This transcript has been edited for clarity.
Christopher J. Chiu, MD: Welcome back to The Cribsiders. This is our Medscape video recap of one of our recent podcast episodes. Justin, what are we reviewing today?
Justin L. Berk, MD, MPH, MBA: We had a fantastic conversation, Period Problems: Heavy Menstrual Bleeding, with our guest, Dr Angela Weyand, who is a pediatric hematologist with a focus on what she calls "shematology." Dr Weyand is an assistant professor and associate fellowship director of pediatric hematology at the University of Michigan, where she helps run a clinic devoted to caring for young women and girls with bleeding and clotting disorders. She was the perfect guest for this podcast, and she taught us about the diagnostic workup for heavy menstrual bleeding, treatment options, and why labs drawn in primary care might not be doing justice for the workup of bleeding disorders.
Chiu: How many adolescents presenting with heavy menstrual bleeding have an underlying bleeding disorder?
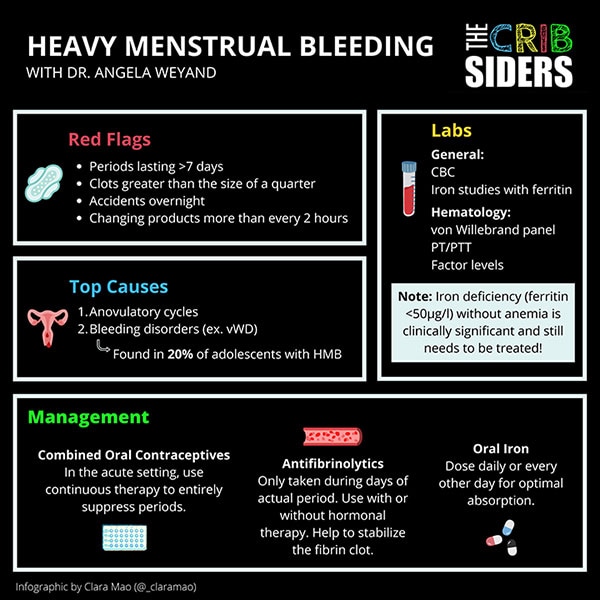
Berk: This was a great pearl from the episode that surprised me. Among average patients with heavy bleeding, about 20% will have some type of underlying bleeding disorder — about 1 in 5. The majority of those bleeding disorders are von Willebrand disease. The workup is a little complicated. Dr Weyand recommends not drawing von Willebrand labs in the primary care, emergency, or inpatient settings because those levels can be falsely elevated in acute illness. It requires some nuance in test interpretation, so she recommends having your friendly hematologist help you out with it.
Chiu: We are looking for anemia; is that correct? But is iron deficiency without anemia significant?
Berk: This was another great pearl. The primary care provider seeing an adolescent with heavy menstrual bleeding typically checks for iron-deficiency anemia, and most are pretty comfortable diagnosing and treating it. But Dr Weyand also pointed out the importance and clinical significance of iron deficiency without anemia. A low ferritin level (< 30 µg/L or < 50 µg/L) can cause significant problems even if the hemoglobin level is stable. These effects include symptomatic fatigue and cognitive dysfunction. Among teen girls, this can lead to significant morbidity. Studies show that iron repletion can actually improve academic performance and can overcome cognitive dysfunction and fatigue. So iron supplementation is recommended for iron deficiency even without anemia.
Chiu: During the podcast, you proposed a different dosing regimen for iron supplementation. We used to prescribe iron to be taken daily or even three times a day. That's no longer recommended, right?
Berk: That's exactly right. I call it "Ferrous Sulfate's Days Off" as a throwback to the Matthew Broderick film. Ferrous sulfate does not need to be dosed on a daily basis, and definitely not three times a day. Some clinical work shows that every other day works just fine because of how the body responds to an iron load with the release of hepcidin. Taking the supplement every other day provides the same degree of bioavailability of iron, but without some of the side effects such as constipation.
Chiu: Some patients have difficulty with "every other day," so I'll suggest taking it on Monday, Wednesday, and Friday. Is that what you do in your practice?
Berk: I do both. I let the patient decide.
Chiu: What are the other treatment options for heavy menstrual bleeding?
Berk: Treating iron deficiency and iron-deficiency anemia is very important to help with symptoms, but they don't address the underlying cause. Treatments for heavy menstrual bleeding include oral contraceptives, long-acting contraceptives, and the levonorgestrel IUD.
We also talked about antifibrinolytic therapy. Tranexamic acid and aminocaproic acid are taken only during the patient's heavy period. Antifibrinolytics greatly reduce the amount of menstrual flow without controlling the patient's period in the way hormonal contraceptives would. It's a great tool to have in the toolbox.
Chiu: It sounds like we have a lot of great pearls. How about a wrap-up of what we learned?
Berk: A key point that I took away was the fact that about 20% of young adolescent women with heavy menstrual bleeding may have a bleeding disorder, the most common of which is von Willebrand disease. Von Willebrand disease should be worked up in collaboration with a hematologist because the labs are pretty nuanced and can be difficult to interpret. Iron deficiency is a very clinically relevant consequence of having menstrual bleeding, even if the patient isn't anemic. Treatment can include every-other-day dosing of iron in addition to treating the underlying problem using contraceptives, but an antifibrinolytic is also an option for people with heavy menstrual bleeding.
Chiu: Excellent. Well, I want to thank our audience again for joining us for another Medscape video recap of The Cribsiders pediatric podcast. You can download the full episode on any podcast player or check it out at our website at www.thecribsiders.com. Thanks for tuning in.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.