Inogen resumed with a Buy
Tuesday, August 21, 2018
Wright Medical initiated at Stifel
Wright Medical initiated with a Buy at Stifel. Stifel analyst Mathew Blackman initiated Wright Medical with a Buy rating and $34 price target, citing its market share-leading positions in surgical repair of upper and lower extremities, which he identifies as two of the fastest-growing medical device industry end-markets. He sees sales growth sustainably accelerating back to low-double digits, Blackman tells investors.
Simple leg exercises can cut impact of sedentary lifestyle on heart, blood vessels
A sedentary lifestyle can cause an impairment of the transport of blood around the body, which increases the risk of disease in the heart and blood vessels. New research published in Experimental Physiology suggests that performing simple leg exercises whilst lying down might help to prevent these problems.
Previous work has demonstrated that prolonged sitting for up to 6 hours results in a decline in both blood flow to the limbs and in our larger arteries’ ability to widen to accommodate increased blood flow. This is the first study to demonstrate that sitting for just 10 minutes is sufficient to reduce blood flow to the legs and impairs the function of small blood vessels supplying muscles in the leg.
This paper also demonstrates a reduction in the function of small blood vessels when lying down. However, this study suggests we might be able to somewhat reverse this impairment in function by performing simple leg exercises when lying down in bed or on the sofa. These findings are important in increasing our understanding of the negative impact of sitting and physical inactivity on blood vessel function and the supply of blood to the legs.
The effects of sitting on blood circulation have been attributed to blood passing more sluggishly through arteries whilst sitting. The researchers who performed this study aimed to find out whether these reductions were caused by sustained sitting, or whether 10 minutes would be sufficient to have a negative effect.
The research group used a Doppler ultrasound technique alongside the knee to measure blood flow and examined the extent to which blood vessels widened in 18 healthy, young males. These measurements were made prior to and following a 10-minute period of sitting or during a period of rest whilst lying down, with or without leg exercises, which were performed by extending the foot back and forth every two seconds for a third of the time spent lying down. Results showed that a 10 minute period of sitting reduced participants’ ability to rapidly increase blood flow to the lower legs via small blood vessels, but did not affect the widening of larger arteries in response to increased blood flow. These findings suggest that a brief period of inactivity affects an individual’s ability to rapidly push blood to the lower limbs as efficiently as normal, but doesn’t affect the ability of large blood vessels to widen. The results also suggest leg exercises can help maintain rapid increases in the blood supply to the limbs.
The current study demonstrates changes in blood vessel function measured at the level of the knee. However, the researchers only tested healthy young males, and as such, their findings cannot be extended to females. It remains unknown as to how these responses may vary with age, or with people who have heart problems. Further research may investigate the impact of sitting and inactivity on blood vessels in other places in the body. For example, would sitting impact the function of blood vessels supplying the brain? Finally, studies designed to investigate the impact of repeated bouts of short-term sitting on blood vessel function are needed.
Co-author Dr. Paul Fadel sheds light on his team’s results: “These findings further our understanding of the negative impact of inactivity on blood vessel function and demonstrate the positive effects of simple leg exercises whilst lying down providing further insight into how inactivity affects vascular health of the lower legs”.
More information: Jennifer R. Vranish et al, Brief periods of inactivity reduce leg microvascular, but not macrovascular, function in healthy young men, Experimental Physiology (2018). DOI: 10.1113/EP086918
Certain antibiotic-resistant infections on the rise
Nearly six percent of urinary tract infections analyzed by a California emergency department were caused by drug-resistant bacteria in a one-year study period, according to new research in Annals of Emergency Medicine. The bacteria were resistant to most of the commonly used antibiotics. And, in many cases, patients had no identifiable risk for this kind of infection, the study found.
“The rise of drug-resistant infections is worrisome,” said Bradley W. Frazee, MD, attending physician, Alameda Health System Highland Hospital and lead study author. “What’s new is that in many of these resistant urinary tract infections, it may simply be impossible to identify which patients are at risk. Addressing the causes of antibiotic resistance, and developing novel drugs, is imperative. A society without working antibiotics would be like returning to preindustrial times, when a small injury or infection could easily become life-threatening.”
The authors urge some immediate changes to clinical practice such as wider use of urine culture tests and a more reliable follow-up system for patients who turn out to have a resistant bug; improving emergency physician awareness of their hospital’s antibiogram (a chart showing whether certain antibiotics work against certain bacteria); adherence to treatment guidelines and knowing which antibiotics to avoid in certain circumstances.
The Centers for Disease Control and Prevention (CDC) estimates that currently 23,000 Americans die each year from antibiotic-resistant infections.
The bacteria analyzed in this study were mostly E coli, that were resistant to cephalosporin antibiotics. Historically, such resistant bacteria were found in hospital-based infections. But, the authors note that they have been infecting more people outside of the hospital, particularly those with urinary tract infections. More than two in five (44%) of the infections analyzed were community-based (contracted outside of the hospital), the highest proportion reported in the United States to date.
The study, “Emergency Department Urinary Tract Infections Caused by Extended Spectrum Beta-Lactamase Producing Enterobacteriaceae: Many Patients Have No Identifiable Risk Factor and Discordant Empiric Therapy is Common,” involved retrospective analysis of 1,745 urinary cultures from patients with urinary tract infections at an urban Northern California Emergency Department between August 2016 and July 2017.
More information: Bradley W. Frazee et al, Emergency Department Urinary Tract Infections Caused by Extended-Spectrum β-Lactamase–Producing Enterobacteriaceae: Many Patients Have No Identifiable Risk Factor and Discordant Empiric Therapy Is Common, Annals of Emergency Medicine (2018). DOI: 10.1016/j.annemergmed.2018.05.006
Doctor Shortages Explode Thanks To ObamaCare: Who Could Have Predicted?
A year before ObamaCare became law, an IBD/TIPP Poll warned that it would lead to doctor shortages because many would quit or retire early. New evidence shows that our warnings were dead on.
A recent report from the Association of Medical Colleges projects doctor shortages of up to 121,300 within the next 12 years. That’s a 16% increase from their forecast just last year.
Not only are medical schools having trouble attracting doctors (New York University plans to offer free tuition to its med students), but current physicians are cutting back on patient visits, retiring early or switching careers.
An article in a recent issue of the Mayo Clinic Proceedings says that nearly one in five doctors plan to switch to part-time clinical hours, 27% plan to leave their current practice, and 9% plan to get an administrative job or switch careers entirely.
Another survey found that nearly two-thirds of doctors feel burned out, depressed or both.
This is already having a significant effect on patient access to doctors. A Merritt Hawkins survey of doctors in 15 metro areas found that “average new-patient physician appointment wait times have increased significantly. The average wait time for a physician appointment for the 15 large metro markets surveyed is 24.1 days, up 30% from 2014. ”
Getting a new-patient appointment with a family physician, for example, went from an average 19 days in 2014 to almost 30 days in 2017. To get an appointment for a heart checkup with a cardiologist, wait times climbed from seven days in 2009 to 21 days in 2017. For a well-woman exam with an OB/GYN, they went from 17 days to 26 over those years.
This should not come as a surprise to anyone.
Eight years ago, IBD/TIPP surveyed 1,376 practicing physicians across the country, asking them what they thought about the health reform bill Democrats had been putting together.
The survey found that a surprisingly large share of doctors, 45%, “would consider leaving their practice or taking an early retirement” if Congress passed what ended up as ObamaCare. (To read more about ObamaCare, click here.)
The survey generated plenty of attention — most of it from Democrats and the mainstream media who desperately wanted to get ObamaCare enacted. They viciously attacked the survey, calling it “shoddy,” “out of whack,” “ludicrous,” “not trustworthy,” “shabby” and “garbage.”
Turns out it was the critics of the poll who were shoddy, out of whack and not trustworthy.
Subsequent surveys proved the IBD/TIPP poll right, including one taken in 2015 by the Mayo Clinic that found 54% of doctors suffering burnout, and a 2016 survey that found just over half say they participate in ObamaCare plans.
Obama Mandates and Doctor Shortages
One of the big drivers of doctor exits, by the way, is the Obama administration’s “electronic health records” mandate, which was supposed to vastly improve the quality and efficiency of care.
It’s had the opposite effect. A Mayo Clinic survey found that the EHR mandate is reducing efficiency, increasing costs and paperwork hassles, and pushing more doctors to quit or retire early.
A Harris Poll found that 59% of doctors say the current EHR system foisted on them by the Obama administration needs “a complete overhaul,” and 40% say it imposes more challenges than benefits.
ObamaCare continued what had been a long and sorry trend in health care. Government-imposed rules designed to fix some problem in the system instead generated mountains of new administrative work.
The result has been that while the number of physicians in the country has climbed modestly over the past three decades, the number of health care administrators exploded.
(You can see the trend in this eye-opening chart compiled by the Center for Freedom and Properity.)
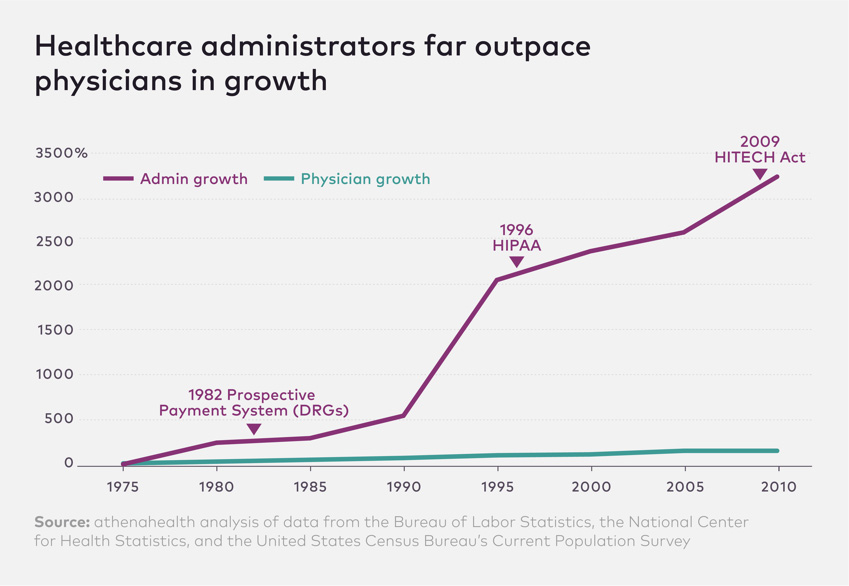{kind=link}
Driving doctors out of the medical profession and exacerbating doctor shortages was not what Obama promised when he started “reforming” health care. But it is what his heavy-handed government interventions are producing.
Don’t say we didn’t warn you.
Alphabet-backed One Medical primary care in talks to raise over $200M
Primary care group One Medical is in talks to raise more than $200 million in growth capital from the private equity firm Carlyle Group, according to people with knowledge of the talks. The firm also aims to buy an additional $100 million worth of shares from existing investors.
The company is in the late stages of conversation, the sources say, as the deal is not yet done. The company declined to comment.
One Medical is a primary care group with offices in San Francisco, New York, Seattle and other cities across the country. It accepts insurance from most carriers, and and also lets users without insurance pay out-of-pocket. The company sets itself apart with its technology. In addition to online scheduling, the company offers a virtual medical team, a suite of mobile apps and has built its own electronic medical system rather than relying on a third party vendor.
One Medical in July of 2017 named former UnitedHealth group executive Amir Rubin as its CEO to replace its founder Tom Lee. At that time, Rubin told CNBC that the company had seen “tremendous growth” in its business that sells its primary care clinics into the employer market, and not just with consumers. One Medical in recent years has positioned itself as an on-site or nearby clinic to companies with large campuses, so that employees can access concierge medical care without leaving the office.
The company has raised more than $180 million in capital since it launched in 2007 from investors such as JPMorgan, Alphabet‘s GV, Benchmark and Maverick. One Medical’s most recently reported valuation was more than $1 billion. It’s not known where the current round values the company.
Pfizer working with FDA to extend expiry dates of Epipens in short supply
Important Update on EpiPen® (epinephrine injection, USP) 0.3 mg
Auto-Injectors
Extended Expiration Dates for Select Lots of EpiPen® 0.3 mg Auto-
Injectors and Its Authorized Generic
To address shortages of EpiPen, Pfizer is coordinating with FDA to extend the expiration dates of specific lots of EpiPen® 0.3 mg Auto-Injectors and its authorized generic version after review of stability data. Patients should have confidence in using the products from these particular lots as Pfizer works to stabilize supply, which is anticipated in the fourth-quarter of 2018.
This announcement is based on a careful review of product stability data provided by Pfizer. We believe the extension of the expiration date will temporarily address patients’access to and use of EpiPen® 0.3 mg Auto-Injectors, and the authorized generic, particularly during back-to-school season as demand increases.
The affected lots, which have current expiration dates between April 2018 and December 2018, are indicated in the tables below with their new expiration dates and can be found on FDA’swebsite
The extension of the expiration datesdoes notapply to EpiPen Jr® (epinephrine injection, USP) 0.15 mg Auto-Injectors and its authorized generic version of this strength. Patients shouldcontinue to adhere to the manufacturer’s expiry datelabeled on EpiPen Jr® 0.15 mg and Epinephrine Injection, USP Auto-Injectors 0.15 mg products.
Please watch thisimportant videofromPfizer’s Chief Medical Officer, Dr. Freda Lewis-Hall, regarding this announcement.
Meridian, a subsidiary of Pfizer that manufactures EpiPen® 0.3 mg and EpiPen Jr® 0.15 mg Auto-Injectors, and the authorized generic versions of these strengths, continues to experience manufacturing constraints affecting supply. Mylan and Pfizer place great importance on the consistent availability of EpiPen for everyone who needs it. Pfizer is working tirelessly to increase production and expedite shipments as rapidly as possible. Currently, supplies will vary from pharmacy to pharmacy, and we cannot guarantee that product will be available at all pharmacies.
We understand the challenges this situation continues to pose to patients. Ensuring continuity of the supply of our medicines is paramount.
Mylan, the distributor, is expediting shipments upon receipt from Pfizer and continues to encourage patients who are experiencing difficulty accessing product to call its Customer Relations team at 800-796-9526 for assistance in locating other pharmacies. To further assist patients during this period of limited supply, Mylan recently extended its Customer Relations hours to Monday through Friday, 8 a.m. to 7 p.m. ET and Saturday through Sunday, 11 a.m. to 4 p.m. ET.
Epinephrine Injection, USP Auto-Injectors 0.3 mgNDC 49502-102-02 appears on the box
NDC 49502-102-01 appears on the individual device within the box
| Lot Number | Manufacturer’sOriginal Expiry Date | New Expiration Date (beyondmanufacturer’s originalexpiry date) |
| 6FM722 | Apr 18 | Aug 18 |
| 6FM739 | Apr 18 | Aug 18 |
| 6FM771 | Apr 18 | Aug 18 |
| 6FM772 | Apr 18 | Aug 18 |
| 6FM773 | Apr 18 | Aug 18 |
| 6FM715 | May 18 | Sep 18 |
| 6FM716 | May 18 | Sep 18 |
| 6FM756 | May 18 | Sep 18 |
| 6FM757 | May 18 | Sep 18 |
| 6FM768 | May 18 | Sep 18 |
| 6FM780 | May 18 | Sep 18 |
| 6FM781 | May 18 | Sep 18 |
| 6FM782 | May 18 | Sep 18 |
| 6FM783 | May 18 | Sep 18 |
| 6FM785 | Jun 18 | Oct 18 |
| 6FM787 | Jun 18 | Oct 18 |
| 7FM115 | Aug 18 | Dec 18 |
| 7FM117 | Aug 18 | Dec 18 |
| 7FM120 | Aug 18 | Dec 18 |
| 7FM134 | Aug 18 | Dec 18 |
| 7FM174 | Sep 18 | Jan 19 |
| 7FM175 | Sep 18 | Jan 19 |
| 7FM274 | Oct 18 | Feb 19 |
| 7FM275 | Oct 18 | Feb 19 |
| 7FM276 | Oct 18 | Feb 19 |
EpiPen® (epinephrine injection, USP) 0.3 mg Auto-InjectorsNDC 49502-500-02 appears on the box
NDC 49502-500-01 appears on the individual device within the box
| Lot Number | Manufacturer’sOriginal Expiry Date | New Use Date (beyondmanufacturer’s original expirydate) |
| 6GM480 | Apr 18 | Aug 18 |
| 6GM481 | Apr 18 | Aug 18 |
| 6GM503 | Apr 18 | Aug 18 |
| 6GM504 | Apr 18 | Aug 18 |
| 6GM506 | Apr 18 | Aug 18 |
| 6GM507 | Apr 18 | Aug 18 |
| 6GM512 | Apr 18 | Aug 18 |
| 6GM669 | Apr 18 | Aug 18 |
| 6GM599 | May 18 | Sep 18 |
| 6GM685 | Jun 18 | Oct 18 |
| 6GM766 | Jun 18 | Oct 18 |
| 6GM767 | Jun 18 | Oct 18 |
| 7GM026 | Aug 18 | Dec 18 |
| 7GM045 | Aug 18 | Dec 18 |
| 7GM048 | Sep 18 | Jan 19 |
| 7GM054 | Sep 18 | Jan 19 |
| 7GM164 | Sep 18 | Jan 19 |
| 7GM172 | Sep 18 | Jan 19 |
| 7GM173 | Sep 18 | Jan 19 |
| 7GM272 | Sep 18 | Jan 19 |
| 7GM191 | Oct 18 | Feb 19 |
| 7GM200 | Nov 18 | Mar 19 |
| 7GM201 | Nov 18 | Mar 19 |
| 7GM203 | Dec 18 | Apr 19 |
| 7GM204 | Dec 18 | Apr 19 |
| 7GM212 | Dec 18 | Apr 19 |
| 7GM213 | Dec 18 | Apr 19 |
| 7GM360 | Dec 18 | Apr 19 |
| 7GM361 | Dec 18 | Apr 19 |
Subscribe to:
Posts (Atom)