The sudden outbreak of the Wuhan Novel Coronavirus (2019-nCoV) has resulted in all of China’s
Hubei Province and three major cities in Zhejiang Province being
subjected to quarantine. Other nations are anxiously trying to get their
people out of China, and restrictions are being placed on flights to
China. Because this novel virus has an extremely high transmission speed
(high R0) and a high fatality rate, it is posing a significant
challenge to public health, not only in China, but around the world.
There are major gaps in our knowledge of the virus’s origin, duration
of human-to-human transmission, and clinical management of those
infected based on the current limited information coming from China.
Nevertheless, the findings of those scientists who have recently
published research papers about this virus are summarized below.
Lancet Article Reports Wuhan Virus Not Likely Caused by Natural Recombination
Most papers reported that the 2019-nCoV is only 88 percent related to the closest bat coronavirus,
only 79 percent to SARS, and just 50 percent to MERS. Professor Roujian
Lu from the China Key Laboratory of Biosafety, National Institute for
Viral Disease Control and Prevention, Chinese Center for Disease Control
and Prevention, and his co-authors commented in a Jan. 30 paper in Lancet that “recombination is probably not the reason for emergence of this virus.”
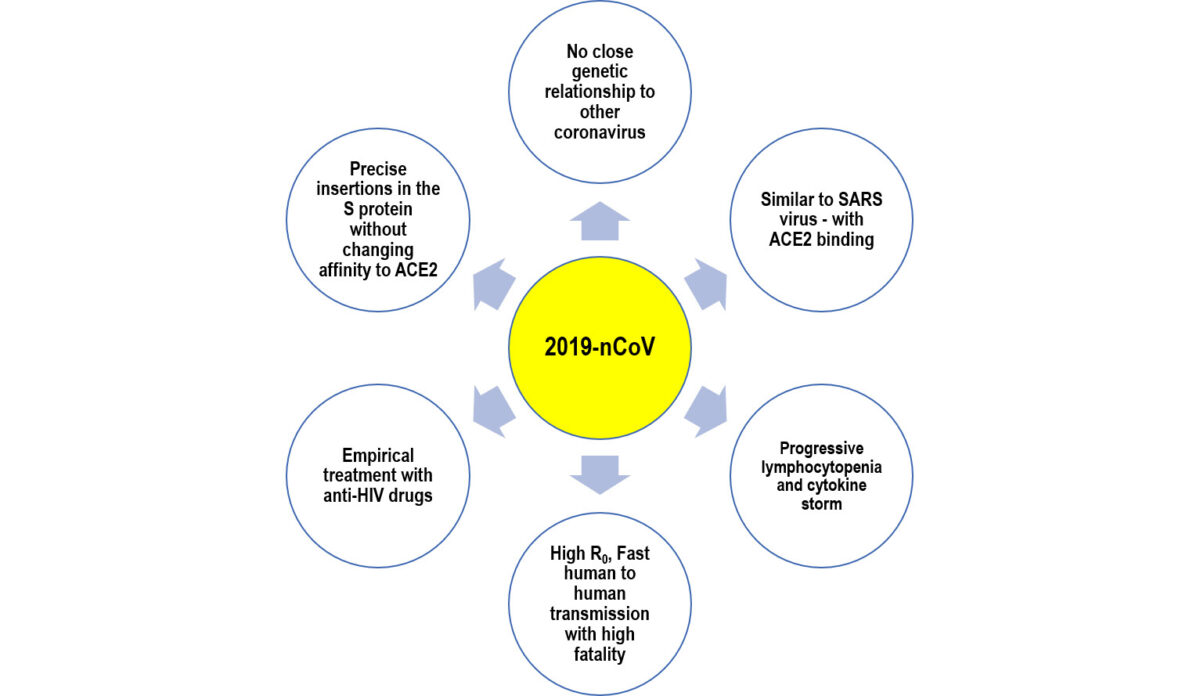
A Jan. 27 2020, study
by 5 Greek scientists analyzed the genetic relationships of 2019-nCoV
and found that “the new coronavirus provides a new lineage for almost
half of its genome, with no close genetic relationships to other viruses
within the subgenus of sarbecovirus,” and has an unusual middle segment
never seen before in any coronavirus. All this indicates that 2019-nCoV
is a brand new type of coronavirus. The study’s authors rejected the
original hypothesis that 2019-nCoV originated from random natural
mutations between different coronaviruses. (Paraskevis et al 2020
BioRxiv) The article is a preprint made available through bioRxiv and
has not been peer-reviewed. Puzzles of the Wuhan Novel Coronavirus (Yuhong Dong)
Very High Genetic Identity in Patients Indicates a Recent Transmission to Humans
2019-nCoV is an RNA virus. RNA viruses have high natural mutation
rates. The Lancet study by Lu et al. states: “As a typical RNA virus,
the average evolutionary rate for coronaviruses is roughly 10-4
nucleotide substitutions per site per year, with mutations arising
during every replication cycle. It is, therefore, striking that the
sequences of 2019-nCoV from different patients described here were
almost identical, with greater than 99.9% sequence identity. This
finding suggests that 2019-nCoV originated from one source within a very
short period and detected relatively rapidly.”
A Jan. 31 article
by Jon Cohen in Science said: “The longer a virus circulates in a human
population, the more time it has to develop mutations that
differentiate strains in infected people, and given that the 2019-nCoV
sequences analyzed to date differ from each other by seven nucleotides
at most, this suggests it jumped into humans very recently. But it
remains a mystery which animal spread the virus to humans.”
Bat or Huanan Market Source Is Not the Whole Story
Prof. Lu et. al. also discussed the natural host of the virus. An
early hypothesis had been the virus had passed to humans from bats sold
at Wuhan’s Huanan Seafood Market.
Lu et. al write: “First, the outbreak was first reported in late
December 2019, when most bat species in Wuhan are hibernating. Second,
no bats were sold or found at the Huanan seafood market, whereas various
non-aquatic animals (including mammals) were available for purchase.
Third, the sequence identity between 2019-nCoV and its close relatives
bat-SL-CoVZC45 and bat-SL-CoVZXC21 was less than 90%. Hence,
bat-SL-CoVZC45 and bat-SL-CoVZXC21 are not direct ancestors of
2019-nCoV.”
The authors point out that while the 2019-nCoV causing the Wuhan
outbreak might have initially been hosted by bats, it may have been
transmitted to humans via other as yet unknown mechanisms.
The Science article said: “Huanan marketplace played an early role in
spreading 2019-nCoV, but whether it was the origin of the outbreak
remains uncertain. Many of the initially confirmed 2019-nCoV cases—27 of
the first 41 in one report, 26 of 47 in another—were connected to the
Wuhan market, but up to 45%, including the earliest handful, were not.
This raises the possibility that the initial jump into people happened
elsewhere.”
Spike Protein Has 4 Precise Mutations Without Impacting Its Affinity for Human Receptor
Every virus must have a receptor to bind to human cells, can only
live inside human cells, and must rely on human cells to replicate.
Without these capabilities, viruses found circulating in blood or tissue
fluids are easily cleared by the human immune system.
Viruses enter human cells via specific surface protein channels. The
interaction of viral surface proteins binding to human cells is similar
with how keys are used to open locks.
Previous studies have shown there are several receptors that
different coronaviruses bind to, such as angiotensin-converting enzyme 2
(ACE2) for SARS-CoV. ACE2 receptors are abundantly present in human
tissue, especially along the epithelial linings of lung and small
intestines, provide routes of entry into cells for SARS-CoV.
According to Lu et al.’s Lancet paper, there is a structural
similarity between the receptor-binding domains of SARS-CoV and
2019-nCoV. 2019-nCoV spike protein (S-protein) is responsible for
binding to cell receptors and is crucial for viral targeting of host
tissue. The molecular modelling data by Lu et. al. suggests that,
despite the presence of amino acid mutations in the 2019-nCoV
receptor-binding domain, 2019-nCoV might use the ACE2 receptor to gain
entry into host cells.
On Jan. 21, 2020, Xintian Xu et al. from Key Laboratory of Molecular
Virology and Immunology, Institute Pasteur of Shanghai, Center for
Biosafety Mega-Science, Chinese Academy of Sciences, Shanghai, China,
published a paper entitled “Evolution of the novel coronavirus from the
ongoing Wuhan outbreak and modeling of its spike protein for risk of
human transmission” in SCIENCE CHINA Life Sciences. This paper provided a more precise analysis of the S-protein of Wuhan 2019-nCoV.
The S-protein was known to usually have the most variable amino acid
sequences compared to other gene domains from coronavirus. However,
despite considerable genetics distance between the Wuhan CoV and the
human-infecting SARS-CoV, and the overall low homology of the Wuhan CoV
S-protein to that of SARS-CoV, the Wuhan CoV S-protein had several
patches of sequences in the receptor binding (RBD) domain with a high
homology to that of SARS-CoV. The residues at positions 442,
472, 479, 487, and 491 in SARS-CoV S-protein were reported to be at
receptor complex interface and considered critical for cross species and
human-to-human transmission of SARS-CoV. So to our surprise, despite
replacing four out of five important interface amino acid residues, the
Wuhan CoV S-protein was found to have a significant binding affinity to
human ACE2. The replacing residues at positions 442, 472, 479,
and 487 in the Wuhan CoV S-protein did not alter the structural
conformation. The Wuhan CoV S-protein and SARS-CoV S-protein
shared an almost identical 3-D structure in the RBD domain, thus
maintaining similar van der Waals and electrostatic properties in the
interaction interface. Thus the Wuhan CoV is still able to pose
a significant public health risk for human transmission via the S
protein–ACE2 binding pathway.” (emphasis added)
We know already that the novel 2019-nCoV is a different virus than
SARS. It is understood that S-protein is highly variable. It would be no
surprise if the genetic sequence, protein structure, and even the
function of 2019-nCoV’s S-protein is different than that of the SARS
virus. But, how could this novel virus be so intelligent as to mutate
precisely at selected sites while preserving its binding affinity to the
human ACE2 receptor? How did the virus change just four amino acids of
the S-protein? Did the virus know how to use Clustered Regularly
Interspaced Short Palindromic Repeats (CRISPR) to make sure this would
happen?
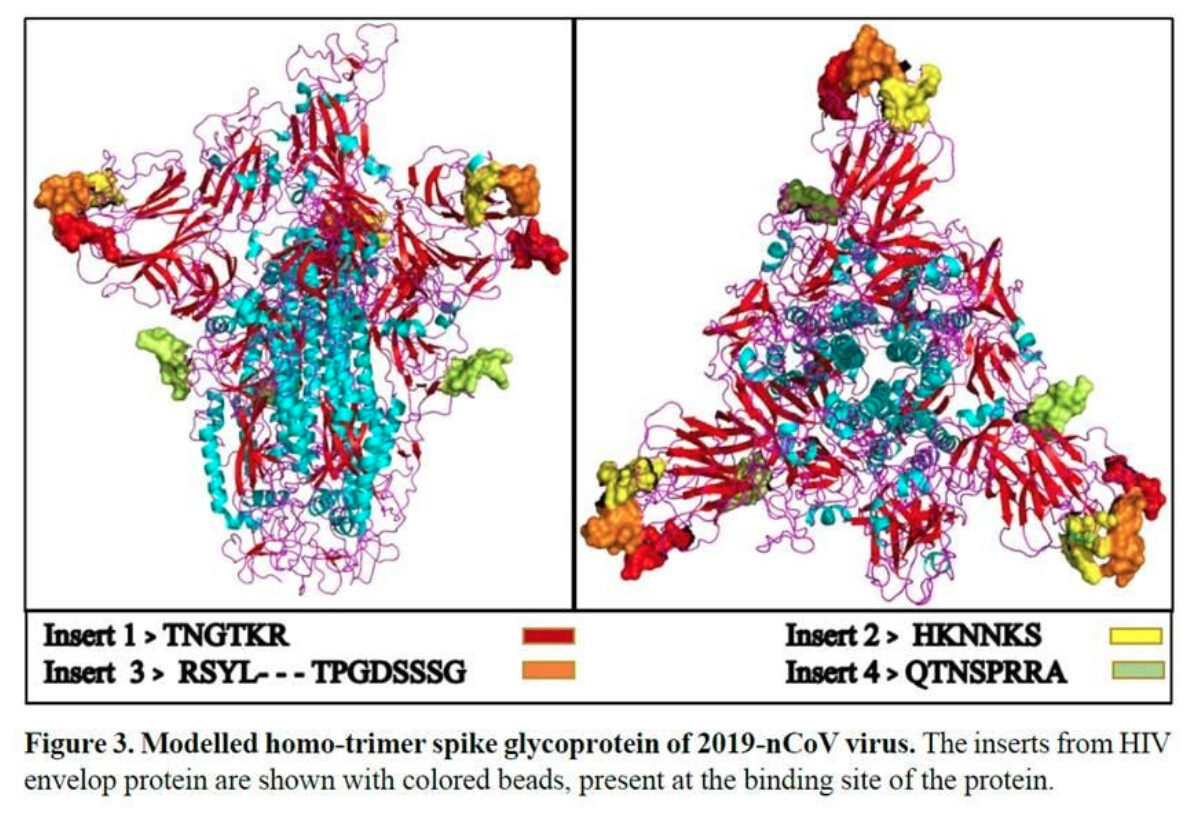
Stunning Finding: S-Protein Insertions From HIV
On Jan. 27, 2020, Prashant Pradhan et. al. from the Indian institute of Technology published a paper
entitled “Uncanny similarity of unique inserts in the 2019-nCoV spike
protein to HIV-1 gp120 and Gag,” which is currently being revised. The
corresponding author of this paper, Professor Bishwajit Kundu, is
specialized in protein genetic and genetic engineering and has published
about 41 papers during the past 17 years on PubMed, including
high-impact biomedical journals.
The authors found 4 insertions in the spike glycoprotein (S) which
are unique to the 2019-nCoV and are not present in other coronaviruses.
“Importantly, amino acid residues in all 4 inserts have identity or
similarity to those of HIV-1 gp120 or HIV-1 Gag. Interestingly,
despite the inserts being discontinuous on the primary amino acid
sequence, 3D-modelling of the 2019-nCoV suggests that they converge to
constitute the receptor binding site. The finding of 4 unique inserts in
the 2019-nCoV, all of which have identity/similarity to amino acid
residues in key structural proteins of HIV-1 is unlikely to be
fortuitous in nature.” (emphasis added) author.
Pradhan et al. added, “To our surprise, these sequence insertions
were not only absent in S-protein of SARS but were also not observed in
any other member of the Coronaviridae family. This is startling as it is
quite unlikely for a virus to have acquired such unique insertions
naturally in a short duration of time.”
“Unexpectedly, all the insertions got aligned with Human
immunodeficiency Virus-1 (HIV-1). Further analysis revealed that aligned
sequences of HIV-1 with 2019-nCoV were derived from surface
glycoprotein gp120 (amino acid sequence positions: 404-409, 462-467,
136-150) and from Gag protein (366-384 amino acid). Gag protein of HIV
is involved in host membrane binding, packaging of the virus and for the
formation of virus-like particles. Gp120 plays crucial role in
recognizing the host cell by binding to the primary receptor CD4. This
binding induces structural rearrangements in GP120, creating a high
affinity binding site for a chemokine co-receptor like CXCR4 and/or
CCR5.”
It is well known that CD4 cells are essential to human immunity and
are the direct targets of the Human Immunodeficiency Virus or HIV. HIV
attaches to CD4 cells, enters and infects them. The virus then turns
each infected CD4 cell into a factory creating more HIV virus until
eventually all CD4 cells are destroyed. People infected with HIV lose
their immunity or defense system which is like a country losing the
function of its army.
If we take a closer look at the 4 insertions of the S-protein in
figure 3 (from Pradhan et. al. 2020 bioRxiv), they are all located on
the binding surface of the protein, seemly designed to be able to bind
to target cell receptor sites. Natural accidental mutation would be
randomly distributed across the whole length of the S-protein. It is
highly unlikely that all of these insertions would coincidentally be
manifested on the binding site of the S-protein.
The article by Pradhan et. al. is a preprint made available through bioRxiv and has not been peer-reviewed.
bioRxiv reports: “This paper has been withdrawn by its authors. They
intend to revise it in response to comments received from the research
community on their technical approach and their interpretation of the
results. If you have any questions, please contact the corresponding
author.”
Clinical Evidence: Patients Have Cytokine Storm with Progressive Decline in Blood Lymphocytes
Are Pradhan et. al.’s findings right or wrong? If correct, the virus
should be able to invade human CD4 T cells and result in corresponding
clinical features. A paper
published in The Lancet on Jan. 24, 2020 by Professor Chaolin Huang
from Jin Yin-tan Hospital, Wuhan, China, et. al., reviewing “Clinical
features of patients infected with 2019 novel coronavirus in Wuhan,
China” supports Pradhan et. al’s conclusions.
Huang analyzed 41 hospital patients admitted with
laboratory-confirmed 2019-nCoV infection as of Jan. 2, 2020. “Only 27
(66%) of 41 patients had been exposed to Huanan seafood market. Common
symptoms at onset of illness were fever (98%), cough (76%), and myalgia
or fatigue (44%); less common symptoms were sputum production (28%),
headache (8%), haemoptysis (5%), and diarrhoea (3%). Dyspnoea developed
in 55% (median time from illness onset to dyspnoea 8·0 days). 63% had
lymphopenia. All 41 patients had pneumonia with abnormal findings on
chest CT. Complications included acute respiratory distress syndrome
(29%), RNAaemia (15%), acute cardiac injury (12%) and secondary
infection (10%). 32% patients were admitted to an ICU and six (15%)
died. Compared with non-ICU patients, ICU patients had higher plasma
levels of IL2, IL7, IL10, GSCF, IP10, MCP1, MIP1A, and TNFα. The
2019-nCoV infection caused clusters of severe respiratory illness
similar to severe acute respiratory syndrome coronavirus and was
associated with ICU admission and high mortality.”
Although low white blood cell counts are common in viral infections,
it is surprising that 63 percent of all infected patients and 85 percent
of those admitted to the ICU had lymphopenia with lymphocyte counts
<1·0 × 109/L. In a study on SARS published March 2004 by C.M. Chu et. al. in the journal Thorax, the mean lymphocyte count was often reported as normal.
On Jan. 22, 2020, two clinical guidelines for the diagnosis and
treatment of Wuhan 2019-nCoV were posted on China websites. One is
“Quick Guide for the Diagnosis and Treatment of New Coronavirus
Pneumonia” authored by the expert group of Tongji Hospital, and the
other is “Instructions for Handling 2019 New Coronavirus” from the Wuhan
Union Hospital of Tongji Medical College of Huazhong University of
Science and Technology. The first guideline clearly points out a “progressive lymphocyte reduction” while the second guideline highlights “the importance of monitoring the absolute value of lymphocytes.” (emphasis added)
Therefore, the observed lymphocyte reduction must be of clinical
significance in a certain proportion of patients. CD4 positive T
lymphocytes constitute a major fraction of all lymphocytes. Although not
a routine test for patients with coronavirus infection, perhaps
monitoring CD4 cell counts would be helpful in 2019-nCoV patients.
Another clinical feature of patients infected with 2019-nCoV is the
high levels of serum cytokines and chemokines, which is defined as a
cytokine storm (Huang et al 2020 Lancet). This is consistent with the
observation from Pradhan et al. that the 2019-nCoV S-protein inducing
structural rearrangements in GP120, creating a high affinity binding
site for a chemokine co-receptor such as CXCR4 and/or CCR5. It is well
known that activating T cell surface receptors can cause a cytokine
storm. Cytokine storms have potential to create significant damage to
organs and bodily tissues. If a cytokine storm occurs in the lungs, for
example, immune cells such as macrophages and fluid may trigger tissue
damage that results in acute respiratory distress and possible death.
The United States Centers for Disease Control stated:
“There is no specific antiviral treatment recommended for 2019-nCoV
infection.” But, there are a few case reports of Wuhan 2019-nCoV
patients benefiting from empiric treatment with anti-HIV drugs such as
lopinavir. More such detailed clinical experience needs to be shared.
Conclusion
There are many scientific questions regarding this novel virus. Based
on recently published scientific papers, this new coronavirus has
unprecedented virologic features that suggest genetic engineering may
have been involved in its creation. The virus presents with severe
clinical features, which make it a significant threat. It is imperative
for scientists, physicians, and people all over the world, including
governments and public health authorities, to make every effort to
investigate this mysterious and suspicious virus in order to elucidate
its origin and to better enable populations in China and around the
world to respond. Yuhong Dong holds a M.D. from Beijing Medical University and a
doctorate in infectious diseases from Beijing University. Dong has 17
years of working experience in viral infectious disease clinical
treatment and antiviral drug research. Dong worked as a doctor in the
First Affiliated Hospital of Beijing Medical University and then later
as a Medical Scientific Expert specialized in antiviral drug clinical
research in Novartis R&D. She currently works as a Chief Scientific
Officer in a Swiss Biotech company. https://www.theepochtimes.com/scientific-puzzles-surrounding-the-wuhan-novel-coronavirus_3225405.html
The source of the novel coronavirus that has led to the lockdown of 34 Chinese cities, and has now spread to 35 countries outside China, is still unknown.
Initial reports from China claimed the source was a live food market
in Wuhan, the capital of Hubei Province, and may have been caused by
bats.
Other reports claimed the source may have been the state-run Wuhan
Institute of Virology near the market, where the virus may have been
leaked from the country’s first top-level “P4” lab, which handles the
most dangerous types of pathogens.
The original report making the claim about the P4 lab as a potential source was published by GreatGameIndia,
a journal on geopolitics and international relations. Other
publications, such as The Washington Times, followed, with additional
claims based on interviews.
While the narrative of the virus coming from the lab hasn’t been
debunked, it has been criticized by several news outlets, since some of
the connections still aren’t proven.
Regardless of where the coronavirus came from, the attention on the
P4 lab has focused a spotlight on the Chinese regime’s alleged
biological warfare programs and is raising questions about the nature of
the P4 lab in Wuhan.
The main argument against the idea that the Chinese regime has a
biological warfare program is the fact that China became a state party
to the Biological Weapons Convention (BWC) in 1984, which would forbid
it from developing biological weapons.
A brief perusal of official documents and strategies, however,
quickly fuels doubt about how closely the Chinese regime has followed
the BWC. A U.S. State Department report
from August 2019 notes the U.S. assessment that China had an offensive
biological weapons program from at least the 1950s to the late 1980s,
and despite signing the BWC, “there is no available information to
demonstrate that China took steps to fulfill its treaty obligations” to
“divert or destroy” any offensive biological weapons it previously
developed.
The report also notes that the Chinese regime “engaged during the
reporting period in biological activities with potential dual-use
applications, which raises concerns regarding its compliance with the
BWC.”
In other words, some research programs done by the Chinese regime
could be used for both peaceful and hostile purposes. The report notes,
“Available information on studies from researchers at Chinese military
medical institutions often identify biological activities of a possibly
anomalous nature … with potential dual-use applications.”
Rick Fisher, a senior fellow at the International Assessment and
Strategy Center and an Epoch Times contributor, said in an interview
that U.S. assessments in the government and intelligence communities
hold that “China has been developing these weapons all along.”
Fisher noted that it was suspected that biological warfare programs
in China were connected to leakages of the SARS virus, following its
outbreak in 2002 and 2003, and to a viral outbreak in the late 1980s in
Xinjiang.
“They are still disasters—breakdowns—in the process of these
laboratories that allowed for these very harmful viruses to leak out
into the public and cause extensive, but clearly unnecessary, death,”
Fisher said.
The P4 lab in Wuhan has connections to the Chinese military, the
People’s Liberation Army. When the U.S.-based company Gilead Sciences
recently sent a new drug (remdesivir) to China that could possibly treat
the novel coronavirus, the Wuhan Institute of Virology quickly moved to
apply for a patent.
In a Feb. 4 statement
published on the institute’s website about the patent, the institute
notes it conducted research alongside the National Academy of Military
Medical Research Institute of Emergency Medicine for Prevention and
Control of Drugs. It also notes ties to the Prevention Engineering
Technology Research Center of Military Medical Research Institute, and
to the National Institute of Emergency Medicine Control and Engineering
Research Center for Military Medical Research.
The Wuhan P4 lab is part of the Chinese Academy of Sciences, which has close ties to the Chinese military in its research programs.
Meanwhile, Chinese military doctrine has identified biological
warfare as a key part of the regime’s military strategies—particularly
in any war scenarios with the United States. Among the key programs is
its Assassin’s Mace (“Sha Shou Jian”) strategy.
Michael Pillsbury, a Pentagon consultant, warned
of the strategy in his 2016 book “The Hundred-Year Marathon,” in which
he noted the only time China won in a simulated war game with the United
States, the China team used the Assassin’s Mace strategy. He wrote,
“whenever the China team used conventional tactics and strategies,
America won—decisively. However, in every case where China employed
Assassin’s Mace methods, China was the victor.”
Fisher said that Assassin’s Mace is designed around using various
unconventional weapons in conjunction for a brutal surprise attack, and
that “when used at the right time, and targeted against a specific
weakness of the enemy, can result in the rapid collapse of that enemy’s
military threat.”
He also noted that Chinese military officials haven’t shied away from
discussing the use of brutal attacks and weapons, including biological
weapons. Some of the statements are so brazen and extreme, however, that
many in the U.S. defense analyst community tend to dismiss them.
In regard to rumors about the new coronavirus spreading in China, he
noted that while they’re still unproven, they also shouldn’t be written
off without some investigation.
“Reputable scientists are beginning to coalesce around the idea that
at a minimum, the coronavirus that we’re facing today is the product of a
laboratory [and] not the product of some kind of naturally occurring
process,” Fisher said.
He said the “developing consensus that this coronavirus is
a man-made virus naturally links this to China’s biowarfare
capabilities and programs.”
“The world should take this as a very serious possibility,
and it should affect our policy and relationships with the People’s
Republic of China.”
Investors are maintaining their enthusiasm with coronavirus-related stocks, driving Moderna (MRNA+15.6%) up on almost triple normal volume. At a news conference today, a U.S. health official stated that
there have been no “glitches” in development to date with the company’s
investigational coronavirus vaccine (company is working with NIH).
Two weeks ago, it announced funding from a public-private coalition to support the manufacture of the vaccine.
Fellow mRNA therapeutics developer Alnylam Pharmaceuticals (ALNY+3%) is up as well, albeit on average volume.
Update: The official stated that the vaccine could be ready for a Phase 1 study in 2 1/2 months.
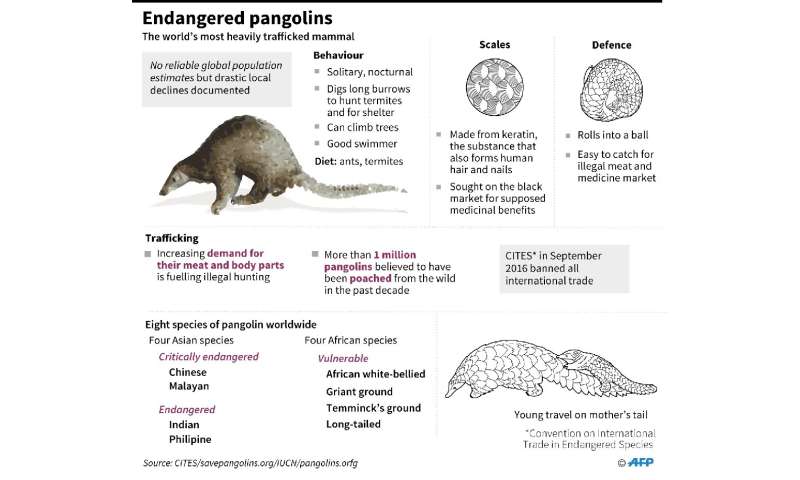
Researchers at the South China Agricultural University have
identified the scaly pangolin as a ‘potential intermediate host’ for the
virus
Chinese researchers investigating the animal origin of the deadly
coronavirus outbreak in China said Friday the endangered pangolin may be
the “missing link” between bats and humans, but other scientists said
the search may not be over.
An earlier study—since discredited—pointed to snakes, and there
remain numerous candidate species in the Wuhan wildlife market thought
to be ground zero of the epidemic.
The SARS outbreak of 2002-3, involving a different strain of
coronavirus, was transferred to humans by the civet, a small mammal
prized in China for its flesh. Missing link: A pangolin?
Many animals are capable of transmitting viruses to other species,
and nearly all strains of the coronavirus contagious to humans
originated in wildlife.
Bats are known carriers of the latest strain of the disease, which
has infected at least 31,000 people and killed more than 630 worldwide,
mostly in China where the outbreak originate.
A recent genetic analysis showed that the strain of the virus
currently spreading among humans was 96 percent identical to that found
in bats.
But according to Arnaud Fontanet, from France’s Pasteur Institute, the disease likely didn’t jump straight from bats to humans.
“We think there’s another animal that’s an intermediary,” he told AFP.
Several studies have shown that the bat-bourne virus lacks the
necessary hardware to latch on to human cell receptors. But it’s still
not clear which animal is the missing link.
Fontanet believes the intermediary was “probably a mammal,” possible belonging to the badger family.
After testing more than 1,000 samples from wild animals, scientists
at the South China Agricultural University found the genome sequences of
viruses in pangolins to be 99 percent identical to those on coronavirus
patients, the official Xinhua news agency reported.
But other experts urged caution.
“This is not scientific evidence,” said James Wood, head of the
department of veterinary medicine at the University of Cambridge.
“Investigations into animal reservoirs are extremely important, but
results must be then be published for international scrutiny.”
“Simply reporting detection of viral RNA with sequence similarity of 99+ percent is not sufficient,” he added. Wild goose chase?
To conclusively identify the culprit, researchers would need to test
each species that was on sale at the market—a near impossibility given
that it’s now permanently closed.
Martine Peeters, a virologist at France’s Institute for Research and
Development (IRD), worked on the team that identified the host animal of
the Ebola virus during recent epidemics.
Graphic on pangolins, the world’s most heavily trafficked mammals.
They found that it was indeed a bat that passed the virus on to
humans, and Peeters believes that’s likely to be the case this time
around.
During her Ebola research, “we collected thousands of bat dropping from several sites in Africa,” Peeters told AFP.
Fontanet said that Chinese researchers were doing likewise now.
“They say they’ve analysed samples from a rubbish truck,” he said.
“They don’t say which, but I think it’s likely to have been excrement
that was just lying around.” Why does it matter?
While it may be too late for this outbreak, identifying the carrier
animal for the novel coronavirus could prove vital in preventing future
flare ups.
China for example outlawed the sale of civet for food in the wake of the SARS epidemic.
Eric Leroy, a virologist and vet at the IRD said the search could
well turn up a result quickly like in the case of SARS. Equally, it
could take years.
“With Ebola, research started in 1976 and we didn’t see the first results published until 2005,” he told AFP.
One determining factor could be what percentage of the same species are infected.
“If that’s low, less than one percent for example, that’s obviously
going to lower the chance you stumble upon an infected animal,” said
Leroy. Prevent future outbreaks?
For Fontanet, coronavirus is just the latest example of the
potentially disastrous consequence of humans consuming virus-carrying
wild animals.
He said that China needed to “take pretty radical measures against the sale of wild animals in markets.”
Beijing has prohibited the practice, but only moved to do so last month, when the outbreak was already out of control.
“Each time, we try to put out the fire, and once it’s out we await
the next one,” said Francois Renaud, a researcher at the Paris-based
National Centre for Scientific Research.
He recommended compiling a watch list of all animals that could potentially transmit viruses to humans.
“You need to see epidemics before they come, and therefore you need to be proactive,” he said. https://medicalxpress.com/news/2020-02-pangolin-potential-link-coronavirus.html
Forty health care workers were infected with the novel coronavirus by
patients at a single Wuhan hospital in January, a new study has found,
underscoring the risks to those at the frontlines of the growing
epidemic.
One patient who was admitted to the surgical department was presumed to have infected 10 health care workers, according to the paper that was authored by doctors at the Zhongnan Hospital of Wuhan University and published in the Journal of the American Medical Association (JAMA) on Friday.
Seventeen patients who were hospitalized for other reasons also
became infected by the coronavirus. A total of 138 patients got the
virus in a period spanning January 1 to January 28, with
hospital-associated transmission accounting for 41 percent of all cases.
The study comes just hours after a Chinese doctor who was punished
for raising the alarm about the coronavirus died from the
pathogen—sparking an outpouring of grief and anger over a worsening
crisis that has now killed more than 630 people.
Li Wenliang, 34, sent out a message about the new coronavirus to
colleagues on December 30 in Wuhan but was later among a group of people
summoned by police for “rumor-mongering.”
He later contracted the disease while treating a patient.
Of the 40 infected health care workers in the JAMA study, 31 worked on general wards, seven in the emergency department, and two in the ICU.
The example of the patient presumed to have infected 10 health workers
highlighted the high level of danger within hospitals during the first
phase of the epidemic, even though overall it is currently estimated
that each patient infects on average 2.2 others.
“If true, then this confirms that some patients
are likely to be far more infectious than others, and this poses
further difficulties in managing their cases,” said Michael Head, a
global health expert at the University of Southampton said in a comment
to the UK’s Science Media Centre.
Medical staff at the epicenter of the virus are overstretched and
lack sufficient protective gear, the deputy governor of Hubei province
admitted Thursday. https://medicalxpress.com/news/2020-02-coronavirus-infected-staff-wuhan-hospital.html
New York state’s top health officials faced
off with state legislators Wednesday, backing the governor’s plan to
shift more Medicaid costs to local governments.
The state’s plan has met fierce opposition from Mayor Bill
de Blasio’s administration, which has estimated the proposal could cost
the city as much as $1.1 billion.
A state budget spokesman told Crain’s the
state estimates the city would pay only $221 million in the case that it
overruns a 2% property tax cap.
The spokesman for the state’s budget office
said the city is calculating its potentially higher share of costs
incorrectly and is inflating how much Medicaid spending will rise. The
state pegs the growth rate at 3%.
The state and city, he said, had once worked together to
hold down spending and the governor’s plan would “revive that
partnership as we return spending growth in the Medicaid program to 3%
or less.”
Gov. Andrew Cuomo this month accused local governments of
suffering from a “blank check syndrome” that led them to let Medicaid
spending go unchecked, helping create a $6.1 billion state budget
imbalance for fiscal 2021, which begins April 1.
Dr. Howard Zucker, the state health commissioner, and state
Medicaid Director Donna Frescatore had little to share with legislators
about how they plan to lower the Medicaid budget by $2.5 billion and who
will serve on a proposed Medicaid redesign team.
New York City and counties around the state have said their
role in the Medicaid program is limited to determining whether people
signing up meet financial eligibility requirements. They say the state,
with the federal government, sets the eligibility standards and the
benefits package.
Frescatore told legislators that local governments could
help manage spending by ensuring Medicaid enrollees aren’t hiding assets
that make them ineligible for the health program, which is for the poor
and the disabled.
“We share in the administration of the Medicaid program,” she said.
The state froze counties’ level of Medicaid spending in
2013, but Cuomo proposed the counties be responsible for paying for any
growth in Medicaid costs above 3%. For New York City, where Medicaid
costs grew about 7% in the 2019 fiscal year, the city would be on the
hook for about $646 million, according to city officials.
If New York City were to raise property taxes above the
state-mandated 2% cap, the city would be responsible for the full 7%
increase, costing $1.1 billion, according to the city’s estimate.
The city has been working to save the state money—generating
$180 million in savings, including $90 million in state spending, in
the past three years by identifying people who shouldn’t have been
eligible for Medicaid—Steven Banks, commissioner of the city Human
Resources Administration, said Wednesday during a call with reporters.
About half of city residents signing up for Medicaid do so
through the HRA, with the other half using the New York State of Health
marketplace.
Frescatore made the case that local governments play a
bigger role. She said the city and counties manage the care plans of
900,000 Medicaid beneficiaries who are enrolled in fee-for-service
Medicaid—which means the state, not a Medicaid insurer, pays their
claims. That population represents about $1.3 billion in monthly costs,
she said.
First Deputy Mayor Dean Fuleihan called that argument
misleading and noted that the greatest cost driver has been the managed
long-term care program, in which private insurers approve oversee care.
Fuleihan said the consequences to the city would be devastating if it had to absorb an extra billion dollars in costs.
“This is an incredibly large amount of money that is being
shifted to us on a program that’s completely run by the state,” he said.
It’s been a busy year for Sanofi: It’s been rejigging deals with the
likes of Regeneron and bought out a biotech in the form of Synthorx.
In its fourth-quarter/full-year update Thursday, analysts, as ever,
had more M&A on their minds. Sanofi spent $2.5 billion on that
Synthorx deal late last year, nabbing an IL-2 drug the pharma thinks can
become a foundation of immuno-oncology combinations. In the future,
more deals may take a similar shape.
CEO Paul Hudson was asked whether the timing of the deal was
deliberate, in order to dovetail with its Capital Markets Day. “As much
as we love you all as an audience, we didn’t do a deal just to achieve a
good news flow for Capital Markets Day,” he said.
“I think this deal has been tracked for a while and for the
fundamental belief that it could, although early, if it works, it could
change what happens in oncology and particularly the I-O/I-O piece. I
think [R&D lead John Reed] beautifully described the Synthorx deal
with putting gas in the tank. And I think as we get closer to launch in a
few years, people will be excited to have a new approach to what could
become a definitive play in combination.”
On future deals, he said: “And I think, you know, it’s hard to say,
but I think we are more excited about mechanisms, new mechanisms,
complementary mechanisms, things in combination. [Reed] mentioned the
CD38 and the PD-1 in combination. There are BD [business development]
opportunities where you can really get to ramp up your own existing
pipeline by pulling forward incredible and unique data. So, we are
excited about that.
“Really, it’s an interesting time for the company because whilst we
go on this BOI journey and we have between vaccines and dupilumab, we
have an opportunity to be able to maintain a really positive growth
trajectory. So, it allows us, I think, from a BD or even M&A
perspective, to go after science in a more determined fashion.
“It’s not necessary. It doesn’t mean we will never do these things.
But I think we are more interested in things like we have just done. And
hopefully, you will see over the months and years that we do more like
that. But we will see.”
One of the bigger changes for the French Big Pharma in the last year
has been its pact with Regeneron: Last January, Sanofi paid Regeneron
$462 million (€404 million) to exit the immuno-oncology pact the two
formed back in 2015.
The move gave Sanofi the right to opt in to two bispecific programs
but otherwise left each company free to operate independently. And,
during the fourth quarter in December last year, the pair also announced
the companies will restructure their 12-year-old partnership into a
royalty-based agreement for PCSK9 med Praluent and rheumatoid arthritis
med Kevzara, with Regeneron taking over U.S. rights to the former and
Sanofi snagging global rights to the latter.
Responding to probing from analysts over why the pair changed up
their pact, Sanofi’s CFO Jean-Baptiste de Chatillon said: “These changes
are simplification on reduced governance on some extra costs. So, on
both sides, it is accretive. Of course, for us, it’s less significant.
So of course, it is taken into account in this guidance. And since we
broadly decided this change in December, as we said in the CMD, so yes,
it’s a positive. It’s embedded into our guidance. But it’s not so
significant in the overall scheme for Sanofi. But it goes in the right
direction.”
Hudson explained: “I think there’s a great spirit, by the way,
between ourselves and Regeneron in trying to simplify things. We
recognize that it’s better to do these things like this and be more
agile in a partnership and I think we will only get benefits from that.
Some will be financial, of course, both sides ultimately. But often, it
will just be speed. It will become important.” https://www.fiercebiotech.com/biotech/sanofi-c-suite-explain-regeneron-deal-simplification-ramping-up-its-pipeline
 Clinical Evidence: Patients Have Cytokine Storm with Progressive Decline in Blood Lymphocytes
Clinical Evidence: Patients Have Cytokine Storm with Progressive Decline in Blood Lymphocytes