I wasn’t planning on having this turn into Coronavirus Vaccine Week again around here, but we do have some news. Yesterday afternoon CureVac, the German mRNA vaccine company, reported results of their Phase III trial in 40,000 patients around the world. They weren’t good. And the data that have come out today don’t make things look any better.
The figure that came out last night was 47% efficacy, which doesn’t reach anyone’s cutoff for approval, not even for emergency use. And the slides that have been released this morning show that there are still a number of cases that are being evaluated, so that number is very likely to go down. Here’s one tweet speculating that the final number might be as low as 40%. At any rate, the big question is why this mRNA candidate is so much worse than the Moderna or Pfizer/BioNTech ones.
Actually, the first question on that topic is whether it is worse in the first place. CureVac has spent a lot of time in its public statements talking about the variants that its trial ran into and saying that these are the reason for the lower efficacy. Implicit in that is the idea that if you ran the other two mRNA vaccines in a trial right now, you’d come out with similar numbers. But I have trouble believing that. The real-world protection that we’re seeing in mRNA-vaccinated populations simply does not reflect an underlying efficacy in the 40% range. That’s the biggest argument right there.
We also have a lot of evidence that blood serum from vaccinated patients can indeed neutralize the newer variants of the coronavirus – here’s one of those papers that just came out, and there are many others. The neutralization is lower, to be sure, but still well above the range that should be protective. (And remember, that’s just the antibody side of the story – the T-cell side of things looks robust as well, although it’s harder to study). So there is evidence both in the lab and out in the streets that the existing mRNA vaccines are (so far) able to continue performing in the face of the variants. I cannot accept the hypothesis that the CureVac vaccine is functionally identical to the Moderna and Pfizer/BioNTech ones, not on the data we have now.
So if it really is inferior, then why? What are the differences between this one and the other two mRNA agents? The biggest one that I can see is that the CureVac vaccine does not use any modified mRNA bases – in fact, they have pointed to this as a feature, in the hopes that this will induce a more wide-ranging immune response. Meanwhile, the other two have made extensive use of bases like N-methylpseudouridine, in an effort to improve stability. So one possibility – a pretty likely one, in my view – is that the all-natural RNA idea has turned out to be a mistake, and that the CureVac agent is getting broken down too quickly to be effective, both inside and outside cells.
There’s also the possibility that the lipid nanoparticle formulation they’re using is in some way less effective than the ones used by the other companies. I find this less likely. For one thing, both the Pfizer/BioNTech and Moderna vaccines seem to work very well, despite being different lipid mixtures, which at least says that there not One Single Formulation that works. Second, CureVac has, as I understand it, been working with Acuitas for this part of their vaccine, the same company that has been involved with the Pfizer/BioNTech vaccine. So they would have brought their own considerable expertise to bear, you would have to think.
For now, then, I think the most likely possibility is that CureVac’s vaccine is indeed notably less effective than its competitors, and that this is due to its unmodified RNA composition. The result of all this is particularly unfortunate, since the EU and others had been counting on this one to deliver. That brings up another point that has to be emphasized again: we have been extremely fortunate.
It should be obvious by now, given the number of prominent failures, that generating an effective coronavirus vaccine is not something you can just stroll up to. As we’ve found, it’s definitely not impossible – and remember, there were plenty of doomsayers last year who were trying to tell everyone that it was, and that we’d never be able to get a vaccine at all. But it’s no sure thing, either, far from it. Ask Merck, ask GSK, ask Sanofi, ask Queensland, ask plenty of other players who have dropped out, and now ask CureVac. This also points up the crucial nature of taking all those shots on goal. There are a lot of factors that are literally beyond our control when such therapies get into clinical trials, and there are other things that we have to learn the hard way so that we can control for them the next time around. The fact that we have any vaccines at all is worth celebrating, and the fact that we have some that work so well, and with such good safety records, is a world-historical stroke of good news.
Background: Easily distributed oral antivirals are urgently needed to treat coronavirus disease-2019 (COVID-19), prevent progression to severe illness, and block transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). We report the results of a Phase 2a trial evaluating the safety, tolerability, and antiviral efficacy of molnupiravir in the treatment of COVID-19 (ClinicalTrials.gov NCT04405570). Methods: Eligible participants included outpatients with confirmed SARS-CoV-2 infection and symptom onset within 7 days. Participants were randomized 1:1 to 200 mg molnupiravir or placebo, or 3:1 to molnupiravir (400 or 800 mg) or placebo, twice daily for 5 days. Antiviral activity was assessed as time to undetectable levels of viral RNA by reverse transcriptase polymerase chain reaction and time to elimination of infectious virus isolation from nasopharyngeal swabs. Results: Among 202 treated participants, virus isolation was significantly lower in participants receiving 800 mg molnupiravir (1.9%) versus placebo (16.7%) at Day 3 (p = 0.02). At Day 5, virus was not isolated from any participants receiving 400 or 800 mg molnupiravir, versus 11.1% of those receiving placebo (p = 0.03). Time to viral RNA clearance was decreased and a greater proportion overall achieved clearance in participants administered 800 mg molnupiravir versus placebo (p = 0.01). Molnupiravir was generally well tolerated, with similar numbers of adverse events across all groups. Conclusions: Molnupiravir is the first oral, direct acting antiviral shown to be highly effective at reducing nasopharyngeal SARS-CoV-2 infectious virus and viral RNA and has a favorable safety and tolerability profile.
Competing Interest Statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare the following: PA, FL, WP, LS, and WH were employed by Ridgeback Biotherapeutics in direct support of the work reported in this manuscript. MA, WF, KM, and RB were contracted by Ridgeback Biotherapeutics in direct support of the work reported in this manuscript. JE, WP, TS, DW, CW, and WF are independent contractors who were topically related to this study within the past 36 months. MC was employed by UNC at Chapel Hill and received a grant from the National Institute of Health in direct support of the work presented in this manuscript. KM has stocks or stock options in ICON Plc. WP and WH received royalties from patents, trademarks, copyrights or other intellectual property. WH has stock or stock options and is a fiduciary offer or member of another board. LF, KB-E, AJL and ED declared no conflicts of interest. The initial draft of this manuscript was prepared by Mark Stead of Covance Clinical Research Unit Limited, UK.
Clinical Trial
NCT04405570
Funding Statement
Molnupiravir was invented at Drug Innovations at Emory (DRIVE) LLC, a not for profit biotechnology company wholly owned by Emory University, and with partial funding support from the US government. Since licensed by Ridgeback Biotherapeutics, all funds used for the development of molnupiravir by Ridgeback Biotherapeutics have been provided by Wayne and Wendy Holman and Merck.
Data from clinical trials of three experimental Alzheimer's disease drugs expected to start emerging next year could help shed light on whether U.S. regulators were justified in their controversial approval of a Biogen Inc treatment without clear evidence that it works.
In approving Biogen's Aduhelm over the objection of its own panel of outside expert advisers, the U.S. Food and Drug Administration has required a trial to confirm that the medicine will indeed slow progression of the lethal, mind-wasting disease - a process that could take several years - even as the drug is being used by patients.
But data expected much sooner on three drugs that work in a similar manner - Eli Lilly and Co's donanemab, Roche Holding AG's gantenerumab, and partners Eisai Co and Biogen's lecanemab - could give the medical community a better sense of whether Aduhelm is up to the job of slowing the ravages of Alzheimer's.
Aduhelm was approved last week based on its ability to clear a type of plaque from the brain that is believed to be a possible cause of Alzheimer's, rather than evidence that it slows disease progression. The FDA contends the plaque removal is likely to benefit patients, an assertion many experts say is unproven.
"I don't feel that we have evidence now that there's a clinical benefit from reducing amyloid," said Dr. Henry Paulson, a neurologist who leads the University of Michigan's Alzheimer’s Disease Center.
"If another independent study of a different anti-amyloid therapy shows a clear clinical benefit, it makes me much more comfortable with continued use of Aduhelm," he said.
All four drugs are antibodies aimed at reducing the accumulation of the sticky plaques composed of a protein called beta amyloid found in the brains of people with Alzheimer's, a disease that currently afflicts some six million Americans.
Positive data from the three experimental medicines could also provide an indication of future competition for Aduhelm, which was developed in partnership with Eisai and is currently the only drug that targets an underlying cause of the disease.
Large clinical trials of Aduhelm, known chemically as aducanumab, produced contradictory data, with one trial failing and another showing benefit. There was also a potentially serious brain swelling side effect.
Nevertheless, the FDA approved Aduhelm under its "accelerated approval" program with the understanding that Biogen would conduct a post-marking study to demonstrate patient benefit.
FDA officials said other Alzheimer's drugs will not automatically be eligible for that program. "We can't say right now whether this will be a path for other Alzheimer's drugs, or drugs for other neurodegenerative diseases," Dr. Patrizia Cavazzoni, director of the FDA's Center for Drug Evaluation and Research, told Reuters.
'PRECEDENT-SETTING'
Critics say the decision does change the landscape for future drugs.
"This is precedent-setting whether the FDA likes it or not," said Dr. Caleb Alexander, a Johns Hopkins public health professor and one of the remaining members of the FDA advisory panel that reviewed Aduhelm. Three members of the panel resigned after the FDA approval.
"That's not to suggest that the next drug that lowers amyloid is a slam dunk or even gets approved. It may not," he said.
For the near future, Biogen will have the market to itself, but analysts are watching potential future rivals closely.
"If another drug comes along and maybe doesn't have as many side effects, or maybe has slightly better data, Biogen's position could be jeopardized," said Raymond James health policy analyst Chris Meekins.
Japan's Eisai completed enrollment last month in a pivotal 18-month study of lecanemab in symptomatic early Alzheimer's patients. The drug is also being studied in a large trial of people with evidence of amyloid in their brains who do not yet have symptoms of the disease.
Roche, which has released limited gantenerumab trial findings, said it expects to have data next year from two global late-stage studies of its drug.
Eli Lilly announced encouraging results in March from a mid-stage study of donanemab and plans to conduct a larger trial.
"I think it is quite likely that if they can replicate those results it would be approved," said Dr. David Knopman, a neurologist at the Mayo Clinic in Rochester, who quit FDA's advisory panel in protest over the Aduhelm approval.
A Federal court in Tampa on Friday granted Florida a preliminary injunction against the Centers for Disease Control and Prevention’s (CDC) decision to prevent an immediate resumption of cruise operations.
The order will prevent the agency from enforcing against a cruise ship arriving in, within, or departing from Florida.
The lawsuit was filed in April by Republican Florida Attorney General Ashley Moody and the state had sought a quick lifting of a “nationwide lockdown” on the cruise industry that has been in place since March 2020.
Early in the pandemic, there were dangerous outbreaks of Covid-19 on several cruise ships.
“The federal government does not, nor should it ever, have the authority to single out and lock down an entire industry indefinitely,” Moody said.
Florida, viewed as a hub for cruise operators, said its ports have suffered a decline in operating revenue of almost $300 million since the pandemic started.
The injunction is stayed until July 18, after which time the CDC’s sailing order will only persist as a non-binding “consideration,” the order said.
The CDC was not immediately available for comment.
The order also allowed the agency to propose a “narrower” injunction by July 2 to allow cruise ships to sail timely and remain within the agency’s authority.
Taiwan will allow Taiwan Semiconductor Manufacturing Co. and Foxconn to buy 10 million doses of COVID vaccines on behalf of the government, as companies race to safeguard the island's flagship tech industry from the pandemic.
It is the first time private companies in Taiwan will be given permission to purchase vaccines, a move that comes as the government struggles to quickly inoculate people. The self-governing island, which was seen as a global role model for containing the deadly virus early on, has experienced a sudden surge in local infections since the middle of last month.
"Both TSMC and Foxconn's Yonglin Foundation proposed to donate 5 million [BioNtech] vaccine doses to Taiwan," government spokesperson Lo Ping-cheng told a news conference on Friday. BioNtech is a German pharmaceutical company.
To avoid "potential hurdles" they might encounter as private companies, the government will issue formal notices authorizing TSMC and Yonglin to negotiate with BioNtech on behalf of Taiwan to buy 5 million vaccines each, Lo said.
Foxconn's charitable foundation filed an application to import COVID vaccines on June 1, while TSMC applied on June 10, according to Lo.
TSMC confirmed to Nikkei Asia that it aims to buy 5 million BioNtech vaccines and donate them to the government, but said negotiations are ongoing. The efforts are directly being directly overseen by TSMC Chairman Mark Liu, Nikkei Asia has learned.
"The government thinks that it may be easier for companies to reach out to vaccine makers or distributors to lower the geopolitical interference," a source with direct knowledge of the matter said.
Foxconn Chairman Terry Gou said in a Facebook post Friday morning that he has been working to secure vaccines for Taiwan since May 23. He called on the government to authorize the Yonglin Foundation to negotiate with vaccine makers on behalf of the government, and to accept the vaccines as a donation.
The tech tycoon, who attempted to run for president in 2019, said he had no "political or commercial agenda" over the matter, and he called on President Tsai Ing-wen to meet with him.
"Although it is a seller's market when it comes to internationally approved vaccines, if President Tsai and the Taiwanese people are willing to let me use my several decades of international connections and business experience, I should be able to make a breakthrough" in buying the vaccines, Gou wrote.
The president's office said on Friday that Tsai will meet Mark Liu and Terry Gou that day at 4 p.m.
Taiwan has been gripped by a serious COVID outbreak since mid-May that has killed more than 450 people in less than a month. The rise in cases has also threatened to disrupt the round-the-clock production that many tech manufacturing plants rely on, which could further worsen the ongoing global chip shortage.
But Taiwan has struggled to secure vaccines due to geopolitical issues. China views the island as part of its territory, and Taiwan is not a formal member of the World Health Organization. President Tsai has accused China of interfering in her government's attempt to buy BioNtech vaccines, a claim that Beijing denies. Taiwanese Foreign Minister Joseph Wu said it is difficult for Taiwan to get enough vaccines from COVAX, a global COVID vaccine-sharing platform led by the WHO.
Japan recently donated 1.24 million AstraZeneca vaccines to Taiwan, while the U.S. said it will provide 750,000 jabs to the island. The doses from Japan are reserved for medical workers and citizens over 85 years old. As of Friday, only 1.32 million of the island's 23.5 million people had received at least one shot.
Taiwan, which has the world's largest semiconductor industry after the U.S., is one of the most important sources of advanced chips used in everything from smartphones and automobiles to data center servers and computers.
The pandemic has already caused disruptions to output. King Yuan, a leading chip testing and packaging service provider, was forced to suspend production for days after reporting the first cluster of infection in the chip industry. The cluster had expanded to more than 500 people as of Thursday, and included chip and networking companies in Miaoli County.
The two biggest Taiwanese companies -- Foxconn and TSMC-- are crucial suppliers in the tech supply chain and together account for more than 30% of the Taiwan Stock Exchange by market capitalization. Nikkei Asia earlier reported that at least five key tech companies, including multiple Apple suppliers, are considering buying vaccines to donate to Taiwan to help keep their operations running.
Nearly 15 months ago, a large, fast-moving and unscheduled experiment began: probing a key protein of the coronavirus SARS-CoV-2 to find chemical starting points for drug discovery. The end point was to develop pills that people could take to treat COVID-19 and related diseases.
This experiment pulled together a spontaneous, open, global, Twitter-fuelled collaboration called the COVID Moonshot. Urgency and a commitment to working openly recruited more than 150 active participants, spanning a huge range of expertise and technology across academia, biotechnology, pharmaceuticals and more, all working without claiming intellectual property. Open drug-discovery efforts are invariably super slow — ours has been an express train on tracks we have laid down as we go. It is a way of working that none of us realized was possible.
The intention for the original experiment was simply to help jump-start large drug-discovery initiatives that could draw directly on our data. In those first weeks, before the pandemic had taken hold in the United Kingdom or Israel (where the experiment started), we expected that some international effort was already in the works for countries and companies to collaborate on finding COVID-19 treatments, as was happening with vaccines.
Disappointingly, from the start of the COVID-19 fight, international funders decided to support only the development of repurposed small-molecule drugs and monoclonal antibodies to deliver treatments quickly, neglecting other approaches. The world seemed to give up on new antivirals before they even started, agreeing on a self-fulfilling prophesy that such drugs would take years to develop. Few seemed willing to contemplate such a timescale for this pandemic. Our first grant proposal was rejected, so we had to find a different way to press on.
Amazing virtual collaborations sprang up around the pandemic in many fields: bioinformaticians and phylogeneticists worked out ways to track new variants. Epidemiologists and computer modellers ran simulations. The World Health Organization activated a network of experts to vet new publications and preprints. Military personnel transported medical equipment and vaccines, and set up community testing centres.
Our COVID Moonshot is different. Rather than engaging with patients while using personal protective equipment, we work in chemistry hoods and with spectrometers, X-rays, computer models and courier companies. It’s driven by a conviction that conventional wisdom is wrong about de novo drug discovery being a job only for big pharma and peripheral to a fast-moving global outbreak: the pandemic is still here, and antiviral drugs against COVID-19 are not.
The screens
Drug-discovery efforts generally require a target, such as a protein that has an important role in disease. Promising drug compounds bind to the protein, affect its function and act safely in the body. Diamond Light Source near Oxford is the UK national synchrotron — a particle accelerator essential for modern X-ray crystallography, the go-to technique for determining 3D structures of proteins. There, one of us (F.v.D.) leads the XChem facility that uses the technique to screen for very small compounds called fragments that bind to drug targets. Although these ‘fragment hits’ bind weakly and the throughput is low compared with other techniques (screening fewer than 1,000 compounds per experiment), the 3D structures show exactly how each fragment binds. This provides powerful clues about how to create bigger, more potent molecules.
By late January 2020, scientists in China had solved the first 3D crystal structures of the SARS-CoV-2 main protease (Mpro), an essential viral enzyme, and made them public. With their guidance, a group at Diamond led by Martin Walsh generated new, high-quality crystals by mid-February — lightning fast for such work. The group also shipped Mpro protein to the Weizmann Institute of Science in Rehovot, Israel, where N.L.’s group uses mass spectrometry to quickly identify covalent fragments that attach to proteins irreversibly. This is another way to find useful starting points for drugs.
Racing to exploit the two weeks before a scheduled shutdown of the synchrotron on 6 March last year, more than a dozen scientists from the Walsh, F.v.D. and N.L. groups dropped everything to complete an XChem experiment four times the normal size1. All the data were analysed within one month, and as soon as we had the first batch of results, we posted downloadable data and a short write-up on the Diamond web page, then tweeted the link on 7 March.
The tweets
The response surprised us: almost 1,000 retweets in a week, and diverse offers for help. A.L. and M.R., two co-founders of the US–UK technology firm PostEra, got in touch to say that their machine-learning technology could propose synthetic routes to make new molecules inspired by the fragment hits. But first we needed drug-like molecules to be designed, and N.L. realized whom we could ask: medicinal chemists newly under lockdown restrictions, but full of expertise and desperate to help.
The next step was a tweet to crowdsource ideas for such molecules, declaring that we would make and test the best ones. A web page built by M.R. and his team in 48 hours enabled participants to submit machine-readable suggestions for compounds. The site made clear that contributions would have no strings attached, no intellectual property and no remuneration. We expected a few hundred submissions at most — in two weeks, we had more than 4,000, and had to work out how to test them.
The experiments
From March to May last year, we were on Zoom calls almost daily, lining up collaborators, logistics, expertise, funding, institutional support and permissions. All around us, the world was shutting down. We were trying to work out how to keep ourselves, our colleagues and our families sane, and our laboratories open.
We tapped an inexhaustible wellspring of goodwill. At the Ukrainian company Enamine, T.M. convinced management to commit to doing synthesis at cost, and to handle compound logistics. Its 650 chemists make molecules to order and have a renowned collection of building blocks for quick synthesis. By early May, new compounds were being shipped weekly from Enamine to organizations in four countries, and that work continues. Two other contract research organizations, WuXi in China and Sai Life Sciences in India, pitched in with offers of chemists and discounts.
Chris Schofield and his team at the University of Oxford, UK, together with Haim Barr and his colleagues at the Weizmann Institute, developed distinct biochemical assays that were key to cross-validating how well molecules inhibited the working Mpro enzyme. At the same time, for all compounds, the 3D mode of binding was assessed at Diamond in crystal structures. Half a dozen graduate students and postdocs suspended their own projects to coordinate, run and evaluate these assays, week after week. The work hasn’t stopped since.
By mid-April 2020, a volunteer troop of industry-based medicinal chemists, chaired by E.G., were holding weekly meetings to scrutinize submissions, review results, discuss strategies, design molecules and coordinate with synthetic chemists at Enamine. This work continues, too.
Computational chemists assembled their own team through their own network, then met weekly to work out algorithms to rank submissions. J.C. developed new ways to use Folding@home, the world’s largest crowdsourced supercomputer, which was already being used to generate models of viral proteins. It crunched ‘free energy’ calculations to predict the best binders for up to 10,000 compounds a week: 100 times more than had been attempted before.
Pharmaceutical companies develop elaborate information systems to track, store and analyse compounds and their associated data; our global effort urgently needed this, too. The informatics web platform CDD Vault donated us cloud space in its infrastructure just hours after a phone call, also arranging training and support. Many other vendors provided licences for free, and XChem’s platform for sharing 3D data, the Fragalysis cloud, had fortunately just been released. M.R. built a back-end system that sent all data live on GitHub, which is more often used as a repository for programming code.
As the pandemic unfolded, on some calls, you could hear the ambulance sirens from half a world away. The first agenda item of every meeting was a list of participants’ latest constraints — lockdowns, lab closures and home-schooling. Children made regular Zoom appearances, and at least two of us came down with COVID-19 ourselves. People pulled their weight not for glory or reward, but because there was a job that needed doing, and it was one that they could do.
To cells and live virus
By June 2020, the Zoom-based collaboration had identified sets of molecules that clearly inhibited a crucial viral protein. The next step was to test antiviral activity in living cells. These are complex experiments, requiring level-three biosafety labs certified for airborne pathogens.
A.v.D., a translational clinician, coordinated a shifting coalition of groups. One virologist friend and colleague lived a 10-minute walk away, and they planned experiments on lockdown evening strolls. Other virology groups responded to our tweet for help, and offered a variety of assays. Compounds were shipped, early results trickled in and some compounds unambiguously stalled the virus. These initial successes were crucial, both scientifically and for morale.
Researchers at the Israel Institute for Biological Research near Rehovot agreed to run a single test plate once we had molecules that were sufficiently potent. When that test showed signs of drug-like activity, they worked out how to conduct regular measurements, filling a crucial gap in our testing cascade.
By September, we had reached a milestone with a chemical series that instilled confidence: the compounds inhibited enzymes at submicromolar concentrations, and blocked viral activity at single-digit micromolar concentrations.
The slog
Since then, for the past nine months, the project has entered familiar territory in medicinal chemistry: we have been tweaking and testing compound designs, and optimizing early lead molecules so that they behave like drugs — entering the blood and staying there without being toxic. Potency against the Mpro enzyme has improved 100-fold, as has antiviral activity, and we are honing compounds’ solubility and rate of metabolism by the liver.
Above all, we can start predicting that these molecules will be straightforward to synthesize and will work as pills that are suitable for vaccine-hesitant or immunocompromised individuals, health-care workers and others in risky situations who could take them prophylactically. Furthermore, we expect them to work against vaccine-resistant variants: whereas vaccines target the spike protein on the virus capsule, our compounds target a conserved part of the virus machinery that works inside cells.
We’ve also had to deal with rejected grant proposals to advance antiviral drugs. Still, as vaccines have showed their dramatic successes, further variants have arrived and funders have begun calling urgently for antivirals and looking at how projects might be accelerated. In April this year, 16 months after the outbreak of SARS-CoV-2 in Wuhan, China, the United Kingdom finally launched a task force focusing on antivirals2.
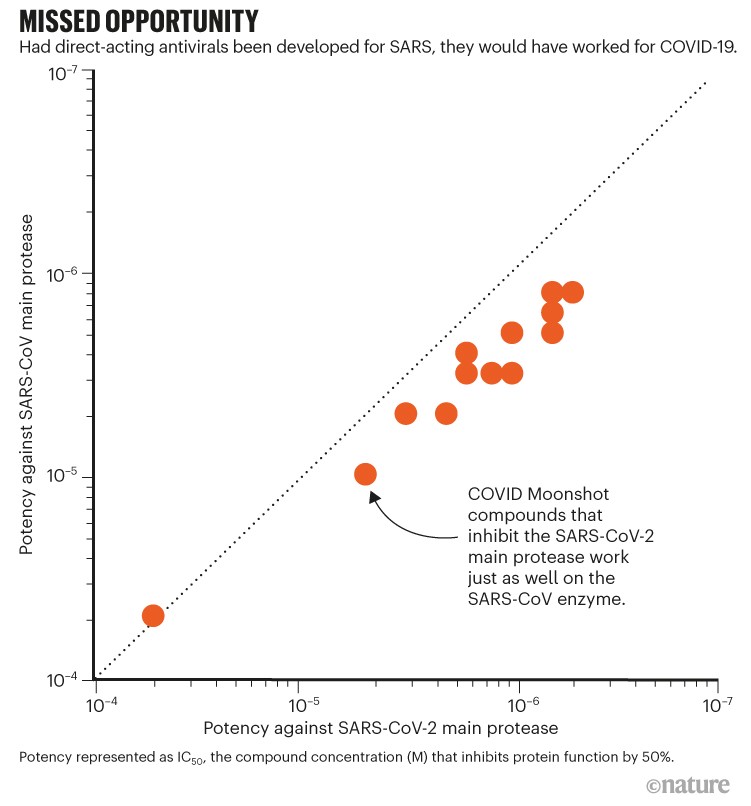
Pfizer’s March announcement of early clinical trials for its antiviral pill is confirmation that an accelerated approach can work, and that we should persevere. Our molecules also inhibit proteins of the coronavirus that causes severe acute respiratory syndrome (SARS; see ‘Missed opportunity’): had drug discovery persevered during the SARS epidemic in 2003, antiviral drugs would have been available when this pandemic hit. Above all, it has become much clearer how an antiviral would be most effective: the treatment must be readily available to everybody, long before they are hospitalized. Accordingly, we have been able to develop a clear plan for how to proceed, and the resources required.
Source: COVID Moonshot
We are approaching the capital-intensive, highly regulated phases of animal studies, producing kilograms of substance for clinical trials and, beyond that, worldwide manufacture and distribution of billions of pills. Our initial goal of delivering a drug straight from the discovery pipeline, free from patents and available for anyone to manufacture, cannot offer investors any conventional return on investment. Yet COVID-19 is not conventional, and vaccines have elevated the normally arcane question of intellectual property into a major political concern. Perhaps the COVID Moonshot can also shape how open drug discovery reaches patients.
The moral
So, what has made our approach work? Presumably, the fact that the mission was clear, even if distant, and the ethos was unambiguous and clearly signposted3,4. Initially, a few of us, fuelled by the urgency of the moment, acted on a conviction that our various combined technologies would accelerate drug discovery. We were soon joined by many people who did the hard work because they felt it was the right thing to do.
Also crucial was the existing large ecosystem of expertise and biopharma supply chains, coupled with new capabilities driven by long-term strategic investments in national infrastructure and research institutes. Tools for online collaboration have reached a critical mass, both general ones (such as Zoom or Google Docs) and those specific to drug discovery (in our case, CDD Vault). Serendipitously, for the segments of our project that had the most collaborators — such as submitting ideas for molecules — the requested contributions broke into discrete, doable tasks that easily accommodated each contributor’s availability and know-how.
The project self-selected a team of reflexively collaborative people, with no big egos. So far, we have avoided bureaucracy — no one claims to be the head of the COVID Moonshot. We retained momentum with collective trust, combined with sufficiently diverse expertise and perspectives, which allowed us to rapidly reach and implement strategic decisions. Reassuringly, people seemed to leave the collaboration only once their part of the project had been completed.
Perhaps the most surprising asset was that we did not have time to plan much at all — if we had, we’d have been paralysed. It seems you just have to get started and set deadlines for when to move on. Even now, we are astonished at how quickly this infrastructure self-assembled, just by scientists unabashedly asking for help from colleagues, distant connections or vendors. With so clear a goal, so obvious a need and the complete absence of contracts, people across the world stepped up.