Clinical-stage oncology companyALX Oncologyis dropping trials for two of its anti-CD47 programs after disappointing efficacy findings.
In its second-quarter earnings report on Thursday, the San Francisco-based company announced an end to its ASPEN-02 and ASPEN-05 programs, which were evaluating the efficacy of its CD47-inhibitor evorpacept. The protein works by binding to receptors on cancer cells that can potentially enhance the action of both chemotherapy drugs, as well as the body's natural immune response.
The two programs were assessing the effectiveness of evorpacept in concert with chemotherapy drugs to treat myelodysplastic syndrome and acute myeloid leukemia, respectively. Initial findings were promising. The combination of evorpacept and chemotherapy drugs—Bristol Myer Squibb’s azacitidine and AbbVie and Genentech’s venetoclax—proved more effective in combination than apart in early trials for myelodysplastic syndrome, as well as acute myeloid leukemia.
However, later findings in the ASPEN-02 trial led ALX to reconsider “as the evorpacept combination did not substantially improve upon the historical activity of azacitidine alone” in the 45 patients being tested, the report said. In addition, because of the “close mechanism of action with azacitidine” in the two cancers, the company decided not to pursue the ASPEN-05 program any further either.
“Based upon this decision, resources originally earmarked for these trials will be allocated to support the company’s ongoing programs evaluating combinations with anti-cancer antibodies and PD-1/PD-L1 immune checkpoint inhibitors,” ALX said.
CEO Jaume Pons said the company remains “steadfast" in its "conviction that the primary mechanism of action of evorpacept is unique compared to other CD47 blockers when combined with anti-cancer antibodies, ADCs, or immune checkpoint inhibitors.”
ALX is going ahead with its Phase II ASPEN-06 trial, evaluating the efficacy of evorpacept in concert with Herceptin, CYRAMZA, and paclitaxel for patients with HER-2-positive gastric and gastroesophageal junction cancers, as well as its Phase II testing evorpacept with KEYTRUDA, and a Phase I/II trial testing it with SARCLISA.
The news comes only weeks after Gilead Sciences ended Phase III trials of its own anti-CD47 investigation focusing on magrolimab “due to futility based on a planned analysis.” The monoclonal antibody was an ambitious target and big risk for the company, which spent just shy of $5 billion acquiring Forty Seven and its lead candidate.
These companies are not alone in running into trouble investigating CD47-based treatments. AbbVie pulled out of its partnership with I-Mab in August 2022 to study lemzoparlimab, while Chinese-biotech Zai Lab deprioritized its own candidate that same month citing the “competitive landscape.”
Meanwhile, Forty Seven's founders have pursued other avenues, launching Bitterroot Bio to investigate anti-CD47 heart medications and receiving backing from major donors such as ARCH, Deerfield, and GV, Google’s venture capital arm.
China has lifted pandemic-era restrictions on group tours for more countries, including key markets such as the United States, Japan, South Korea and Australia in a potential boon for their tourism industries.
The decision was announced by China's culture and tourism ministry on Thursday, effective immediately.
Prior to the pandemic, mainland Chinese tourists spent more than any other country's tourists when abroad, clocking up a combined $255 billion in 2019 with group tours estimated to account for roughly 60% of that.
Their absence since the pandemic has led to financial troubles for many tourism-dependent businesses around the globe.
U.S. Commerce Secretary Gina Raimondo described the step as "a significant win" for the U.S. tourism industry and said it was the result of "months of hard work" between the U.S. Commerce Department and the Chinese culture and tourism ministry.
Germany and Britain were also among the countries for which restrictions were lifted but Canada, which has had especially politically fraught relations with China of late, was not reinstated.
It was China's third list of countries to receive approvals. The first batch approved in January included 20 countries such as Thailand, Russia, Cuba and Argentina. The second batch in March included 40 countries, among them Nepal, France, Portugal and Brazil.
China has never explained its staggered approach to approvals but analysts have noted that the countries taking time to gain approval have had more political and/or trade tension with the world's second-largest economy.
The move was also welcomed by Japanese Prime Minister Fumio Kishida as well as tourism ministers in South Korea and Australia, who said it would boost their economies.
"This is another positive step towards the stabilisation of our relationship with China," said Australian Trade and Tourism Minister Don Farrell.
Just how much outbound Chinese tourism will bounce back for the latest group of countries remains to be seen. Expectations that demand would come roaring back after borders were re-opened have to date been largely unfulfilled.
International flights in and out of China have recovered to only 53% of 2019 levels as of July.
That is in large part due to staffing issues for many global airlines that have limited the flying of more routes, slow visa issuance for Chinese travellers amid backlogs in many Western countries, and a sputtering domestic economy that is discouraging many holidaying Chinese from spending big.
In response to the news, some Chinese said online that they were less than enthusiastic about international trips.
"I don't want to go; I feel domestic travel is pretty good, such as the beautiful scenery in Xinjiang and the Northeast and the food is cheap," said one Weibo user with the handle @Chongshengshilangbushilang.
But others were more upbeat.
"Despite a cooling overall economy, 40% of (Chinese) people say they will spend more on travel," said Steve Saxon, a partner at McKinsey & Co. "People want to spend the money they've saved during COVID on international travel."
Trip.com, China's largest travel agency, noted that the news had led to a spike in searches for destinations including Australia and Japan. Those countries, along with several other Asian nations and the United States, are among the most visited by Chinese travelers.
"The opening of group travel from China to the U.S. is a significant milestone," said Adam Burke, head of the Los Angeles Tourism and Convention Board. "It's impossible to overstate the importance of Chinese tourism to Los Angeles."
Shares in firms in the latest group of countries with large exposure to Chinese travel demand jumped on the news. Gains for South Korean casino operators were particularly striking, with Grand Korea Leisure and Paradise surging 20% and 18% respectively on Thursday.
Two sources in South Korea's travel industry told Reuters it was the first time group tours from China would be allowed on a large scale since a 2016 dispute over Seoul's deployment of a U.S. missile defence system. China has never publicly acknowledged limiting group tours to South Korea.
A growing number of healthcare companies in China are shelving their initial public offering (IPO) plans as its stock exchanges have stepped up scrutiny of the pharmaceutical industry's business practices amid an escalating anti-corruption drive.
Healthcare stocks have already slumped in China since the government in late July launched a year-long anti-graft campaign, targeting what it said was the rampant practice of bribing of doctors in drug and medical equipment sales.
Pharmaceuticals is the latest industry in the cross-hairs of Chinese regulators, and the tighter vetting of the sector's IPO candidates shows the sway regulators have over companies' fundraisings. That is even though China has revamped its IPO system to make it market-oriented, with listings no longer needing the securities watchdog's approval.
Vaccine maker Shanghai Rongsheng Biotech Co terminated its IPO plan this week, after the company's high proportion of sales expenses drew attention from regulators.
The Shanghai Stock Exchange asked Rongsheng - whose sales expenses over the past three years were equivalent to a third of revenue - if it had "undisclosed transfer of interests to customers", according to securities filings.
"Drugmakers' sales expense problems are in the limelight" due to the anti-corruption campaign, said a Shanghai-based IPO banker at a state-owned brokerage who did not wish to be identified due to the sensitivity of the topic.
"Vetting of drugmakers' IPO applications has become extremely strict recently."
Another drugmaker, Fujian Mindong Rejuenation Pharmaceutical Co, also withdrew its listing application, after the Shenzhen Stock Exchange sought details and the rationale of its sales promotion activities including academic seminars. The company's sales expenses over the past three years amounted to nearly half of its revenue.
Newly released NIH documents show conclusively that statements made during congressional hearings to U.S. Sen. Rand Paul (R-KY) and Rep. John Moolenaar (R-MI) by NIH leaders Anthony Fauci and Lawrence Tabak were misleading, if not outright false, regarding third-party royalties paid before, during, and after the pandemic.
Tabak, acting director of the National Institutes of Health, and Fauci, then-director of the National Institutes of Allergies and Infectious Diseases, both claimed before Congress that they could not release the names of the companies paying NIH third party royalties.
Last week, however, our OpenTheBooks lawsuit based on our Freedom of Information Act request caused NIH to release new documents.
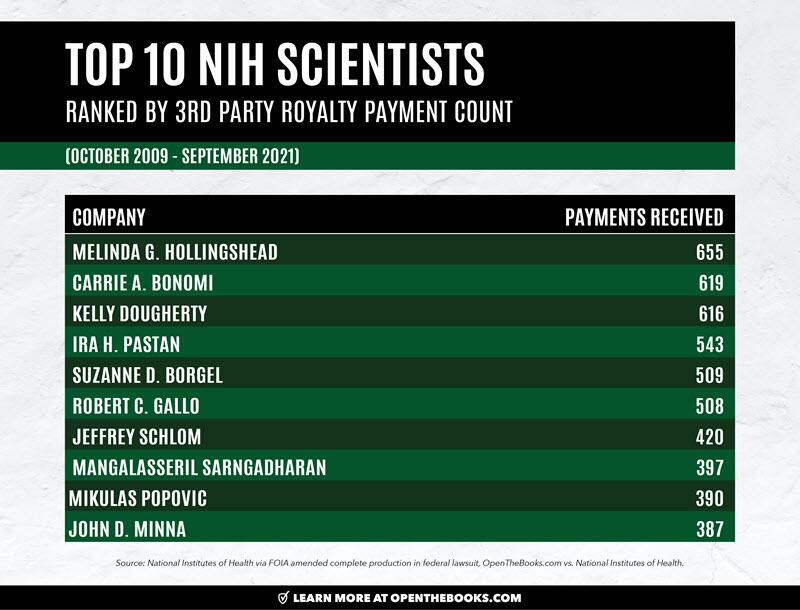
The newly released documents reveal – for the first time – the names of companies that paid NIH scientists $325 million in third party royalties from 56,000 transactions between September 2009 and October 2020.
Our OpenTheBooks oversight reporting — which led to three congressional hearings during 2022 regarding NIH’s secret third party royalty payments — is available here for review.
Here are some key findings from the new disclosures:
In U.S. Senate hearings during 2022, Dr. Anthony Fauci refused to disclose the companies who licensed his “inventions” and paid his third-party royalties. Finally, now, we know the companies paying him. They are listed below.
Chinese government-owned pharmaceutical companies, controlled by the Chinese Communist Party (CCP), paid the National Institutes of Health (NIH) third-party royalties to license technologies developed on the U.S. taxpayer dime. One such company neighbors the Wuhan Institute of Virology, collaborates with the lab, and even paid a royalty to Douglas Lowy, a multiple term acting director at the National Cancer Institute, a sub-institute of NIH.
Russian animal vaccine maker – which was allegedly a front for a Soviet bio-weapons lab – licensed inventions and paid royalties to NIH for tech developed with taxpayer dollars.
Purdue Pharma – the makers of the highly addictive and frequently abused OxyContin (oxycodone) – licensed tech developed with public funds and paid royalties to NIH – even after the company pleaded guilty to federal crimes relating to opioids.
Long-serving former NIH director, Francis Collins, received third party royalties on his inventions from four companies that themselves received nearly $50 million in federal contracts and grants since 2008.
During the pandemic, the American people started to worry that Big Government was too close to Big Pharma. Now, because of our oversight investigation at OpenTheBooks.com, we know just how close they are: NIH spends billions on the industry and now we know the industry sends millions back to NIH and its scientists.
Last year, the National Institutes of Health – Fauci’s former employer – doled out more than $30 billion in government grants to roughly 56,000 recipients. That taxpayer largess buys plenty of friends and enormous influence across the entire U.S. healthcare complex – the scientific, research, drug, therapeutic, and healthcare industries.
These payments from third-party payers enriched the agency, its leadership, and 2,400 individual NIH scientists. It took our Freedom of Information Act request – ignored by NIH in September 2021 – and our federal lawsuit filed in November 2021 to finally force production of these payment records. The public interest law firm, Judicial Watch, represents us.
Supported by Tabak and Fauci’s false testimony to Congress, NIH initially redacted the name of the payor (company), the amount paid to the individual scientist (think Fauci) and what was invented by the taxpayer-paid scientist in the government lab (license/patent number) from their initial 3,000 pages of court-ordered production during 2022.
Their production defied the court and the public’s right to know. For a gaggle of doctors, they were treating the sunlight of transparency like an unknown pathogen.
Significant Transparency Victory Achieved
Until last week. That’s when NIH provided new production disclosing a partial two of the three formerly redacted items on all royalties paid since 2009: 1. The name of the third-party payor; and 2. The license number on the NIH invention.
NIH still refuses to disclose the dollar amount paid to the individual scientist and will not disclose patent numbers either. We will exhaustively litigate what we consider to be NIH’s smoking cover-up gun of defiance toward informing the taxpayers whose agency it is.
Background: What is a third-party royalty? When a government scientist invents something, it can be licensed to the private sector for enhancement, distribution, and profit-making. Under the law, the private entity pays royalties back to NIH – enriching the agency, its leaders, and its scientists.
Watch the U.S. Senate hearing where Fauci obfuscated and defended secrecy at the expense of our right to know while being questioned by Sen. Rand Paul (R-KY):
Fauci, Collins, Et Al – Who Paid Them?
We now know “Who” paid royalties to agency leadership, top scientists at NIH, and everyone else.
Well-known scientists receiving payments during the period included:
Francis Collins, the director of NIH from 2009-2021 who then served as President Biden’s Covid czar in 2022 (Public salary: $300,000). Collins received 21 royalty payments between 2010 and 2021.
Specialty Laboratories, Inc. (4 royalty payments) – provides biological testing services and was acquired by Quest Diagnostics in 2007. The company received $40.1 million on 403 contract payments from many U.S. agencies since 2008.
ISIS Pharmaceuticals, Inc./Ionis Pharmaceuticals (4 royalty payments) – specializes in RNA-targeted therapeutics. Ionis changed its name from ISIS in 2015. The company received $2.2 million in federal contracts (including DARPA) since 2008.
GeneDx, Inc. (12 royalty payments) – founded in 2000 by two NIH alumni involved in genetic research. The company received $5 million on 155 contract-payments, mostly from NIH, since 2008.
Progeria Research Foundation (1 royalty payment) – a nonprofit dedicated to finding treatments and a cure for the congenital disorder. The organization received $407,887 in federal grants since 2008.
Anthony Fauci, the immediately retired director of the National Institute of Allergy and Infectious Diseases (NIAID) and highest paid federal bureaucrat since 2019, received 37 royalty payments (2010-2021). (Fauci’s 2022 taxpayer-funded salary: $480,654.)
Here are the companies that paid Fauci, according to NIH disclosures:
Ancell Corporation (14 royalty payments) – produces immunology tolls intended for scientific research and payments spanned the years 2012 through 2016. License: +L-257-95/0
Santa Cruz Biotechnology (15 royalty payments) – creates products for medical research, including antibodies and payments spanned a decade, years 2011 through 2021. Licenses: +L-012-07/0, +L-012-07/1, +L-012-07/2 (Overall—when ranked by number of royalties paid since 2009, Santa Cruz was #5 out of 2019 companies in the database.)
Chiron Corporation (8 royalty payments) – focused on biopharmaceuticals, vaccines, and blood testing. Fauci’s royalties continued through March 2014 on License: +L-167-95/1.
Sen Rand Paul: “Can you tell me that you have not received a royalty from any entity that you ever oversaw the distribution of money in research grants?”
Fauci answered: “You know, I don't know as a fact, but I doubt it.”
In 2004, Fauci’s NIAID contracted with Chiron to develop a vaccine for avian influenza (bird flu). Fauci said, “information generated under this task order will be important for preparing our nation and the world against new influenza viruses with pandemic potential.”
In 2005, then-reporter John Solomon at the Associated Press successfully used FOIA to crack open the full NIH royalty database – including payments to individual scientists. Anthony Fauci was among the 51 scientists found doing experiments involving inventions for which they were being paid royalties.
Between 1997 and 2004, Fauci received $45,072.82 in royalties from Chiron Corp. for a patent license on an experimental AIDS treatment (interleukin-2). Then, NIAID funded it with at least $36 million for testing on patients at 200 sites across 18 countries during five years.
When challenged about collecting the payments and later making decisions about related research funding, Fauci said he’d donate his royalties to charity — but never provided proof.
In 2005, Novartis acquired Chiron Corp. Novartis is the #10 ranked company on the count of royalty payments (324) at NIH since 2009.
Since 2008, Novartis received $2.3 billion in contract payments from multiple federal agencies including $17 million in contracts and $15 million in grants from NIH. Much of that funding was during a period when Fauci was receiving “Chiron” royalty payments.
Douglas Lowy has been the Acting Director of the National Cancer Institute for three periods since 2015 and the deputy director of the of that institute since 2010. He has directed a research laboratory at NCI since 1975 and also held the title of chief of the Laboratory of Cellular Oncology within the agency’s Center for Cancer Research.
Lowy is one of the top royalty receivers at NIH with 192 payments since 2009 from 32 companies. Here is a sample:
Wuhan Institute of Biological Products Co Ltd (one royalty payment) – a subsidiary of the state-owned pharmaceutical company Sinopharm. In 2016, the company moved next to the Wuhan Institute of Virology, and collaborates with that lab. (In total, this institute made 64 royalty payments to NIH scientists during the period 2009-2019.)
Merck (33 royalty payments) and GlaxoSmithKline (13 royalty payments) – the companies then marketed vaccines that used Lowy’s inventions as Gardasil, Gardasil 9, and Cervarix, respectively.
Gardasil and Gardasil 9 generated $1.5 billion in sales for Merck alone in 2021. (NIH redacts the amount of the payment, so we do not know how much money Lowy made from these payments. However, NIH rules limit staff from receiving more than $150,000 a year in royalties. Any payments in excess go back to the agency itself.)
Foreign Firms Paying Royalties Include Those Located In Russia, Belarus and China
Every segment of drug development and distribution globally is represented in the database including foreign companies linked to adversarial states. Drug development and pharma sales and distribution have human risks and these data points need transparency.
A quick survey of the data revealed at least 31 countries represented including China, Russia, Belarus, Cayman Islands and Hong Kong, in addition to United Kingdom, Switzerland, Japan, Germany, France, Canada, India, Ireland, Singapore, Israel and many others.
In Belarus, we found BelVituniPharm (4 payments) paid NIH royalties to license technologies paid-for by U.S. taxpayers. This is an unstable veterinary company in a country with a reputation of rabid corruption. Belarus is a puppet satellite of Russia taking hostile actions against NATO allies where journalists are imprisoned.
In China, there are at least 28 major Chinese companies licensing NIH technologies including:
Wuhan Institute of Biological Products Co Ltd (64 payments) – This company is a subsidiary of the state-owned pharmaceutical company Sinopharm. In 2016, the company moved next to the Wuhan Institute of Virology to collaborate with them.
WalVax BioTech (35 payments) – The company is engaged in research and development, manufacturing and distribution of, they claim, “safe and efficacious quality vaccines” in China with major investments from the Bill and Melinda Gates Foundation.
Guangzhou HeAn Biological (24 payments) – In 2017, the company made the FDA’s “top grossing license agreements” on their list of “technology transfer success stories.”
Other Chinese companies licensing NIH technologies developed with taxpayer funds and paying royalties identified ( by no means exhaustive) include:
Wuhan Inst of Biological Products; WuXiAppTec, Inc.; Chengdu; Changchun Hongda Bio. Pharm. Co., Ltd.; Ping An Technology (Shenzen) Company LTD; Sinotau Pharmaceutical Group; Beijing Kinghawk Pharma; Beijing Zhongyuan Ltd; Sinovac; Beijing Luzhu Biopharm Co., Ltd.; Shanghai ChemPartner Co., Ltd.; Beijing Cell-fusion Biotechnology Co.; Shandong Yidu Biotechnology Co., Ltd.; Xinkexian (Beijing) Biological; Pharmaron Beijing Co., LTD; International Medica Foundation; Dalian Hissen Bio-Pharm; Shanghai Institute of Biological PR; Anhuilongcom Biologic Pharmacy Co LTD; HJB (Hangzhou) Co., Ltd.; China Novartis; Chengdu Boaovax Company; and Ningbo Rongan Biological.
But Tabak assured lawmakers that “firewalls” were in place to prevent undue influence of licensees over grant-making, research, and regulatory decisions. He never provided concrete examples of these firewalls and his office did not respond when we asked for comment.
The NIH position on the transparency of third party royalties seems to be just give us the funding. We’ll do the rest!
These unelected bureaucrats have forgotten that they work on behalf of us, the American people. And we get to hold them accountable for tax-and-spend decisions.
Pfizer and Moderna Royalty Payments
In the NIH disclosures, Pfizer is listed under multiple companies including Pfizer, Inc.; Pfizer Animal Health; Pfizer Global Research and Development; and Pfizer Limited (UK). The multiple Pfizer entities made 265 payments to 83 NIH scientists since 2009.
Because the amount of the payment isn’t listed, we don’t have an answer as to how much Pfizer paid in royalties.
Covid-vaccine maker Moderna paid 207 royalties to 43 NIH scientists since 2009 through May 2021. According to court disclosures and news reports, Moderna settled litigation with NIH for $400 million in Covid-vaccine royalties during 2022.
Again, more information isn’t forthcoming because NIH is waging a war on transparency.
With every or nearly every S&P member in healthcare products paying third party royalties to NIH and their scientists, the database is ripe for all kinds of ethical questions. For example, agency capture – has the industry captured the NIH?
Is there a steady stream of scientists moving from the agency to the private sector who succeed at attracting funding from their former colleagues?
Is NIH engaging in sweetheart license agreements with favored players?
Furthermore, the industry isn’t distinguished by historically high morals. Most drug companies have been sanctioned for corrupt practices around drug trials.
Purdue Pharma paid 15 royalty payments to NIH for technologies developed on the taxpayer dime between the years 2010 and 2013 – during a period when NIH admits it was trying to “partner” with company. This was despite the fact that Purdue had already pleaded guilty in 2007 to federal crimes for deceptive marketing that downplayed the risk of becoming addicted to opiate painkillers such as their segment leading branded product OxyContin – which grew into the national opioid crisis.
Our Battle Continues
The American people need to be able to follow the money. After 18 months in federal court alongside our lawyers, Judicial Watch, NIH still refuses to disclose the amount of money paid to each individual scientist. We also need to know the patent number – what the invention was – and that should be basic information.
This Fall, we are back in federal court to demand complete transparency. The American people deserve no less.
Note: Since the 1980 Bayh-Dole Act, federal scientists have legally been able to receive royalty payments for inventions in government facilities. These payments are legal and no scientist is accused of wrongdoing.
U.S. House Appropriations Hearing | Lawrence Tabak, Acting Director, National Institutes of Health questioned by Rep. John Moolenaar (R-MI) on third party royalties and appearance of conflict-of-interest | C-SPAN | May 11, 2022
U.S. Senate Hearing | Anthony Fauci, Director of National Institute of Allergies and Infectious Diseases questioned by Sen. Rand Paul (R-KY) on third party royalties | C-SPAN | June 16, 2022
U.S. Senate Hearing | Anthony Fauci, Director of National Institute of Allergies and Infectious Diseases questioned by Sen. Rand Paul (R-KY) on third party royalties | C-SPAN | September 14, 2022
Hospitals nationwide charge payers more than double for healthcare services covered under commercial plans than they do for the same insurer’s Medicare Advantage (MA) plans, according to a recent Johns Hopkins analysis of hospitals’ published pricing data.
The work, published this week in Health Affairs, reviewed more than 200,000 unique combinations of hospitals, insurers, settings and services for which a commercial and an MA price were available for direct comparison. In total, it included pricing data from 2,434 hospitals and 118 insurers collected in September 2022.
Commercial prices were, on average, between $600 and $707 more expensive than MA prices, or 2.1 to 2.2 times more expensive.
The dollar gap for prices was widest within the surgery and medicine service category where median commercial prices were nearly $800 more expensive than the charges for MA plans ($1,702 versus $928), 1.8 times higher. The median price increases were consistent across the other three reviewed service categories: imaging ($490 versus $191, 2.6 times higher), lab tests ($32 versus $12, 2.7 times higher) and ED visits ($519 versus $262, 2.0 times higher).
The researchers found that commercial prices often remained twice as high or greater even when looking at the same hospital, insurer and services, though there was “substantial variation” in the commercial-to-MA price ratio across the data set.
While a small portion (3.7% and 6.6%, depending on service category) of the prices were equivalent between plan types, some hospitals’ commercial prices were also five times or more than the MA prices for the same service (6.5% to 27.2%). Researchers also found differences in the median ratio from state to state, with commercial prices highest in Delaware (5.1 times higher) and South Carolina (4.2) and broadly higher ratios in the country's most populous states such as California (2.8), Texas (2.5) and Florida (2.7).
“The substantial gap in prices between commercial and MA, when negotiated by the same insurers and hospitals, [reveals] the pricing consequences of differing incentives and regulations across markets,” Mark Meiselbach, Ph.D., assistant professor in the Department of Health Policy and Management at Johns Hopkins University and the study’s lead author, told Fierce Healthcare. “These differences include out-of-network price benchmarks, competition from traditional Medicare, and that insurers bear more risk in the MA market than in the commercial market.”
Subsequent analyses linked the higher median price difference ratios with hospitals affiliated with a health system, nonprofit hospitals and teaching hospitals, according to the study. Greater hospital market concentration and a higher number of hospital beds were also tied to “modestly” higher price ratios.
Meanwhile, large national insurers were also associated with greater ratios, while greater insurance market concentration was linked to “modestly” reduced ratios, they wrote.
“All of the major insurers generally had median price ratios above 2.0 for most or all service categories, with the exception of Centene. Kaiser Permanente generally had the highest median ratios, which were as high as 3.7 and 4.1 for imaging and laboratory tests, respectively,” the researchers wrote, noting that the integrated system’s high ratio was “unsurprising, given that our sample contained non-Kaiser hospitals.”
The researchers noted in the study that insurers bear more risk for their MA plans than they do commercial plans, as much of the cost for the latter is self-funded by employers. Though insurers should still be incentivized to negotiate lower commercial prices as they compete for employers’ business, “insurers may accept higher prices for their commercial plans if it allows them to remain competitive in the MA market, where gross margins are nearly twice as high per enrollee,” they wrote.
Further exploring that incentive—alongside other pricing pressures such as competition with traditional Medicare and government requirements that out-of-network MA prices fall in line with traditional Medicare prices—could represent a path for policymakers interested in reducing commercial charges that are, ultimately, passed along to employers and their employees, researchers wrote.
“Though employers should be concerned with the much higher prices they pay, these findings suggest that changes in regulation and incentives could meaningfully impact prices,” Meiselbach said.
The researchers' study is the latest in a string of healthcare cost analyses enabled by recent federal requirements that hospitals, and later payers, share their prices for common services with the public. Others have found substantial differences in the commercial prices for brain MRI depending on a hospital’s characteristics or outlined frequent pricing discounts when patients pay with cash.
Most Medicare Advantage (MA) beneficiaries are satisfied with their health plan, but many enrollees feel they are overbilled, have struggled navigating the prior authorization process or are confused by the features of their plan, anew surveyfrom Retirement Living recently revealed.
The survey found that 71% of beneficiaries are satisfied with their MA plan, with most people choosing a MA plan due to the plan's affordable costs and out-of-pocket expenses. Other factors that contributed to the decision included coverage of prescription drugs, access to providers and the ability to choose a doctor, comprehensive coverage options and medical and preventive care options.
In addition, 61% of people said their MA plan outperforms their previous coverage plan.
However, only 44% of MA enrollees say they fully understand their plan, with 68% saying certain details have caused confusion. Dental coverage was the most reported area of confusion, followed by out-of-pocket costs, transportation to medical appointments, caregiver support services, home health services and vision and hearing coverage. At least 20% of beneficiaries said they didn’t understand one or more of these plan elements.
Other respondents believed a lack of familiarity with the plan (56%) caused confusion, while some (44%) believed there was inadequate communication and education about benefits offered. More than 1 in 4 beneficiaries reported paying out-of-pocket costs for services they believed were covered by their plan, while 1 in 10 said they thought were overbilled for their MA plan.
Some MA enrollees felt unsatisfied by various elements of their plan, including telehealth services, online and mobile app management and chronic disease management programs, while almost 20% of respondents said they experienced delays in care caused by the prior authorization process.
Of the nearly 1 in 10 enrollees who thought they might switch coverage plans in the next year, 50% cited cost and 39% wanted to switch provider networks.
Recent studies have highlighted the positive impacts of MA plans for enrollees, including a report from the Elevance Health Public Policy Institute that found 83% of dual-eligible and 75% of non-dual-eligible individuals used at least one supplemental benefit a year. The analysis concluded that MA enrollees find value in plans when they need to meet personalized needs.
MA plans are also more popular with individuals from marginalized backgrounds. Analysis from ATI Advisory showed that a higher percentage of Black, Latino and Asian enrollees choose MA than fee-for-service plans. The report showed that MA beneficiaries also tend to live in more socially vulnerable counties.
Retirement Living surveyed 351 beneficiaries, asking them about premiums, customer service and provider networks. The median age of respondents was 69 years old.
Health plans are set to receive $12.8 billion in Medicare Advantage (MA) quality bonus payments this year, with UnitedHealthcare topping the list at $3.9 billion in bonuses.
UHC and Humana, which together account for the largest share of MA enrollment, will receive 49% of 2023 bonus payments, according to an analysis from KFF. Humana will earn $2.3 billion in bonuses.
However, Kaiser Permanente has the largest number of plans earning bonuses at 99%, according to the report. The healthcare giant will earn $966.8 million in total for an average of $523 per annual enrollee.
Kaiser Permanente enrolls 6% of MA members, according to the analysis.
Centene plans earned the lowest average payout at $251 per enrollee, and 55% of its MA members were enrolled in plans that earned bonuses. The company received $321.6 million in total bonuses.
Cigna was the lowest earner in total tracked by the report, bringing in $247.3 million, but it was also the smallest player at 2% of MA enrollment. It earned $432 per enrollee on average, and 80% of its MA members were enrolled in a plan that earned a bonus.
The KFF analysts noted that bonus payments in the program have increased each year since 2015. This does follow significant growth in MA enrollment, but payments have increased more quickly, they said.
Payments have more than quadrupled in that window, growing from $3 billion in bonuses in 2015. Bonus payouts were up by nearly 30% from 2022 alone, the KFF researchers found.
The number of people enrolled in plans with at least four stars is a key factor in the increasing payouts, according to the report.
"This spending comes at a time when the Medicare program is facing growing fiscal pressures, which are exacerbated by growth in quality bonus program spending," the researchers wrote. "Growth in the quality bonus program is projected to lead to faster growth in Medicare Advantage benchmarks (and corresponding spending) compared to traditional Medicare spending in upcoming years."
Overall, 85% of people enrolled in MA are in a plan that will earn a bonus, according to the report. By comparison, that's up from 75% in 2022 and 80% in 2021.
Bonuses were highest in group employer or union-sponsored MA plans, averaging $460 per enrollee. Payouts were $417 on average for individual plans and $374 in special needs plans.
The analysts said tracking bonus payment trends will be a continued focus as MA enrollment swells.
"Understanding the effects of the quality rating system and associated bonus payments, including the implications for Medicare spending and beneficiary premiums, will be increasingly important as Medicare Advantage enrollment continues to climb," they wrote.