A recent clinical trial assessing the safety of weight-loss drugs Belviq and Belviq XR (lorcaserin) has led to the FDA issuing a public alert, warning that the drug may contribute to cancer risk.
“At this time, the cause of the cancer is uncertain, and we cannot conclude that lorcaserin contributes to the cancer risk,” reads the statement. “However, we wanted to make the public aware of this potential risk.”
Lorcaserin was approved by the FDA in 2012 for assisting weight-loss in combination with a reduced-calorie diet and increased physical activity in obese or overweight adults. The drug works by increasing feelings of fullness to reduce the amount of food eaten and is available in two tablet-based forms, Belviq and Belviq XR.
In one academic study from 2011, the drug did show the propensity to cause several different types of cancer in rat models, albeit at doses larger than the recommended clinical dose in humans. The FDA originally rejected the approval of the drug in 2010 based on these results, but later concluded that the development of these tumors were rodent-specific and unlikely to happen in humans.
“We are continuing to evaluate the clinical trial results and will communicate our final conclusions and recommendations when we have completed our review,” reads the statement.
There are currently 49 clinical trials listed on clinicaltrials.gov involving lorcaserin for a number of indications and 9 are currently recruiting participants or will start shortly. It is currently unknown whether the new findings will affect any of these trials as well as the recommended prescription of the drug for weight-loss.
The FDA statement urges healthcare professionals to “consider if the benefits of taking lorcaserin are likely to exceed the potential risks when deciding whether to prescribe or continue patients on lorcaserin.”
Patients are urged to talk to their healthcare professionals about the potential increased risk of cancer associated with using the drug.
CVS Health’s top executive said its stores are focused on offering “80% of what a primary care physician can treat” as it rolls out its new HealthHub format and “zero” and “low copays” for certain Aetna health plan members using CVS services.
Speaking at the JPMorgan Chase Healthcare conference Tuesday, CVS chief executive Larry Merlo said the company remains on track to have 1,500 HealthHUBs operating by the end of 2021. This comes after the first 50 HealthHubs opened last year in four markets: Houston, Atlanta, Tampa and the market that includes Philadelphia and southern New Jersey.
“We now have about 600 HealthHUBs scheduled for this year, 1500 by the end of 2021,” Merlo told JPMorgan analyst Lisa Gill in an interview webcast from the bank’s annual healthcare meeting in San Francisco.
“We are confident we are on the right path to creating the most consumer-centric healthcare company,” Merlo said. “We have completed a tremendous amount of work over the last 13 months.”
CVS in December of 2018 closed on its acquisition of Aetna, the nation’s third-largest health insurer with more than 20 million customers. As a larger healthcare company that is benefitting from Aetna health plan members, CVS is dedicating more than 20% of its stores to health services that include new durable medical equipment, supplies and various new product and service combinations.
CVS executives say the HealthHubs will tend to be rolled out where there are a large concentration of Aetna members. “There is a direct link between the ZIP codes associated with Aetna membership and the locations of these HealthHUBs,” Merlo said.
CVS is rolling out new health plans this year that feature “zero” and “low copayments” for Aetna members who use CVS HealthHubs and the drugstore services, CVS executives on the JPMorgan panel with Merlo said Tuesday.
Though not all of CVS’ more than 9,800 retail locations will convert to HealthHub locations, Merlo said CVS is adding new healthcare services and new personal care items at all of its stores as well as additional services at its MinuteClinics.
The move to add new healthcare services comes as rival retailers in the healthcare space like Walgreens Boots Alliance and Walmart look to fill the emptying space in their brick and mortar stores in the face of changing consumer shopping habits driven by online retail giant Amazon and others.
But Merlo told JPMorgan’s Gill “there is a physical role for bricks and mortar.” As new healthcare services and personal items have been added to the HealthHubs, CVS is seeing more foot traffic and more purchases. “We see the HealthHubs has an evolution of the drugstore,” Merlo said. “We talk about the need to make healthcare local.”
How cool is this: the Massachusetts General Hospital (MGH) laboratory that invented cryolipolisis or “Coolsculpting,” a popular non-surgical method for reducing fat under the skin, is developing a new form of the technology that can selectively reduce fat almost anywhere in the body using a safe, injectable ice solution or “slurry.”
The technology, not yet approved for use in humans, is designed for removal of fat in the abdomen or other parts of the body—virtually anywhere that can be reached with a hypodermic needle. Fat is a normal part of our bodies, but in excess or with some diseases can be life-threatening.
The new technique is described in a paper published online ahead of print in the journal Plastic and Reconstructive Surgery. As one of the reviewers of the paper said, “this treatment has the potential to become one of the most performed cosmetic procedures in plastic surgery practice.”
“The appeal of this technique is that it’s easy and convenient to do,” says lead author Lilit Garibyan, MD, Ph.D., investigator in the Wellman Center for Photomedicine at MGH and the Department of Dermatology at Harvard Medical School. “With Coolsculpting, which is a topical cooling technique, the patient has to sit there for almost an hour for enough heat to diffuse from the fat underneath the skin. With this new technique the doctor can do a simple injection that takes just less than a minute, the patient can go home, and then the fat gradually disappears.”
Cryolipolysis is currently the leading non-invasive fat removal technology because of its minor side effects and non-invasive nature. The Coolsculpting method is limited, however, by the amount of fat that can be removed per treatment, and is not practical for reaching more deeply seated fat surrounding organs or other body structures.
The MGH team’s innovative spin on the technique involves the use of an injectable ice “slurry,” a sterile solution of normal saline and glycerol (a common food ingredient) containing approximately 20% to 40% small ice particles, similar in texture to slush. The solution can be injected directly into fat deposits, causing the fat cells (adipocytes) to crystallize and die and fat deposits to shrink. The killed adipocytes are gradually eliminated by the body over a period of weeks. “One of the cool things about this is how the injected slurry causes selective effects on fat,” said Rox Anderson, MD, a co-author and leader of the Wellman Center. “Even if the slurry is injected into other tissue such as muscle, there is no significant injury.”
As the investigators report, injection of the ice solution into pigs resulted in a 55% reduction in fat thickness compared to that of pigs injected with the same but melted ice solution. There was no damage to skin or muscle at the injection site, and no systemic side effects or abnormalities seen.
Unlike topical cooling, slurry injection can target and remove fat tissue at essentially any depth and any site that can be accessed by a needle or catheter. Injection of physiological ice slurry could be a transformative method for nonsurgical body contouring.
More information: Lilit Garibyan et al, Subcutaneous Fat Reduction with Injected Ice Slurry, Plastic and Reconstructive Surgery (2020). DOI: 10.1097/PRS.0000000000006658
Hospitals that launch robotic surgery programs have a broad and immediate increase in the use of robotic surgery, accompanied by a decrease in traditional laparoscopic minimally invasive surgery, according to a study published online Jan. 10 in JAMA Network Open.
Kyle H. Sheetz, M.D., from University of Michigan in Ann Arbor, and colleagues used clinical registry data from Michigan (Jan. 1, 2012, through June 30, 2018) to assess trends in the use of robotic surgery for common procedures for which traditional laparoscopic minimally invasive surgery was already considered a safe and effective approach.
The researchers identified 169,404 patients (mean age, 55.4 years; 53.5 percent women) at 73 hospitals. The use of robotic surgery increased 8.4-fold (1.8 percent in 2012 to 15.1 percent in 2018), with the magnitude even greater for some procedures (inguinal hernia repair, 0.7 to 28.8 percent). In the first four years after hospitals began performing robotic surgery, its use increased 8.8 percent. This increase was associated with a decrease in laparoscopic surgery (53.2 to 51.3 percent), which had previously been increasing 1.3 percent per year before adoption of robotic surgery.
“These findings highlight a need to continually monitor the adoption of robotic surgery to ensure that enthusiasm for new technology does not outpace the evidence needed to use it in the most effective clinical contexts,” the authors write.
One author disclosed financial ties to ArborMetrix.
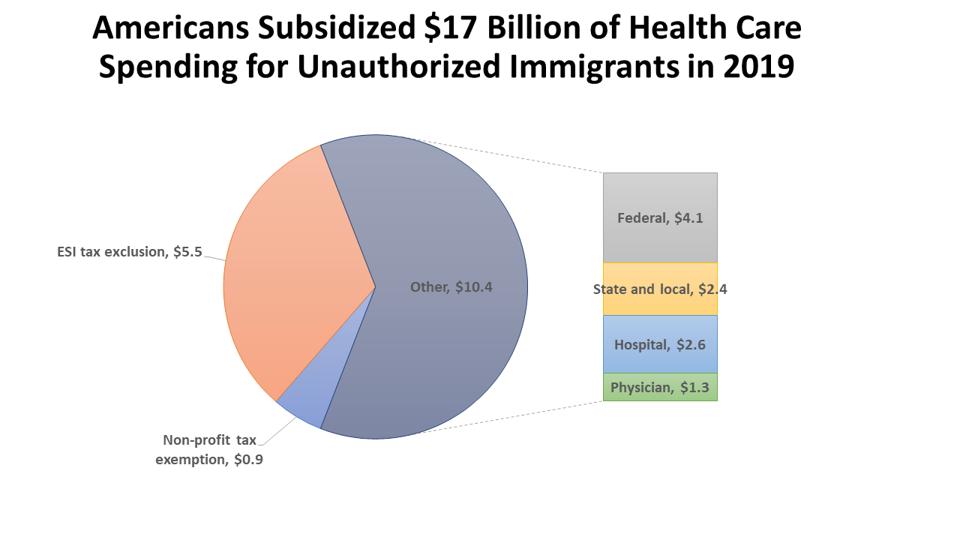
All told, Americans cross-subsidize health care for unauthorized immigrants to the tune of $17.0 billion a year. Federal taxpayers provided $10.0 billion in subsidized care to unauthorized immigrants in 2019. The total amounts to $1,615 per unauthorized immigrant, imposing a burden of $51 per U.S. resident.
Current federal policy is to prohibit federal tax funding of health care to unauthorized immigrants through either Medicaid or Obamacare. Two years ago, I did a deep dive showing that despite these statutory prohibitions, Americans nevertheless provided at least $18.5 billion in subsidized health services for unauthorized immigrants in 2016. Today I want to explore whether that reality has appreciably changed under the Trump administration.
Nevertheless, rough estimates suggest that the nation’s 4.1 million uninsured immigrants who are unauthorized likely receive about $4.1 billion in health services paid for by federal taxes, $2.4 billion in health services financed by state and local taxpayers, another $2.6 bankrolled through “cost-shifting” i.e., higher payments by insured patients to cover hospital uncompensated care losses, and roughly $1.3 billion in physician charity care. In addition to these amounts, unauthorized immigrants likely benefit from at least $0.9 billion in implicit federal subsidies due to the tax exemption for nonprofit hospitals and another $5.5 billion in tax expenditures from the employer tax exclusion.
All told, Americans cross-subsidize health care for unauthorized immigrants to the tune of $17.0 billion a year . Of this total, federal taxpayers provided $10.0 billion in subsidized care to unauthorized immigrants in 2019 .
Americans Subsidized $17 Billion of Health Care
PRODUCED BY CHRISTOPHER J. CONOVER, DUKE UNIVERSITY, USING METHODS AND SOURCES DESCRIBED IN POST.
In this post, I describe in more detail current policy, current sources of funding for health care of unauthorized immigrants. In a previous post, I offered four independent reasons federal tax funding for such care is a bad idea (that is, a reader need only accept one, not all, in order to conclude we should dispense with such funding).
Current Policy Regarding Federal Funding of Health Care for Unauthorized Immigrants
The purported intent of federal policy is to prevent federal tax dollars from being used to fund health care for unauthorized immigrants except in extreme circumstances. Notwithstanding express prohibitions contained in the statutes related to Medicaid and Obamacare, there also are companion federal programs that permit federal funding to be used for health care of unauthorized immigrants indirectly. While the Trump administration has taken various steps to reduce the number of unauthorized immigrants, there have been no overt changes in policy regarding use of federal funds to finance health care for such individuals. Thus, what follows is largely unchanged from my post from two years ago.
Where Use of Federal Dollars to Fund Health Care for Unauthorized Immigrants is Expressly Prohibited
Moreever, states can and do use state-only Medicaid programs to cover such individuals. For example, California’s Health for All Kids Act provides unauthorized immigrant children with access to coverage through Medi-Cal, the state Medicaid program. Its passage in 2015 made California the largest state to use state-only funding to provide coverage to all children regardless of immigration status; in doing so, it joins New York, Illinois, Massachusetts, Washington, and the District of Columbia.
ACA. Under the ACA, immigrants must be lawfully present to purchase insurance in a Qualified Health Plan, or to be eligible for an Advance Payment for Premium Tax Credit or Cost-Sharing Reduction. Under legislation signed by Governor Jerry Brown in June 2016, California would have been the first state to allow unauthorized immigrants to purchase health plans through its insurance exchange without fear that their information would be shared with other government agencies. The law directed California’s exchange, Covered California, to apply for a State Innovation Waiver to allow people who would be eligible for the exchange if not for their immigration status to purchase California Qualified Health Plans (QHPs), which provide benefits identical to those included in other ACA-compliant QHPs. This policy requires a waiver because it involves an alteration to the original terms of the ACA, which bars the participation of unauthorized immigrants in state exchanges. However, this waiver request was withdrawn on January 18, 2017.
Where Use of Federal Dollars to Fund Health Care for Unauthorized Immigrants is Indirectly Permitted
The “clear intent” of restrictions embedded in Medicaid and Obamacare is undercut by several end-arounds that allow health care for unauthorized immigrants to be indirectly funded using federal dollars.
Medicaid DSH Payments. First, there is a source of Medicaid financing that indirectly benefits unauthorized immigrants: DSH payments [2]. Kaiser Family Foundation reports “DSH, or “disproportionate share” hospitals are hospitals that serve a large number of Medicaid and low-income uninsured patients…At the facility level, Medicaid DSH payments are limited to 100 percent of the costs incurred for serving Medicaid and uninsured patients that have not been compensated by Medicaid (Medicaid shortfall).” The DSH program simply provides a general subsidy against a hospital’s aggregate uncompensated care losses from uninsured patients. Nothing requires hospitals to back out their spending on uncompensated care for unauthorized immigrants from their aggregate losses; consequently, federal Medicaid funds end up indirectly subsidizing their care even though it would be expressly illegal to pay for their care by making them direct Medicaid recipients.
Medicare DSH Payments. In a similar fashion, although the formula is much more complicated, Medicare also pays hospitals a DSH payment that effectively serves as a general subsidy to offset aggregate uncompensated care losses without making any distinction between uncompensated costs generated by unauthorized immigrants and those generated by American citizens or legal immigrants.
Community Health Centers. Federally qualified health centers provide primary healthcare, dental, mental health and pharmacy services. They treat all comers without concern for immigration status or ability to pay for care.
Tax Exemption. Nonprofit hospitals (and other health facilities) receive tens of billions of dollars annually in benefits from the federal tax exemption including forgone taxes, public charitable contributions, and the value of tax-exempt bond financing. Unauthorized immigrants benefit from this federal largesse.
Employer Tax Exclusion. The employer tax exclusion provides an indirect federal tax subsidy to everyone with employer-sponsored health insurance. Noncitizen immigrants are admittedly less likely to have such coverage than natives, but the differential is less than 10 percentage points after adjusting for the most important demographic/socioeconomic characteristics.
From where I sit (a libertarian-leaning conservative health reformer), current policy makes a lot of sense. It allows states or localities to opt to provide health care for unauthorized immigrants using local tax resources. In a country of 330 million people with deeply divided views on this issue, the federalist approach seems far preferable to trying to adopt a one-size-fits-all policy that forces tens of millions of federal taxpayers to subsidize lawbreakers against their will.
Moreover, my view is that if the intent of federal policy is to prevent taxpayer resources from being used to finance health care for unauthorized immigrants, federal officials have an obligation to be vigilant this does not occur inadvertently and a parallel obligation to be transparent if it does. That was the purpose of my writing an earlier post on this issue 20 months ago.
Current Funding for Health Care of Illegal Immigrants
Uninsured Unauthorized Immigrants. According to Pew Research Center, there were 10.5 million unauthorized immigrants in the U.S. in 2017. This is the latest figure available and smaller than the 11.3 million figure I used to develop my 2016 estimate of spending on health care for unauthorized immigrants.
Currently, 14.9% of the non-elderly uninsured (4.1 million) are unauthorized immigrants who are ineligible for both Medicaid and ACAcoverage under federal law. For purposes of discussion, I am going to focus principally on financing health care for unauthorized immigrants who are uninsured since we know that about 70% of care for America’s uninsured is uncompensated, meaning that ultimately it is paid for by society in one way or another.
In 2013 (the latest available such figures), America’s uninsured generated $84.9 billion in uncompensated care costs [Table 2] or $1,257 per person who was ever uninsured that year [Table 1]. Of this:
39% was covered by various federal programs (e.g., disproportionate share payments to hospitals);
23% by state and local governments (e.g., via taxpayer support of state and locally owned hospitals);
12% came in the form of physician charity care covered;
25%—was covered by hospitals (arguably by “cost-shifting” i.e., higher charges to privately insured patients that effectively cross-subsidize care for patients who do not pay full freight etc.). An unknown fraction of this stems from EMTALA—the Emergency Treatment and Active Labor Act—a federal law that requires hospitals to treat emergency patients regardless of their ability to pay. EMTALA is an example of “taxation by regulation” insofar as the same outcome might have been achieved by using tax dollars to pay hospitals to treat such patients voluntarily.
Between 2013 and 2018, the average daily uninsured rate declined by 35% (dropping from 14.4% to 9.4% according to the National Health Interview Survey). One might suppose that uncompensated care levels would decline in direct proportion. However, according to the American Hospital Association, hospital uncompensated care declined only 18% between 2013 and 2017 even though the average daily uninsured rate declined by 37% during the same period. In the shorthand of economists, the elasticity of uncompensated care spending with respect to uninsured risk is .5: for every 10% change in uninsured risk there is only a 5% reduction in uncompensated care spending.
Using this elasticity estimate to the observed change in uninsured risk from 2013 to 2018, I have estimated there was a 16.9% reduction in uncompensated care spending between 2013 and 2019. Assuming this reduction was the same across each of the four components and that unauthorized immigrants received a pro rata share of such support (i.e., 14.9%), they account for the $10.5 billion in uncompensated care costs in 2019, financed as follows:
$4.1 billion—federal taxpayers
$2.4 billion—state and local taxpayers
$2.6 billion—hospital charity care/bad debts arguably cost-shifted to private patients
$1.3 billion—physician charity care
I recognize these back-of-the-envelope figures are crude, but they are the best estimates I could make given that the recent (2017) National Academy of Sciences report The Economic and Fiscal Consequences of Immigrationonly provides highly aggregated estimates of cost impacts, with no breakdown of how much of these costs can be attributed to health care etc.
Federal Taxpayers. It might puzzle some readers that the federal government is paying for any care for unauthorized immigrants in light of federal policy. This can happen through fraud, to be sure, but as explained earlier, most of this occurs indirectly through various federal programs that fund institutions rather than individuals. These include hospitals (Medicaid/Medicare DSH payments) and community health centers/free clinics.
Hospital Charity Care/Bad Debts. Hospitals with 501(c)(3) status are required to establish written financial assistance policies under Affordable Care Act sections 501(r). As a consequence, there is a cleaner distinction between genuine charity care and bad debts than there was in the past when hospitals adopted very disparate practices about how to treat situations where a patient was not expected to pay (charity care) versus not able to pay (bad debt).
Let me concede that there is only limited evidence that hospitals engage in what’s called “dynamic cost shifting.” That is, if a hospital’s uncompensated care burden rises by $1 million, only some, not all, of that amount can be expected to be recovered by the hospital’s increasing charges to privately insured patients to make up the difference.
That said, hospitals can and do exercise market power, meaning they are able to charge private patients a higher rate than Medicare or Medicaid patients. This practice results in profits from private patients that then are used by the hospital in various ways, including the provision of charitable care.
The point being that if the federal government eliminated whatever payments it now makes for uncompensated care (including that generated by unauthorized immigrants), hospitals hypothetically would not respond by increasing charges to recover part of their increased uncompensated care costs, but instead make adjustments in the form of either spending less on other things or taking steps to discourage unauthorized immigrants from showing up at their doors.
Conversely, if federal, state or local governments were to make hospitals entirely whole regarding their uncompensated care losses to unauthorized immigrants, this would not necessarily benefit hospital patients in the form of lower charges. For these reasons, it is not altogether obvious that these hospital uncompensated care losses are a problem that can be solved by better public policy. Nevertheless they manifestly are a public policy issue from the standpoint of patients concerned about high health costs.
Physician Charity Care.The $1.3 billion in physician charity care represent an average of $1,414 for each of the country’s 893,000 active physicians. According to Medscape’s Physician Compensation Report for 2017, the average physician makes $294,000 a year. Even generously assuming a 60 hour workweek, that’s roughly $100 hourly meaning the average physician devotes 14.1 hours a year to charity care for unauthorized immigrants (less if we assume a higher hourly rate).
Note that physicians, receive no tax benefits for providing charity care; that is, they cannot write off the cost of charity care from their personal or business taxes. Consequently, although physician charity care is an important component of the uncompensated care landscape, in my view, these voluntary donations of time—a longstanding worthy tradition in American medicine—do not pose a public policy concern.
Other Federal Subsidies Benefiting Unauthorized Immigrants
Although it presumably did not arise by a deliberate intent to benefit unauthorized immigrants, current tax policy likely confers an additional $6.4 billion in additional benefits financed by U.S. taxpayers. The tax exemption for nonprofit hospitals (and any other nonprofit health facilities) benefits unauthorized immigrants regardless of their insurance status. The employer tax exclusion benefits unauthorized immigrants who happen to receive employer-provided health benefits.
Tax Exemption. The value of the nonprofit tax exemption to U.S. nonprofit hospitals in 2019 was approximately $28.7 billion, including forgone taxes, public charitable contributions, and the value of tax-exempt bond financing. Assuming that 10.5 million unauthorized immigrants receive a pro rata share of this benefit, they receive roughly $0.9 billion in additional federal subsidies for their hospital care. I could locate no parallel figures for other nonprofit health facilities.
Employer Tax Exclusion. Estimating the size of these tax benefits for unauthorized immigrants is of necessity extremely rough. I could locate no reliable information on the wage distribution of such immigrants, especially among those who obtain employer-provided health benefits. According to Kaiser Family Foundation, “nonelderly lawfully present and unauthorized immigrants are as likely as nonelderly citizens are to live in a family with at least one full-time worker, but they are more likely than citizens are to be low-income, since they often work in low-wage jobs.” More concretely, nearly half (48%) of unauthorized immigrants live in low income families below 200% of the federal poverty level.
That said, as shown earlier, we know that only 4.1 million of 10.5 million unauthorized immigrants are uninsured, leaving 6.4 million with some sort of coverage. No good data exist on what fraction of these obtain non-group health coverage, but Kaiser Family Foundation’s Larry Levitt has said via Twitter that “some are buying non-group, but I’d agree that it’s primarily employer coverage.” Assuming that 91% have employer-provided coverage (which is the identical percentage among all non-elderly adults having private coverage in 2018 [1]) this would equal 5.8 million unauthorized immigrants with such coverage.
And even if we conservatively assume that such workers obtain less expensive coverage from an employer with many low-wage workers, the single premium in 2019 would be $6,189 (compared to $7.188 across all plans/industries [Fig. 6.16]). If we further conservatively assume all unauthorized workers pay no income taxes and are only liable for payroll taxes, the tax subsidy amounts to 15.3% ($947 per worker) or $5.5 billion for all unauthorized immigrants with such coverage.
Conclusion
When we sum all the figures, including $10.5 billion for the uninsured and another $6.5 billion in tax subsidies, we arrive at a grand total of $17.0 billion in subsidized health care for all unauthorized immigrants in 2019. These figures are much easier to grasp on a per capita basis:
· This amounts to a benefit of $1,615 per unauthorized immigrant
· It imposes a burden of $51 per U.S. resident.
The share that concerns me the most—$10.0 billion borne by federal taxpayers—amounts to $951 per unauthorized immigrant or $30 per U.S. resident. Admittedly, one could argue that since the amounts at stake are so small, this is not an issue worth fighting about. However, it is precisely that sort of thinking that has led us to today’s dismal reality that unfunded liabilities facing Uncle Sam now are roughly $200 trillion and rising.
So even though the dollar stakes are quite small in a federal budget that now spending at a rate of $4.8 trillion a year, I believe citizens and federal policymakers should stop pressing the Easy button and seriously ponder four important principled arguments against federal tax financing of health care for unauthorized immigrants:
“Nutritional ketosis supports diabetes reversal by reducing insulin resistance while providing an alternative fuel to glucose with favorable signaling properties,” she said at the World Congress on Insulin Resistance, Diabetes, and Cardiovascular Disease.
Low-carbohydrate nutritional patterns including ketosis have extensive clinical trial evidence for improvement of type 2 diabetes, including preliminary results from a 5-year study of 465 patients enrolled in the Indiana Type 2 Diabetes Reversal Trial that Dr. Hallberg is overseeing in her role as medical director and founder of the medically supervised weight-loss program at Indiana University Health Arnett, Lafayette.
“The ketogenic diet is not a fad diet, it’s what we used to treat people with before the advent of insulin,” said Dr. Hallberg, who has been recommending and counseling patients with type 2 diabetes to follow a ketogenic diet for nearly 10 years. “Of course, insulin has been wonderful. It’s saved so many people with type 1 diabetes. But we also misused it in type 2 diabetes. Instead of counseling people the way we used to about the food that they’re taking in to control their blood sugar, we’ve just been putting [them] on medication, including insulin.”
The American Diabetes Association and other organizations have updated their guidelines to include low-carbohydrate eating patterns for type 2 diabetes treatment, she continued. Veterans Affairs/Department of Defense recommend carbohydrate levels as low as 14%.
Dr. Hallberg, who is also medical director for Virta Health, defined a very-low-carbohydrate or ketogenic diet as less than 50 g of carbohydrates per day, or fewer than 10% of calories consumed. A low-carbohydrate diet is 51-130 g of carbohydrates per day, or 25% or fewer calories consumed, whereas anything above 25% calories consumed is not a low-carbohydrate diet. A well-formulated ketogenic diet, she continued, consists of 5%-10% carbohydrates (or less than 50 g), 15%-20% protein, and 70%-80% fat. The carbohydrates include 5-10 g per day of protein-based food, 10-15 g of vegetables, 5-10 g of nuts/seeds, 5-10 g of fruits, and 5-10 g of miscellaneous nutrients. “When we’re talking about a total carbohydrate intake per day of under 50 g, you can get a lot of vegetables and nuts in,” she said. “I like to tell my patients they’re not eating GPS: no grains, no potatoes, and no sugar.”
Recently, Dr. Hallberg and colleagues published a review in which they sought to evaluate the appropriateness of sources cited in the ADA’s guidelines on eating patterns for the management of type 2 diabetes, identify additional relevant sources, and evaluate the evidence (Diabetes Obes Metab. 2019;21[8]:1769-79). “We looked at how much evidence there is for the low-carb diet, the Mediterranean diet, the DASH [Dietary Approaches to Stop Hypertension] diet, and a plant-based diet,” she said. “We found a wide variation in the evidence for each eating pattern, but the low-carb eating pattern for diabetes has so much more evidence than any of the other eating patterns.”
In an earlier study, researchers followed 10 inpatients with diabetes in a metabolic ward for 3 weeks. Their mean age was 51 years, and their mean body mass index was 40.3 kg/m2. The patients were fed a standard diet for 7 days, then a low-carbohydrate diet (21 g per day) for 14 days (Ann Intern Med. 2005; 142[6]:403-11). After 2 weeks of the low-carbohydrate diet, their mean fasting blood glucose dropped from 7.5 to 6.3 mmol/L, and their mean hemoglobin A1c (HbA1c) fell from 7.3% to 6.8%. “The levels came down very fast,” said Dr. Hallberg, who was not involved with the study. “This is an important part of the intervention, because when you get a patient who’s tried everything, who’s injecting hundreds of units of insulin every day, you can make a huge difference in the first couple of weeks. It is not unusual for us to pull patients off of 200-plus units of insulin. This is as motivating as all get out. It also affects their pocketbook right away. This is one of the reasons our patients are able to sustain a ketogenic diet along with support: early motivation and satisfaction.”
In a longer-term trial, researchers evaluated the impact of a ketogenic diet in 64 obese patients with diabetes over the course of 56 weeks (Moll Cell Biochem. 2007;302[1-2]:249-56). The body weight, body mass index, and levels of blood glucose, total cholesterol, LDL cholesterol, triglycerides, and urea showed a significant decrease from week 1 to week 56 (P less than .0001), while the level of HDL cholesterol increased significantly (P less than .0001).
A separate trial conducted in Israel evaluated the effects of a low-carbohydrate diet, compared with a Mediterranean or low-fat diet in 322 moderately obese patients over the course of 2 years (N Engl J Med. 2008;359:229-41). The rate of adherence to a study diet was 85% at 2 years. The mean weight change was greatest for those on the low-carbohydrate diet, followed by the Mediterranean and low-fat diets. Fasting glucose was best for those on the Mediterranean diet at the end of 2 years, whereas change in HbA1c was best among those on the low-carbohydrate diet.
Another study randomized patients to a low-carbohydrate ketogenic diet (less than 20 g per day with no calorie restriction) or to a low–glycemic index diet (55% carbohydrate restriction of 500 kcal from baseline) over the course of 24 weeks (Nutr Metab [Lond]. 2008 Dec 19. doi:10.1186/1743-7075-5-36). Between baseline and week 24, the mean HbA1c fell from 8.8% to 7.3% in the very-low-carbohydrate diet group, and from 8.3% to 7.8% in the low–glycemic diet group, for a between-group comparison P value of .03. In addition, 95% of patients in the low-carbohydrate diet group were able to reduce or eliminate the number of medications they were taking, compared with 62% of patients in the low–glycemic diet group (P less than .01).
Dr. Hallberg and colleagues are currently in year 4 of the 5-year Indiana Type 2 Diabetes Reversal Study, a prospective, nonrandomized, controlled trial of carbohydrate restriction in 465 patients, making it the largest and longest study of its kind. Of the 465 patients, 387 are in the continuous-care arm, which consists of a diet from Virta Health based on principles of nutritional ketosis, and 87 patients in a usual care arm who are followed for 2 years. The trial includes patients who have been prescribed insulin and who have been diagnosed with diabetes for an average of 8 years.
At the meeting, Dr. Hallberg presented preliminary results based on 2 years of data collection. The retention rate was 83% at 1 year and 74% at 2 years. In the treatment arm, the researchers observed that the level of beta hydroxybutyrate, or evidence of ketogenesis, was the same at 2 years as it had been at 1 year. “So, people were still following the diet, as well as being engaged,” she said.
At the end of 2 years, the mean HbA1c reduction was 0.9, the mean reduction for the Homeostatic Model Assessment of Insulin Resistance was 32%, and 55% of completers experienced reversal of their diabetes. Overall, 91% of insulin users reduced or eliminated their use of insulin, and the average weight loss was 10% of baseline weight. “Medication reduction was across the board,” she added. “This is huge from a cost-savings and a patient-satisfaction standpoint. We were improving A1c levels in patients who have had diabetes for an average of over 8 years while we were getting [them] off medication, including insulin. Low carb is now the standard of care.”
Even patients who did not experience a reversal of their diabetes were conferred a benefit. They had an average reduction of 1.2 in HbA1c level, to 7%; their average weight loss was 9.8%; 45% of patients eliminated their diabetes prescriptions; 81% reduced or eliminated their use of insulin; there was an average reduction of 27% in triglyceride levels; and they had a 17% reduction in their 10-year risk score for atherosclerotic cardiovascular disease.
In the overall cohort, the 10-year Atherosclerotic Cardiovascular Disease risk score improved by 12%; almost all markers for cardiovascular disease improved at 1 year. “We were giving these patients appropriate support, which I think is key,” Dr. Hallberg said. “No matter what you do, you have to have a high-touch intervention, and supply that through technology. We do better than medication adherence. Putting patients on a carbohydrate-restricted diet with the appropriate support works for sustainability.”
Dr. Hallberg disclosed that she is an employee of Virta Health and that she is an adviser for Simply Good Foods.
For older individuals with opioid use disorder (OUD) resulting from treatment of chronic pain, buprenorphine may be a safer pain management alternative, new research suggests.
Results from a literature review conducted by investigators at the University of Kansas Medical Center, Kansas City, indicate that buprenorphine, an opioid used to treat OUD as well as chronic and acute pain, may be a better choice for pain management in chronic pain patients older than 65 years who have become addicted to opioids.
Results of the review show that in general, there is evidence to support the use of buprenorphine in older patients. It is well tolerated, it has few side effects, and it can improve pain control, study investigator Dheepthi Arakonam Ravishankar, MBBS, told Medscape Medical News.
“Some of these patients had poor pain control, poor quality of life, and these improved after buprenorphine was initiated,” she added.
The findings were presented here at the American Academy of Addiction Psychiatry (AAAP) 30th Annual Meeting.
A Growing Problem
Addiction is a growing problem among the elderly. In the United States, the number of Americans aged 50 years or older who have a substance use disorder is set to double, from 2.8 million in the years 2002–2006 to 5.7 million in 2020.
Many older individuals develop OUD after years of prescription opioid use to treat chronic pain. However, with aging comes drug metabolism changes that increase the risk for adverse events, including organ damage.
“We have noticed that over the years, our patient population [with OUD] has changed from mostly heroin-using young adults to older patients who have been receiving prescription opioids for chronic pain but are now being sent to the addiction clinic due to development of opioid use disorder,” lead investigator Roopa Sethi, MD, told Medscape Medical News.
This shift in the clinic’s clientele, she added, prompted the investigators to conduct a literature review to determine the optimal treatment for this patient population.
In all, they found nine studies on OUD in elderly patients, four of which focused specifically on the use of buprenorphine for chronic pain in the elderly.
Results showed that buprenorphine was effective as a treatment for chronic pain in patients aged 65 to 84 years. The response was better among those aged 80 years or older than among those younger than 80.
Buprenorphine also decreased sleep disturbances caused by pain, and it improved quality of life.
The medication was well tolerated. Reported side effects included constipation, nausea, dizziness, vomiting, and respiratory depression in more elderly, frail patients.
A Critical Issue
Commenting on the findings for Medscape Medical News, Carla Marienfeld, MD, addiction psychiatrist and associate professor at the University of California, San Diego, said the study sheds light on a “critical issue.”
She added that in her own practice, she has seen a “huge shift” in the number of older patients referred to her with chronic pain who are struggling with OUD.
These findings, she said, are “especially helpful” for psychiatrists. Even though psychiatrists don’t treat pain, it is useful for them to understand that a drug such as buprenorphine, which is used to treat OUD, can be beneficial for other comorbid conditions such as pain.
Marienfeld believes that psychiatrists, including addiction psychiatrists, may not be aware that buprenorphine has fewer side effects, less impact on immune response, and typically requires fewer dose adjustments than other opioids.
She often has to advise surgeons, dentists, and other providers who are the first managers of pain but who may not be aware of the nuances of such management.
These findings, she said, aid clinicians’ decision making “about what we might do to help this new, older population we are now beginning to see in our addiction clinics.”
Sethi, Ravishankar, and Marienfeld report no relevant financial relationships.
American Academy of Addiction Psychiatry (AAAP) 30th Annual Meeting: Abstract 13. Presented December 08, 2019.