go a long way to make supplements safer. But honestly, this is still not what really bothers me about companies that sell CAM, companies like Goop. It’s something a bit deeper. It’s that their business model depends on sowing doubt about the very scientific method upon which we’ve built modern medicine. They substitute anecdote for analysis. They appeal to the use of a product throughout history as adequate evidence of its safety and efficacy.
I am thankful that we’ve moved away from this approach, lest the lead tableware the Romans preferred still be found at our dinner tables.
We are in part to blame for the rise of companies like Goop. We’ve dropped the ball and left the emotional and psychological needs of our patients at the door in service of our need to see 50 patients a day to make ends meet. In the vacuum we’ve created, all sorts of people—from the true believers to cynical hucksters—will step in.
But even in the best light, the CAM-selling companies need to bear some blame. They do better when patients trust their doctors less. They embrace the anti-expertise, anti-intellectual milieu we’ve found ourselves in and paint conventional docs like me as pharmaceutical company shills at best, sociopathic mass murderers at worst.
Still, it remains my firm belief that if we can recapture the spirit of community with our patients, if we can spend more time looking at them and less at a computer screen, more time listening and less time billing, they will come back to us—if for no other reason than that our medicines work.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Program of Applied Translational Research. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @methodsmanmd and hosts a repository of his communication work at www.methodsman.com.