The insurer is teaming up with the physician-led value-based care organization to serve Medicare Advantage patients in southern and central California.
Humana and Heritage Provider Network (HPN) announced a value-based alliance to cater to Medicare Advantage members in California, according to a press release Wednesday.
The Marina del Rey, California-based insurer announced the collaboration in order to bolster the patient experience for Medicare Advantage customers in certain areas of the state. HPN features a network consisting of 3,600 primary care physicians and 10,000 specialists, while Humana accounts for nearly 2 million Medicare Advantage members nationwide.
Counties where Medicare Advantage HMO members will have in-network access to HPN include:
Los Angeles
Orange
Riverside
San Bernardino
Kern (as well as Dual Eligible Special Needs Plan members)
Ventura (as well as Dual Eligible Special Needs Plan members)
Leaders from both Humana and HPN celebrated the deal, with each eyeing future expansion opportunities.
“We are excited to offer our southern California Medicare Advantage members additional access to value-based care through our new relationship with Heritage,” Rick Beavin, California Medicare President for Humana, said in a statement. “By working together with Heritage, we are able to better serve Humana Medicare Advantage members and offer them high-quality care with the goal of improving their health and well-being.”
“Working with Humana brings together two highly respected, experienced organizations committed to providing better care, better health and lower costs,” Dr. Richard Merkin, CEO of HPN, said in a statement. “We will be able to coordinate care needs across our entire system and tailor healthcare services proactively that will bring added value to Humana Medicare Advantage members by increasing their access to healthcare services in all of our medical provider groups throughout Southern and Central California, creating a robust care network.”
TURN UP THE VOLUME is what people with impaired hearing sometimes say while watching TV with family or friends. But a new generation of hearing aids could change all that, provided the folks who need them are willing to use them – and are able to AFFORD them. Our Cover Story is reported by David Pogue, tech critic for Yahoo Finance:
Meet Dick Pogue, Cleveland lawyer. He’s 90 years old, he goes to the office six days a week, and he’s David Pogue’s dad. Hedoesn’t make many concessions to aging. About the only one David has noticed is that he wears hearing aids.
David asked, “Under what circumstances do you wear them? Movies?”
“I wear them at movies? Yes.”
“And watching TV?”
“I do wear them watching television.”
“Talking to mom?”
“When I’m listening to her!” Dick laughed.
Most people with hearing loss get it by getting older. Two out of three people over 70 have trouble hearing. But what’s really surprising is how many of them don’tget hearing aids.
CBS NEWS
“On average, about 20% of adults who have a hearing loss actually use a hearing aid,” said Frank Lin, an ear surgeon, professor, and director of the Cochlear Center for Hearing and Public Health at Johns Hopkins. His research shows that hearing loss is associated with higher risks of hospitalization, depression, and especially dementia.
First, the price: “The average cost to get a pair of hearing aids in the United States is about $4,700, which is remarkable, right?” Dr. Lin said. “Because that basically means then for the average American, that this could be their third largest material purchase in life after a house and a car. So, it’s incredibly expensive.”
What’s more, the majority of insurance companies don’t cover hearing aids.
But cost is only one obstacle. Some people are also embarrassed to wear hearing aids. (Many don’t realize how much smaller hearing aids have become over the decades.)
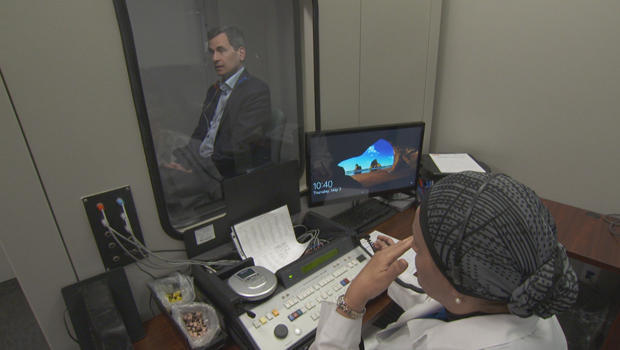
And some people are put off by the hassle of getting them.In the U.S., you can’t get hearing aids without testing and consultation with a doctor or audiologist.
David Pogue has his hearing tested.
CBS NEWS
Today, most of the world’s hearing aids are made by six companies. Only one is headquartered in the U.S., and that’s Starkey, near Minneapolis.
Starkey’s founder and CEO, Bill Austin, jokes, “I’ve been in everybody’s ears!”
Like who? “Ford, Reagan, Clinton.” And a pope, too.
While Pogue doesn’t actually need hearing aids (yet), Starkey’s team treated him to a pope-worthy fitting experience.
First, a cleaning. “You do have narrow ear canals,” Pogue was told.
Then, a hearing test. Then, a molding session, for hearing aids that will exactly fit his ears. Blue liquid plastic poured into his ear canal takes about five minutes to solidify.
Making a good impression of David Pogue’s ear canal.
CBS NEWS
Technicians have to fit all the electronics into a tiny shell that will disappear completely inside your ear. Once it’s inserted, it can’t be seen.
Or, you can get the kind that slips over and behind your ear. They have room for a lot more features; you can listen to music from your phone or make phone calls. They even have different presets for different sonic environments, like crowded rooms.
Think that sounds fancy? You ain’t heard nothing yet.
Starkey’s chief technology officer, Achin Bhowmik, met Pogue inside one of the company’s echo-proof testing chambers. He’s adding more sensors to their hearing aids, so they can notify loved ones when you’ve fallen, or monitor your steps and heartbeat like a FitBit. “We’ll transform the hearing aid with sensors and artificial intelligence to become a true gateway to your health,” he said.
Chief technology officer Achin Bhowmik with David Pogue inside one of Starkey’s echo-proof testing chambers
CBS NEWS
But probably the number-one technology most hearing-loss sufferers would like to have now is just the ability to understand someone talking across the table from them in a restaurant. Why can’t we lick that?
“I think we are close to cutting the problem,” Bhownik said. “We’re going to do that by detecting, Where are you looking? Are you looking at me? Are you looking at the person over there?”
But even basic hearing aids cost an ear and a leg, and this is why: Two-thirds of the price is all of those doctor services – testing, customization, and follow-up, all bundled in that price.
But Frank Lin became convinced that people with mild hearing loss don’t need all that. They might be content with something more generic that costs one-tenth as much. So, his team worked with Congress to successfully pass a new bill allowing hearing aids to be sold over-the-counter, which means that, by August of 2020, companies will be able to sell hearing aids directly to consumers. “Companies like Bose, Samsung, Apple could all enter the market now,” Lin said.
He says access to hearing aids will be improved, and costs will come down.
As for the big companies making hearing aids now, “You’re taking direct aim at their spreadsheet,” Pogue noted.
“Yes and no,” Dr. Lin said. “It’s an industry, and a profession, and a practice that’s been built up over the last several decades. And now we’re disrupting the model. If we think hearing is so important for public health, then that’s how we need to advance the field.”
The new law will create a new class of hearing aids much less customized, but also much less expensive. They may resemble these devices, called personal sound amplification products, or PSAPs.
Personal sound amplification products (PSAPs), such as the SuperEar (left) and Bose’s Hearphones.
CBS NEWS
These PSAPs are on the market today, but legally they can’t be called or marketed as hearing aids.
But when the new law kicks in, several of these PSAPs might be allowed to be called that, said Nicholas Reed, an audiologist at the Johns Hopkins School of Public Health.
Some of these over-the-counter devices have some pretty cool features, too, such as the SuperEar, which has a microphone that clips onto your lapel. It retails for around $80.
Then there are the Bose Hearphones, for $500. “These have noise cancellation,” said Reed. He said that in tests done in a controlled environment, devices that cost several hundred dollars improved speech understanding about as well as hearing aids costing several thousand.
As you could probably guess, the big hearing aid companies say they’re not as good as their products. “In a restaurant or backgrounds of noise, they just don’t perform,” said Chris McCormick, the chief marketing officer at Starkey.
“So, what’s going to happen when people are allowed to buy hearing aids without the audiologist’s services?” Pogue asked.
Hearing aid user Dick Pogue.
CBS NEWS
“The concern is people trying to self-diagnose, people trying to self-program,” McCormick replied. “The products will have to be standardized. And the problem with that is, everybody’s hearing is different.”
Bottom line: the world of hearing aids is about to improve dramatically, both at the expensive end, and – thanks to that new law – over-the-counter.
In the meantime, if you’re among the 80 percent who could use hearing aids but haven’t looked into it, well, we’ll give the last word to David’s dad, Dick.
When asked if he could imagine his life without hearing aids, he said, “Well, I wouldn’t be able to work. I mean, I couldn’t go to meetings, I couldn’t hear people. It would just cause me to isolate myself and be at home and very seldom go out. It would be a dramatically different life.
In elementary school, children get the talk about unwanted touching. In college, they learn about boundaries and what constitutes assault.
But in between, sex education in schools is often an antiseptic regurgitation of the science of reproduction mixed with healthy doses of the need for protection and, increasingly, abstinence.
As it is, only 24 states and the District of Columbia mandate sex educationin public schools, the study found.
Of those, only eight states require mention of consent or sexual assault, it said: California, Hawaii, New Jersey, North Carolina, Oregon, Rhode Island, Vermont and West Virginia. (The District of Columbia does, too.)
“States are not providing students with enough guidance and support in terms of how to behave in the world they grew up in,” Catherine Brown, the vice president of education policy at the institute, told CNN.
“It’s really important to be clear with them about what is and what isn’t permissible and the lines are when dealing with other people in relationships.”
Rhode Island, West Virginia and the District of Columbia provide clear standards on topics of sexual health and categorize them by age group, the Center for American Progress found. For example, DC standards require that third-grade students are taught how “individual bodies are different” and sixth-graders learn about “sexual feelings and the need for love, affection and physical intimacy.”
But most of the states the study looked at — including Georgia, South Carolina, Kentucky and Nevada — provide little detail on what the curriculum should look like and don’t separate standards by age.
Delaware, for example, requires that the curriculum of its health education for students includes “sexuality education and an HIV prevention program that stresses the benefits of abstinence from high-risk behaviors.”
And two states, Tennessee and Montana, stress abstinence-only education and STDs, a practice that Brown said has never proven to work on reducing teen sexual activity and pregnancies.
“The research shows the opposite,” Brown told CNN. “The students who participate in (comprehensive sex ed courses) are less likely to have sex.”
“You have some states that are teaching inaccurate information,” she said. “Students deserve to have age-appropriate, helpful information about how to behave in intimate relationships.”
Some are making progress
Still, some states are trying to enact reforms to their sex ed programs.
The legislature in Missouripassed a bill this summer to add lessons about sexual harassment, sexual violence and consent to sex education.
Rhode Island‘s governor signed a bill in July permitting age-appropriate education on consent and sexual activity to be increased in “family life” courses in schools.
And in Maryland, the governor approved a bill requiring age-appropriate instruction on the meaning of consent as an “unambiguous and voluntary agreement,” starting in the current school year.
The change has a lot to do with the recent movement that’s sparked conversation around sexual assault and workplace harassment, Brown said.
“There definitely is more interest in this topic since the #MeToo movement,” she said. “We are seeing more interest in pushing legislation that would clarify that you should teach consent and sexual abuse.”
Children’s body mass index (BMI) category in the first years of life was often carried through to adolescence, a German population-based study showed.
Most children stayed in the weight group they were in at age 5 through into ages 15 to 18, Antje Körner, MD, of the University of Leipzig, Germany, and colleagues reported in the New England Journal of Medicine.
Age 2 to 6 appeared to be a critical period: While 50% of those overweight (BMI standard-deviation score of 1.28 to <1.88) at 2 or younger achieved normal weight in adolescence, almost 90% of those who were obese (BMI SD score of 1.88 to <5) at age 3 were overweight or obese in adolescence.
The trajectory to obesity in the teen years followed a growth spurt from ages 2 to 6, with a 1.4-fold greater risk of overweight or obesity than seen among children with stable BMI in the preschool years.
High birthweight was a risk factor too, as 43.7% of those born large for gestational age were overweight or obese in adolescence. That corresponded to a 55% elevated risk of obesity in the teen years compared with other children.
The good news was that lower-weight preschoolers uncommonly became obese as teens.
Because teen obesity tends to carry over into adulthood, with metabolic and cardiovascular consequences, the findings have implications for identifying at-risk children based on early dynamics and patterns of BMI, Körner’s group noted.
“With regard to prevention, the clinical manifestation of obesity is a late starting point.” An annual increase of 0.2 or more in the BMI standard-deviation score during the preschool years “can be regarded as an early sign of ensuing obesity in adolescence that appears much earlier than the actual clinical manifestation of overweight.”
“A practical clinical implication of our study results would be surveillance for BMI acceleration, which should be recognized before 6 years of age, even in the absence of obesity.”
The researchers suggested tracking growth and weight patterns, particularly in those with maternal overweight or large-for-gestational-age status at birth, to prompt early intervention. “It is therefore important for healthcare professionals, educational staff, and parents to become more sensitive to this critical time period.”
The population-based study included 51,505 children with at least one measure of height and weight by age 14 and another at age 15 to 18, collected by pediatricians participating in the CrescNet patient registry at well-child or other office visits. The weight categories followed German national guidelines.
The findings were largely in line with prior studies, although those assessed a smaller age span or had limited sample size, the researchers noted. Studies that were well-powered missed the period from 2 to 7 years of age, “and hence began after the most pronounced weight gain had occurred.”
In an accompanying editorial, Michael Freemark, MD, of Duke University Medical Center in Durham, N.C., called the findings important, cautioning, however, that extrapolation to children in other countries is unclear, particularly in the developing world where the timing and magnitude of changes in BMI are often different from in Germany.
Another limitation was the inability to determine causality, he added, suggesting a clinical trial of early dietary intervention.
“We are now witness to an evolving epidemic of childhood obesity in the United States and other westernized countries … It is an ominous sign that the number of American children with the most severe and recalcitrant forms of obesity has increased progressively during the past 10 years. One hopes that interventions tailored to high-risk children at an early age can help to prevent or limit excess weight gain before obesity becomes irreversible.”
The study was supported by the German Research Council for the Clinical Research Center, German Federal Ministry of Education and Research, and Leipzig Research Center for Civilization Diseases (LIFE Child, supported by the European Union, the European Regional Development Fund, and the Free State of Saxony).
The CrescNet registry infrastructure was supported by grants from Hexal Germany, Novo Nordisk Pharma, Merck Serono Pharma, Lilly Deutschland, Pfizer Pharma, and Ipsen Pharma.
Körner reported financial relationships with the German Research Council, the European Regional Development Fund, the Federal Ministry of Education and Research, and Merck Serono, as well as non-financial support from Ferring Arzneimittel, Ipsen Pharma, and Eli Lilly.
Freemark reported grants from Rhythm Pharmaceuticals, the American Heart Association, and the Humanitarian Innovation Fund and European Commission, and personal fees from Springer Publishing.
Viking Therapeutics, Inc. (‘Viking’) (NASDAQ: VKTX), a clinical-stage biopharmaceutical company focused on the development of novel therapies for metabolic and endocrine disorders, today announced positive new findings from the company’s 12-week, Phase 2 clinical trial of VK5211 in patients who recently suffered a hip fracture.
As previously reported, the trial achieved its primary endpoint, demonstrating statistically significant, dose-dependent increases in lean body mass, less head, following treatment with VK5211 as compared to placebo. Additionally, newly presented data demonstrated dose-dependent decreases in mean fat mass, coupled with dose-dependent increases in mean body weight following VK5211 treatment. Findings also demonstrated dose-dependent increases in 6-minute walk distance following VK5211 treatment, reaching a greater than 20-meter improvement over placebo at the study’s highest dose. The results were presented as part of the oral plenary session of the American Society for Bone and Mineral Research (ASBMR) 2018 annual meeting, held September 28 – October 1, 2018 in Montreal, Quebec, Canada.
VK5211, Viking’s lead program for musculoskeletal disorders, is an orally available, non-steroidal selective androgen receptor modulator (SARM) designed to selectively stimulate muscle and bone formation with reduced activity in peripheral tissues such as skin and prostate. The Phase 2 clinical trial was a randomized, double-blind, placebo-controlled, parallel group, international study designed to evaluate the efficacy, safety and tolerability of VK5211 in patients recovering from hip fracture surgery. A total of 108 patients were randomized to receive once-daily VK5211 doses of 0.5 mg, 1.0 mg, 2.0 mg, or placebo for 12 weeks.
Nymox Pharmaceutical Corporation (NASDAQ:NYMX) reported today that after long-term safety assessments of repeated Fexapotide Triflutate (FT) intraprostatic injections, there have been no identifiable risks or serious side effects or adverse events identified associated or linked with the drug.
FT is Nymox’s lead drug for which the Company is in the process of seeking U.S. and European marketing approvals for BPH (prostate enlargement), and FT is also in late stage development for prostate cancer. Pivotal trial results for FT BPH studies involving 977 treated patients were published in 2018 in the prestigious World Journal of Urology (May 2018, Volume 36, pages 801–809), and the safety and efficacy results have been presented to the American Urology Association and previously to the European Association of Urology.
Dr. Paul Averback, CEO of Nymox said, “For prostate cancer in particular, repeated injection treatments will be needed and a focal molecular treatment will have negligible value if there cannot be reliable safety expected from repeated injection. Prostate cancer is a multi-focal disease and it is to be expected that multiple focal molecular treatments will be utilized for optimal outcomes. Follow-up and re-treatment will be needed. Nymox undertook 2 large FT re-injection safety studies in 2010-2014 involving 351 subjects with BPH, who were subsequently followed for up to 7 years. These mandatory and adequately sized safety studies are absolutely required in order to demonstrate safety of re-injection, and this is a standard requirement.”
Dr Averback added, “In addition, Nymox undertook extensive immunological testing involving over 1000 subject samples, demonstrating that FT does not lead to detectable antibody formation, which underlines FT safety and supports the lack of risk for allergic reactions. All laboratory testing and sexual function tests including semen analyses showed no changes in FT treated men compared to controls.”
Nymox’s lead drug Fexapotide (FT) has been in development for over 10 years and has been tested by expert clinical trial investigative teams in over 70 distinguished clinical trial centers throughout the US, and has been found after 7 years of prospective placebo controlled double blind studies of treatment of 977 U.S. men with prostate enlargement to not only show clinically meaningful and durable relief of BPH symptoms, but also to show a major reduction in the incidence of prostate cancer, compared to placebo and compared to the known and expected normal incidence of the disease. The same clinical program has also shown in a long-term blinded placebo group study an 82-95% reduction in the number of these patients who required surgery after they received FT in the trial, as compared to patients who did not receive FT but instead later received conventional approved BPH treatments (p<.0001).
FT has been shown to produce long-term improvements in lower urinary tract symptoms associated with prostate enlargement (BPH), a problem that afflicts an estimated 100 million or more men in the world. FT does not cause the annoying side effects and risks found with available treatments for BPH. FT is also in development for low grade prostate cancer.
The clinical trial results for Fexapotide treatment of BPH are published in the World Journal of Urology May 2018, Volume 36, pages 801–809 (https://doi.org/10.1007/s00345-018-2185-y) in a peer review report entitled “Fexapotide Triflutate: Results of Long- Term Safety and Efficacy Trials of a Novel Injectable Therapy for Symptomatic Prostate Enlargement” authored by Neal Shore, MD, FACS (Carolina Urologic Research Center, Myrtle Beach, SC); Ronald Tutrone, MD, FACS (Chesapeake Urology Research Associates, Baltimore, MD); Mitchell Efros, MD, FACS (Accumed Research, Garden City, NY); Mohamed Bidair, MD (San Diego Clinical Trials, San Diego, CA); Barton Wachs, MD (Atlantic Urology Medical Group, Long Beach, CA); Susan Kalota, MD (Urological Associates of Southern Arizona, Tucson, AZ); Sheldon Freedman, MD, FACS (Freedman Urology, Las Vegas, NV); James Bailen, MD, FACS (First Urology, Louisville, KY); Richard Levin, MD, FACS (Chesapeake Urology Research Associates, Towson, MD); Stephen Richardson, MD (Jean Brown Research, Salt Lake City, UT); Jed Kaminetsky, MD, FACS (University Urology, New York, NY); Jeffrey Snyder, MD, FACS (Genitourinary Surgical Consultants, Denver, CO); Barry Shepard, MD, FACS (Urological Surgeons of Long Island, Garden City, NY); Kenneth Goldberg, MD, FACS (U T Southwestern Dept of Urology, Lewisville, TX); Alan Hay, MD, FACS (Willamette Urology, Salem, OR); Steven Gange, MD, FACS (Summit Urology Group, Salt Lake City, UT); Ivan Grunberger, MD, FACS (Brooklyn Urology, Brooklyn, NY).
Leidos announced today it is joining Cerner, a global leader in health care technology, and other industry leaders and innovators to help make seamless care available to the nation’s veterans. This newly formed team announced by Cerner will bring extensive experience in large enterprise systems and commercial sectors to modernize the U.S. Department of Veterans Affairs (VA) electronic health record (EHR).
“As lead systems integrator for the DoD’s Defense Healthcare Management Systems Modernization (DHMSM) program, we are pleased that the deployment of MHS GENESIS will now include the VA,” said Jerry Hogge, senior vice president, Leidos. “We look forward to continuing our partnership with Cerner, further strengthening our joint mission to deliver an enhanced healthcare solution for both our active duty military, as well as our Veterans and their families.”
In addition to Cerner, Leidos will join Guidehouse, Accenture, Henry Schein One, AbleVets LLC, MicroHealth, ProSource360 and 17 additional small businesses – many of which are veteran-owned – to form the team that will provide experience and expertise to the VA implementation.
“We are proud Leidos will be part of this important team of industry leaders that will shape the future of care for veterans through a modern EHR system,” said Travis Dalton, president, Cerner Government Services. “We will work together to address the needs and capabilities that are in the best interest of the VA. Our veterans deserve the highest quality care and with this team, we look forward to bringing a modern, seamless system to those who have served our country.”
In May, Cerner announced an historic agreement and VA made the program one of their top priorities to improve care for veterans. Using technology that has been deployed successfully at Department of Defense (DoD) medical facilities and thousands of provider sites globally, Cerner plans to provide seamless care across the VA’s high-performing integrated network, including VA facilities, community providers and DoD facilities.
Leidos will join Cerner and other VA EHR modernization members to outline the strategy during the Cerner Health Conference, Oct. 8-11, in Kansas City, Mo.