One of my favorite books this year was Michael Lewis’s The Premonition: A Pandemic Story, a page-turner in which he traced the problematic issues of the CDC long before and intra-Covid-19 and gave it a different acronym: CDOR, the Center for Disease Observation and Reports. I did an in-depth interview with him about what he learned.
In the first year of the pandemic, the CDC was subverted by the Trump Administration even to the point of interference and censorship of its MMWR reports, stripping its control of data, and frank undermining of public health. That’s why we warmly embraced the new Administration’s proclamation that it would stick to the science. There were clearly issues with that regarding the lack of need for masks among vaccinated people, unwillingness to recognize SARS-CoV-2 airborne transmission, and mass confusion over boosters. But in the last 24 hours things have gotten much worse.
Yesterday, the CDC issued a shortened isolation period guideline of 5 days instead of 10 days for people with Covid infections. That came less than a week after they issued the guideline of 7 days for health care workers.
There were serious problems about the new 5-day isolation period. First, there are no data or evidence to back it up. Yes, we’re facing an Omicron onslaught of cases and it would be useful to come up with a strategy to avoid a mass loss of functionality among our workforce and the on-the-go public, no less in the midst of the holiday season. But that doesn’t justify issuing a vacuous guideline. Second, there was no mention of using a test, to confirm that the isolated individual is now OK to circulate, that there is no indication of infectiousness. That could be done via a rapid antigen test, which denotes infectiousness, carries some reduced sensitivity with Omicron, or via a PCR. The cycle threshold value of a PCR test is also indicative of infectiousness; the lower it is, the more likely potential for spread. Either of these tests would be far better than no test to justify a reduced isolation time in any individual.
Third, there are no data for Omicron’s clearance time. We know the characteristics of shedding and average time it takes for clearance of the virus for Delta and preceding variants, but to date we have not seen any such data for Omicron kinetics. With the Hong Kong report of 70-fold copies of the virus in the upper airway for Omicron versus Delta and prior variants, there is no certainty yet that Omicron’s clearance is fast.
Fourth, the guidance did not mention a word about vaccinated or unvaccinated status of people. We know from past studies there is a more rapid clearance among vaccinees than people who were not vaccinated, but the recommendation does not take this knowledge into account. Fifth, it assumes that all people handle the virus similarly when, it fact, there is considerable variability. Look at the data last week published at NEJM
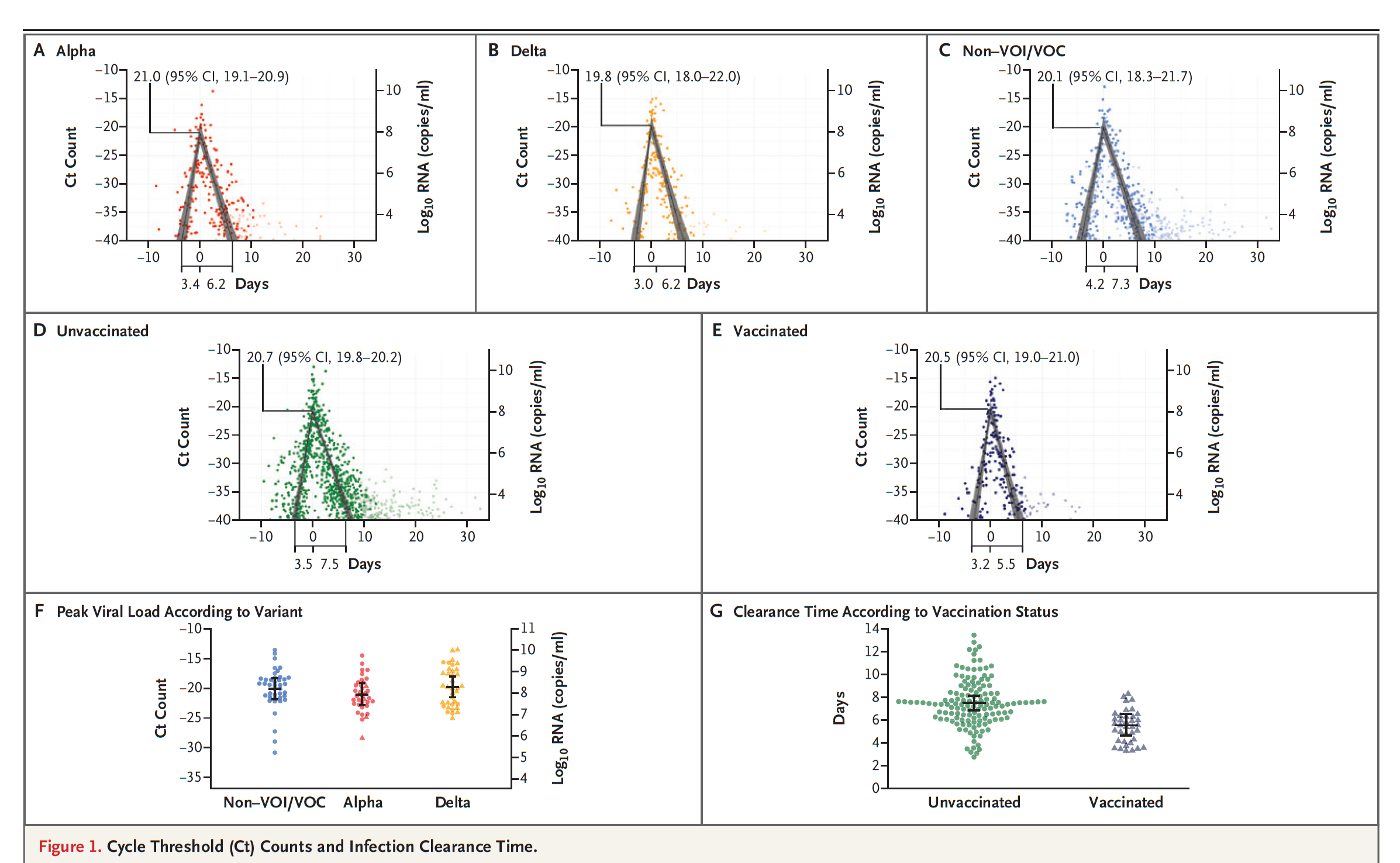
Note from the Figure that there are significant differences for vaccinated, average 5.5 days (95% CI 4.6, 6.5), compared with unvaccinated, average 7.5 days (95% CI 6.8,8,2) There is marked inter-individual variability: for example, look at all the green dots even >20 days in the unvaccinated group, panel D. These data, representing nearly 20,000 samples, were obtained from predominantly healthy young men and may not be representative of the population at large. By the way, the NBA uses a 6-day isolation cutoff with testing with heavy emphasis on testing.
This problem can be fixed. The CDC could come out and revise their guidance and say there are no such data for Omicron (as a cover, like they did when they finally recommend boosters for all adults) and require testing. Even the airlines, which pushed for a shortened 5-day isolation period, wanted to use testing as part of that requested change in policy.
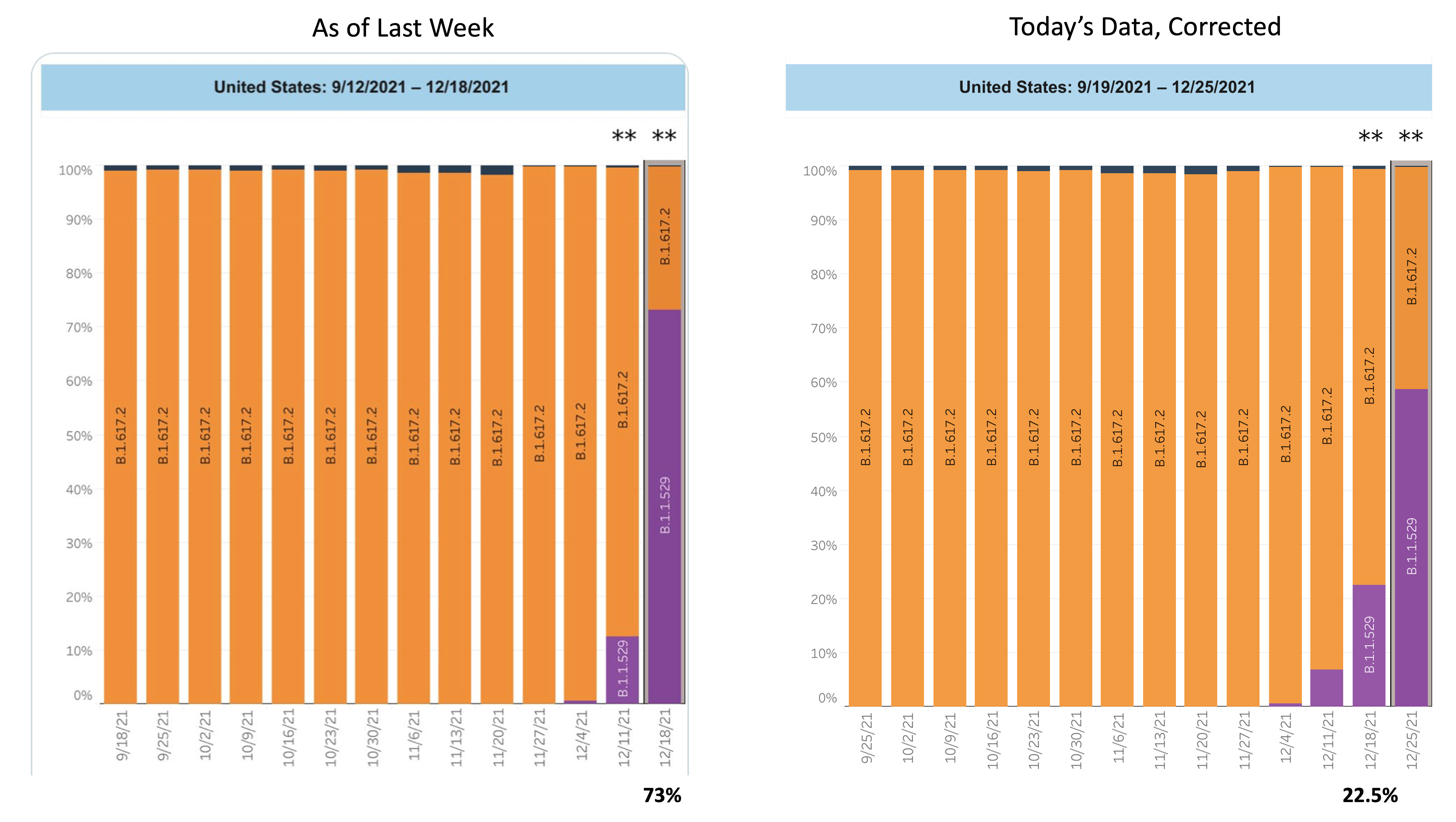
But the bad day wasn’t just about isolation in isolation. There was also the major gaffe about genomic sequencing surveillance. Here are the data from last week, and the corrected data this week, announced today by CDC. The point estimate for Omicron changed for the week ending December 18th from 73% to 22.5%, which is remarkable. We were led to believe that the country was well in the midst of the Omicron wave when, in fact, we were and are still experiencing a large number of Delta infections. As of December 25th, the point estimate is 59% with 95% confidence intervals lower 42%, upper 74%, indicating there is a lot of wobble, a relatively limited number of sequencing samples to draw upon, no less a reduction in confidence for the CDC itself.
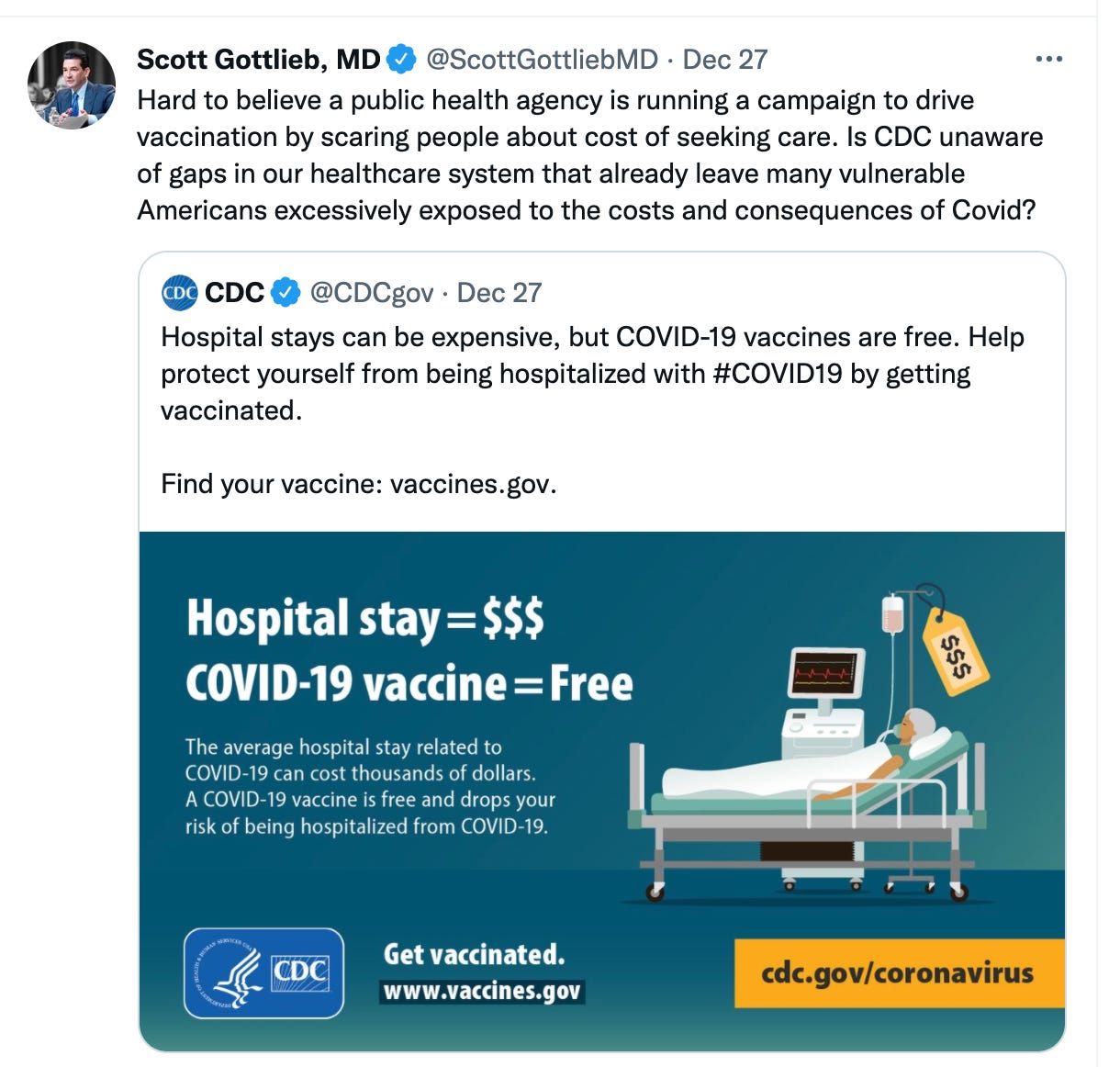
But it continues. Yesterday, as noted by Scott Gottlieb on twitter a critique of a poor new ad for CDC to encourage vaccination to save hospital costs. He makes the point in his post that I don’t need to repeat here.
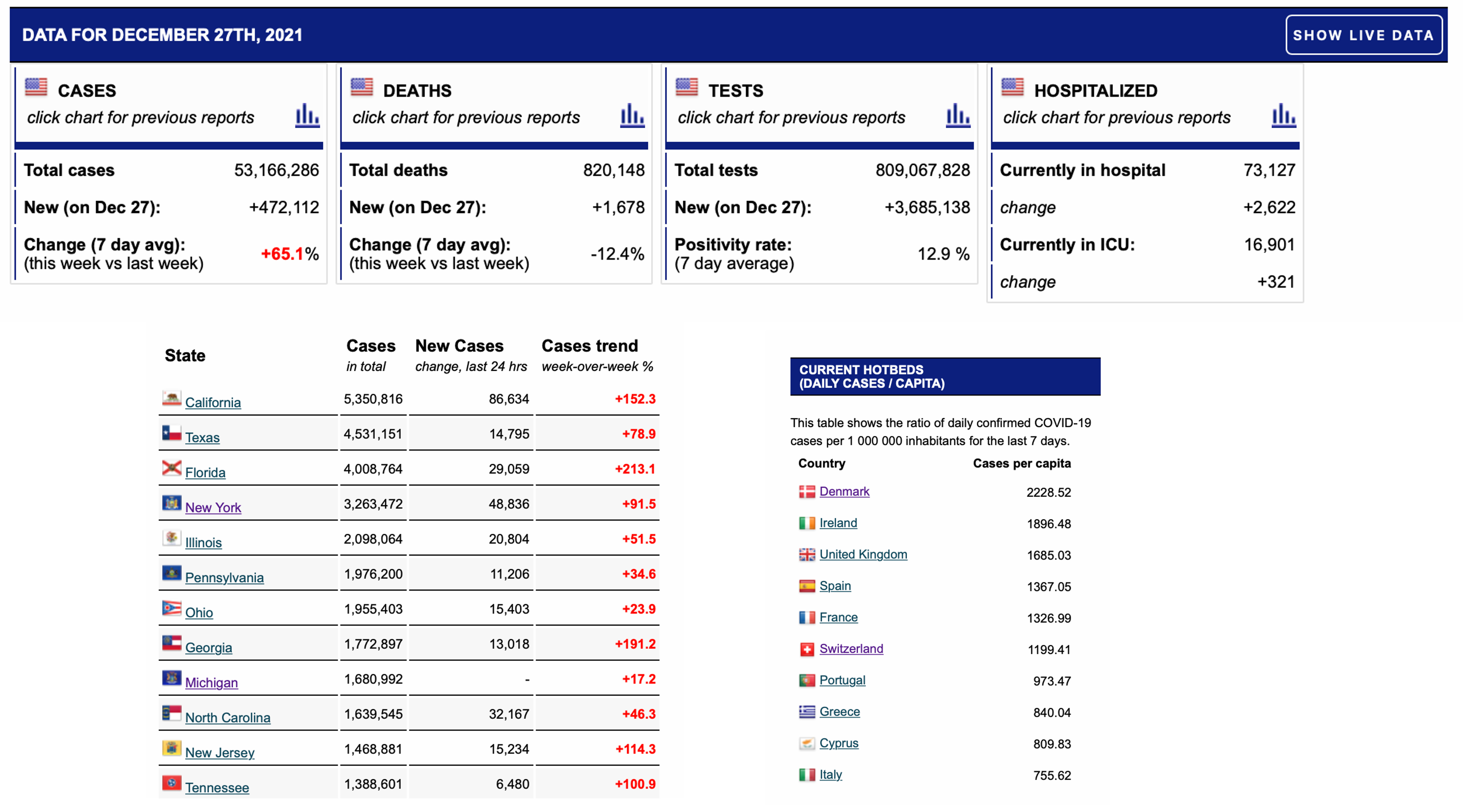
The profound data deficiency and lack of any semblance of informativeness by CDC is a topic I covered in a recent Substack post. But yesterday I found out that it takes only 3 people https://newsnodes.com/us, led by Gérard Hoeberigs, to post data promptly every day for each US state — including new cases, tests, % positive tests, hospitalizations, ICUs & deaths—and much of this for the rest of the world. But CDC has an annual budget that exceeds $7.9 billion and cannot do this. Here’s a little of what newsnodes.com posts each and every day, and you can go much deeper into states and countries around the world.
Remember the Covid-19 Tracking Project posted such data for the United States each day because the CDC was incapable, but stopped doing so in March 2021 because it was given reassurance that CDC would step up. They have never done so, particularly when it comes to divvying up hospitalizations by vaccination status (including type, timing, number of doses), variant, and patient characteristics (such as age, co-existing conditions, immunocompromised). Close tracking of breakthrough hospitalizations and deaths was promised by CDC in May 2021, but they haven’t made good on that. Instead, they have served up once a month snapshots with minimal data, such as this most recent posting, for a limited number of US jurisdictions. As previously reviewed, HHS Secretary Becerra could mandate collection of these data for all US states, but has chosen not to.
It’s now crunch time when we need to know about Omicron and whether it will prove to be less severe, and how much less severe, than Delta. We have a much lower vaccination rate and booster rate than UK, Denmark, Norway and other countries that faced Omicron dominance before us. Their experience to date of the uncoupling of cases and severe disease may not play out to the same extent in the United States, just as Delta did not. This requires having the data—virus sequencing and clinical data—-in real time or as close to real time as possible. You’d think you could get that for billions of dollars, with much more allocated this year to CDC to do far better with informatics.
To sum up, the CDC performance is disappointing and unacceptable, despite high hopes and a boosted budget to perform well. This was a very bad day. We can ill afford any more of these. The pandemic has a ways to go into 2022. We need this federal agency to “stick to the science” as promised, provide critically important data in a timely way, and avoid publishing alarming and erroneous data based on limited sampling. Let’s hope for a turnaround as fast as one we hope to see with Omicron. Never give up, especially the hard working staff and leadership at CDC, that we must rely upon for good guidance.
Eric Topol
physician-scientist, author, editor
https://erictopol.substack.com/p/the-very-bad-day-at-the-cdc
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.