It is too early to consider widespread use of a second COVID-19 vaccine booster dose, according to the European Centre for Disease Prevention and Control (ECDC) and EMA’s COVID-19 task force (ETF).
The official word from the EU authorities is that for now a fourth dose of Pfizer/BioNTech’s Comirnaty or Moderna’s SpikeVax – the preferred booster vaccines in Europe – should only be used in adults aged 80 years and over and people with compromised immunity.
There is no clear evidence of a benefit of a second booster in other age groups with normal immune systems, or that in younger adults (aged below 60) “that vaccine protection against severe disease is waning or that there is an added value of a fourth dose.”
They organisation’s haven’t ruled out re-vaccination campaigns in the autumn however – which could be pivotal if Pfizer/BioNTech and Moderna are to meet their expectations for sales of the two mRNA-based shots in 2022.
Ultimately, the decision on whether to roll out fourth doses will depend on EU member states, as the conclusions of the ECDC and ETF are advisory only.
The recommendation comes as EU and European Economic Area (EEA) countries are seeing a steady increase in COVID-19 cases, driven by the Omicron variant, with just under 2,000 cases per 100,000 people on average.
At the same time, the average death rate has been falling, although it has been creeping up in recent days in some countries, including Germany and Italy.
Meanwhile, the UK – which relaxed restrictions earlier – reported 780 deaths where COVID-19 was mentioned on the death certificate in the seven days leading up to 25 March.
“Vaccination against COVID-19 remains the most effective way to prevent severe illness during the current pandemic, including severe illness caused by the Omicron variant,” said the EMA in a statement.
FDA gives first thinking on updating vaccines
In the US meanwhile, the FDA has given its first indication on what it may expect from vaccine developers who intend to update their COVID-19 shots in response to the emergence of new variants.
The agency laid out a “tentative” framework at a meeting with its Vaccines and Related Biological Products Advisory Committee (VRBPAC) yesterday, saying it hopes it will stimulate discussion on the topic.
The framework anticipates that the VRBPAC would provide advice on changes to the composition of vaccines, based on review of epidemiological data from the US in a similar manner way to the way the make-up of the annual flu shot is decided, taking into account other factors including manufacturing capacity and clinical data on new candidates.
“FDA considers experience to date with COVID-19 vaccines insufficient to support authorisation or approval of a modified vaccine based on manufacturing information alone,” said the agency in briefing documents for the meeting.
Novartis’ generics unit Sandoz has moved on to the next stage of a collaboration with Ares Genetics, which is focusing on the use of artificial intelligence to track antimicrobial resistance (AMR), improve diagnoses and guide the most effective use of antibiotics.
Sandoz and Ares – a subsidiary of OpGen – started working together in 2018, and with the extension will continue the project until the end of January 2025.
During the initial stage of the collaboration, Ares developed a an AI-powered anti-infectives platform using microbiological lab techniques and bioinformatics that can be used to identify effective antimicrobial compounds or combinations against specific pathogens, which Sandoz can use to inform its “portfolio and commercial decisions.”
Now, the aim is to layer in genomics surveillance using Ares’ next-generation sequencing (NGS) expertise, improving the monitoring of resistant pathogens and making sure that antibiotics are prescribed wisely.
“AMR, which is now estimated to directly account for nearly 1.3 million deaths worldwide every year, is an unprecedented threat to global public health,” said Sandoz chief executive Richard Saynor in a statement on the revised collaboration.
The World Health Organization (WHO) meanwhile has warned that, without new treatments, AMR could kill 10 million people every year by 2050.
“As the world’s leading provider of generic antibiotics, our goal at Sandoz is to play a key role in overcoming this growing threat,” he added.
Sandoz’ parent Novartis exited novel antibiotics R&D four years ago, joining an exodus from the sector by big pharma companies that has raised fears of increasing numbers of infections that will resist all current drugs.
The generics unit has been however extending its product range in the category, for example last year it spent $350 million on GlaxoSmithKline’s cephalosporin franchise, including Zinnat (cefuroxime axetil), Zinacef (cefuroxime) and Fortum (ceftazidime).
The big challenge is making sure these drugs are used in the best way, to conserve their efficacy as new therapies come through the pipeline, and big part of the Ares collaboration will be working out how antibiotics may be repurposed to tackle specific infections, said Saynor.
“Diagnostic and surveillance data not only have the potential to empirically inform antibiotic stewardship today, but also hold the potential to expand our options in treating AMR in the future,” added Dr Arne Materna, Ares’ managing director and CEO.
“Supplying up-to-date AMR data…promotes the discovery of effective conventional antimicrobial compounds and combinations thereof, and may ultimately allow their targeted repurposing as treatment alternatives that could help preserve last-resort therapies,” he added.
Pfizer Inc said on Thursday it would buy privately-held ReViral Ltd in a deal worth as much as $525 million including milestone payments, to gain access to experimental drugs against the respiratory syncytial virus (RSV).
The deal marks the U.S. drugmaker's second acquisition in less than six months to boost its drug portfolio, after a $6.7 billion takeover of Arena Pharmaceuticals in December.
RSV, a common respiratory virus that causes cold-like symptoms, is a cause of pneumonia in toddlers and the elderly.
London-based ReViral has four RSV therapies in its pipeline, with lead product candidate sisunatovir and another treatment currently in mid-stage studies.
Pfizer's own RSV vaccine candidate is in late-stage studies now.
"Currently, treatment options for RSV are extremely limited and focus primarily on supportive care," said Annaliesa Anderson, chief scientific officer of Bacterial Vaccines and Hospital at Pfizer.
Evan Seigerman, analyst at BMO Capital Markets, says the deal is encouraging for M&A activity in biopharma, but not so impactful for Pfizer in the near-term. "The transaction does not materially impact Pfizer's ability to do a larger transaction or other smaller deals."
The acquisition could potentially signal a return to M&A for biopharma companies, especially in an environment where companies seem to face hurdles going public, said Truist analyst Robyn Karnauskas.
Aptinyx Inc. (Nasdaq: APTX), a clinical-stage biopharmaceutical company developing transformative therapies for the treatment of brain and nervous system disorders, today announced results from a Phase 2b clinical study evaluating the effects of NYX-2925 in patients with painful diabetic peripheral neuropathy (DPN). NYX-2925 did not achieve statistically significant separation from placebo on the study’s primary endpoint, which assessed the change from baseline in average daily pain on the numeric rating scale (NRS) during week 12.
"We are clearly disappointed that the study did not meet its primary endpoint," said Andy Kidd, M.D., president and chief executive officer of Aptinyx. "We appreciate the contributions of patients, investigators, and the entire team that worked on the study. Unfortunately, the data from this study do not currently point to a path forward in development for painful DPN."
"We continue to believe, however, that NYX-2925 can offer a novel therapeutic approach for fibromyalgia, a disorder fundamentally characterized by abnormal pain processing in the brain. To this end, we look forward to reporting data from our ongoing fibromyalgia Phase 2b study in early to mid Q3. We continue to have confidence in our platform and pipeline and will manage our existing balance sheet to enable readouts across our currently ongoing Phase 2 studies in fibromyalgia, cognitive impairment, and PTSD."
Moderna, Inc., (NASDAQ:MRNA) a biotechnology company pioneering messenger RNA (mRNA) therapeutics and vaccines, and the nonprofit scientific research organization IAVI today announced a new collaboration to employ mRNA technology to meet the challenge of a range of global health threats. These diseases - HIV/AIDS, tuberculosis (TB), antimicrobial-resistant enteric infections, and COVID-19 - are estimated to have caused at least 95 million new infections and more than 4 million deaths in 2020 alone. The collaboration combines the power of Moderna's mRNA platform and IAVI's expertise in discovery and product development to advance vaccines and antibodies designed to be globally accessible, especially in low-income countries where the targeted diseases have high incidence and prevalence.
Throughout the pandemic, the media have eagerly compared Covid statistics between different countries. But such comparisons are often deceptive.
Take, for example, the use of Covid case counts. These depend not only on the number of people infected but also on the amount of testing performed. While useful for evaluating whether cases are increasing or decreasing within a particular country, they are deceptive when comparing countries. If we truly wanted to know, it would be easy, through random seroprevalence surveys that measure the proportion of people with antibodies. But not all governments have been eager to conduct these surveys, while some scientists have even got into trouble for doing them.
Comparing Covid death tolls between countries, as many journalists have done, is equally problematic. A Covid death is defined differently in different countries, with varying testing thresholds and a different maximum number of days required between a positive test and death. Therefore, countries vary in the proportion of reported Covid deaths that, firstly, are genuinely due to Covid, secondly, have Covid as a contributing factor but not as the main cause, and, thirdly, that show whether an individual died with rather than from Covid.
This confusion can lead to an over-reporting of Covid deaths. If we truly wanted to know, it would be easy. We could randomly select some reported deaths and evaluate their medical charts. Surprisingly few such studies have been performed.
Other countries have under-reported Covid mortality. For example, Nicaragua has reported very few Covid deaths. However, from reports that carpenters were working overtime to fulfill the burgeoning demand for wooden burial coffins in 2020, we certainly know that large numbers of people were dying from Covid there.
The media have also been tripped up by several significant variables. For example, the pandemic arrived and surged at different times in different countries, and even within countries – as you would expect from any pandemic. During the first wave in 2020, some countries were praised for their strict lockdowns and low Covid mortality, but subsequent waves hit some of them so badly that they now have among the highest mortality numbers in the world.
Covid is also seasonal. This means that it follows different seasonal patterns in different regions. This fact also tripped up journalists. In 2021, many journalists (often New York-based) blamed the seasonal summer wave in the southern United States on Covid policies. But when the subsequent winter wave arrived in the northern US, it was clear to all that it was a seasonal effect.
Extreme Covid restrictions, such as those imposed by Australia, Hong Kong and New Zealand, certainly kept the virus at bay for a while. But that just postponed the inevitable. All countries have to work their way through the pandemic sooner or later.
Moreover, the focus on Covid cases, death counts and so on, ignores the collateral public-health damage from Covid restrictions. These have contributed to deaths from other diseases, and such deaths are just as tragic as Covid deaths. A basic public-health principle is that one should never focus on one single disease but consider public health as a whole. Even if the lockdowns reduced Covid mortality, for which there is scant evidence, one must also consider the harm that the lockdowns caused on other health conditions such as worsening cardiovascular-disease outcomes, missed cancer screening and treatment, lower childhood-vaccination rates, and deteriorating mental health.
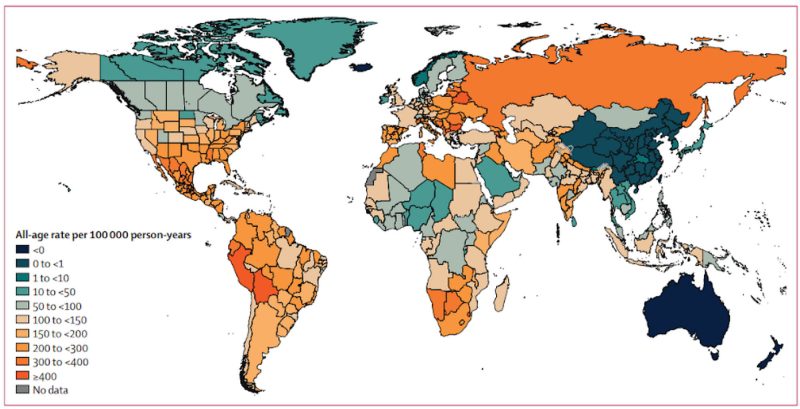
Given all this, how should we compare countries’ handling of the pandemic? While not perfect, the best way is to compare excess mortality; that is, the observed total number of deaths during the pandemic minus the average number of deaths observed during the years before the pandemic. Since the pandemic is not yet over, we do not have the full picture yet. Nevertheless, a recent article in the Lancetpresents excess deaths for 2020-2021 for almost every country in the world. The map below shows the results:
Global distribution of estimated excess-mortality rate due to the Covid-19 pandemic, for the cumulative period, 2020-21
What can we learn from these data? How did three main pandemic strategies compare: (a) a do-nothing, let-it-rip approach; (b) focused protection of high-risk older people with only limited restrictions on others, and (c) general lockdowns and restrictions on all age groups?
Belarus and Nicaragua did little to protect older people and they imposed very few Covid restrictions. They also report among the lowest Covid mortality numbers. From the excess-mortality data, it is clear that they did not escape the pandemic. Nicaragua had 274 excess deaths per 100,000 population, which is precisely the same as the regional average. Belarus had 483 excess deaths per 100,000, higher than the average for either Eastern Europe (345) or Central Europe (316).
In Western Europe, the Scandinavian countries had the lightest Covid restrictions while they tried to protect their older high-risk population. Sweden was heavily criticised for this by the international media. The Guardian, for instance, reported in 2020 that life in Sweden felt ‘surreal’, with ‘couples stroll[ing] arm in arm in the spring sunshine’. Many journalists, politicians and scientists expected that the lighter Scandinavian touch would lead to disaster. That did not happen. Sweden has among the lowest reported Covid mortality numbers in Europe. Of the European countries with more than one million people, Denmark (94), Finland (81), Norway (7), and Sweden (91) are four of only six countries with excess mortality less than 100 per 100,000 inhabitants, the other two being Ireland (12) and Switzerland (93).
What about the UK, with its more heavy-handed Covid restrictions? Compared to the Western European average of 140 excess deaths per 100,000, England had 126, Scotland 131, Wales 135, and Northern Ireland 132.
In the US, South Dakota imposed few Covid restrictions, while Florida tried to protect older people without too many restrictions on the general population. Did that result in the predicted disaster? No. Compared to the national average of 179 excess deaths per 100,000, Florida had 212 while South Dakota had 156.
Countries in Sub-Saharan Africa report the lowest Covid mortality globally, with seven deaths per 100,000, but their excess mortality is 102 deaths per 100,000. Without age-stratified numbers, we do not know how much of this difference is due to the under-reporting of Covid deaths as opposed to the harsh lockdowns that caused malnutrition and starvation among the poor.
The countries with the highest excess mortality are Bolivia (735), Bulgaria (647), Eswatini (635), North Macedonia (583), Lesotho (563), and Peru (529), with no other countries topping 500 excess deaths per 100,000. According to the Oxford Stringency Index, Peru has endured some of the world’s harshest Covid restrictions while those in Bulgaria, Eswatini and Lesotho were closer to the average. Bolivia had very harsh restrictions in 2020, but not in 2021.
Though excess-mortality data should still be treated with caution, they do show that the few places that rejected draconian Covid restrictions did not see the catastrophic death counts that some had predicted.
The pandemic is not over, and with different seasonal patterns in different regions and different levels of population immunity, some countries have not yet seen the worst. For example, 40 per cent of all reported Covid deaths in Denmark occurred during the first 80 days of 2022. Denmark is not as extreme a case as Hong Kong, where 97 per cent of all reported Covid deaths have been in 2022.
The biggest weakness of excess-mortality statistics is that while they count Covid deaths, they do not fully capture the deaths, not to mention the collateral public-health damage, that come from Covid restrictions themselves. Missed cancer screenings and treatments do not lead to immediate deaths, but a woman who missed her cervical cancer screening may now die three or four years from now instead of living another 15 or 20 years. The mortality statistics do not reflect non-fatal collateral damage such as increasing mental-health problems or missed educational opportunities, either. Those harms need to be tallied and addressed in the years to come.
Politicians argued that the draconian lockdowns were needed to protect lives. From the excess-mortality data, we now know they were not. Instead, they have contributed to the enormous collateral damage that we will have to live with for many years to come. It is tragic.
In her classic book, The March of Folly, historian Barbara Tuchman describes how nations sometimes pursue actions contrary to their interests. She starts with Troy and the Trojan horse and ends with the US and the Vietnam War. By ignoring basic, long-standing principles of public health during the pandemic, most nations marched down the path of folly together. The leaders of those nations will be fine, except for some early retirements. The devastation on children, the poor, the working class and the middle class, on the other hand, will take decades to repair.
Authors
Martin Kulldorff, Senior Scholar of Brownstone Institute, is an epidemiologist and biostatistician specializing in infectious disease outbreaks and vaccine safety. He is the developer of Free SaTScan, TreeScan, and RSequential software. Most recently, he was professor at the Harvard Medical School for ten years. Co-Author of the Great Barrington Declaration.
Jay Bhattacharya, Senior Scholar of Brownstone Institute, is a Professor of Medicine at Stanford University. He is a research associate at the National Bureau of Economics Research, a senior fellow at the Stanford Institute for Economic Policy Research, and at the Stanford Freeman Spogli Institute.