Many hospitals and health systems have integrated diversity, equity and inclusion into their workforce and patient care strategies.
But now DEI is under scrutiny for both public and private organizations. President Donald Trump signed an executive order Jan. 20 to remove DEI from the federal government. Large companies are following suit; Google ended its DEI hiring goals and other DEI programs are being reviewed, according to The Wall Street Journal.
Amazon also slimmed down its diversity initiatives last year and Facebook disbanded its team overseeing diversity efforts. What will health systems do?
Many CEOs are keeping a close eye on new legislation and considering next steps. Providence, a 51-hospital system in Renton, Wash., is taking a thoughtful approach.
"As we do whenever new laws are enacted, Providence is carefully evaluating these executive orders to understand what it means for our patients, caregivers, physicians and communities. We are also well aware that legal challenges and legislative actions are common in the lawmaking process, so it's likely many of these new policies will continue to evolve," said a statement provided to Becker's.
Workforce inclusion
Providence reaffirmed its commitment to an inclusive work environment reflecting the diverse communities it serves and "ensuring every person has a chance to live their healthiest life, especially among health disparate populations."
"In addition, we will continue to be a safe, welcoming place of healing for everyone, including members of the LGBTQ+ community. We believe this is an important part of delivering high-quality patient care, with respect and compassion," the statement reads.
Providence isn't the only system leaning into a diverse workforce. USF Tampa General Physicians President Mark G. Moseley, MD, told Becker's Tampa General Hospital has a deep focus on belonging as a core cultural value.
"If you join our team, you have the right to belong and you matter to us regardless of any particulars about your own individual situation," he said. "As a team member, we will help you find connection to deep meaning and purpose in the work we do together. We prioritize our values and seek to have an intentional culture where we cultivate and encourage those values."
Leong Koh, MD, president and CEO of Northwest Permanente and co-lead of Kaiser Permanente National Health Equity Group took a similar stance.
"Across Permanente Medical Groups, we have an unwavering commitment to equity, inclusion and diversity in our workforce and in how we care for patients," he told Becker's. "Permanente Medicine was founded on the principle that healthcare should be accessible and affordable to all. Permanente Medical Groups are actively building on the principles of value-based care to advance health equity."
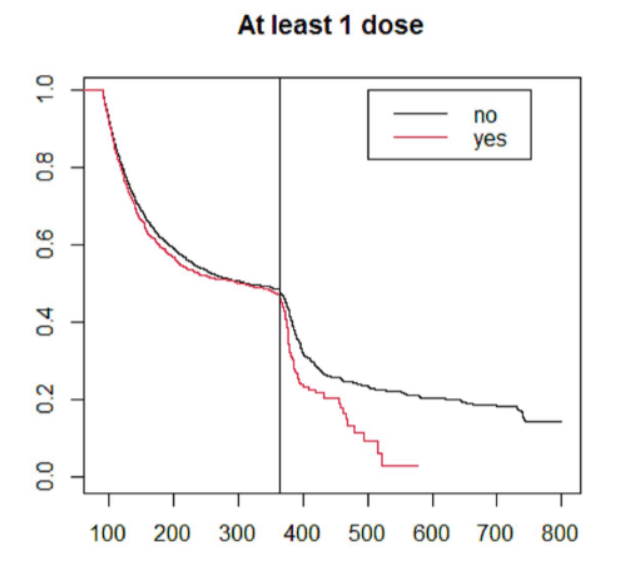
Northwestern Permanente also aims to build a workforce that is "as diverse or more diverse" than the patient population served to improve preventative care for all patients. Data published in the Journal for the American Medical Association Network Open showing Black residents had lower mortality rates in areas where there were more Black physicians than those in areas without Black physicians, validating the practice's strategy.
"The Permanente Medicine model was built on the premise of equitable care. That hasn't changed," he said. "As the country grows more diverse, the need for equitable, culturally responsive healthcare increases. Data consistently shows that when we focus on reducing disparities, public health improves. We are deeply committed to eliminating health disparities."
Sinai Chicago, a safety-net hospital, has built its workforce to reflect its own patient population, which is 90% Black and Latino. Sinai Chicago's workforce breakdown is 36% Black / African American, 28% Hispanic / Latino, 21% White and 12% Asian.
"Our caregivers are the heart and soul of Sinai Chicago," Ngozi Ezike, MD, President and CEO of Sinai Chicago, told Becker's. "We embrace the strength that lies in understanding diverse perspectives, encouraging the formation of Caregiver Resource Groups, and fostering a sense of cultural humility among our management. This translates into a high-performing, empathetic and culturally adept workforce."
Sinai Chicago actively recruits physicians and caregivers from the same communities as their patients, who can understand their backgrounds, speak the same language and share a common culture. The hospital also trains students, nurses, residents and others in cultural competency and fosters a passion and commitment to caring for the surrounding communities.
"With these initiatives and more, Sinai Chicago remains dedicated to celebrating the diversity that defines us and moves toward a future where prosperity and health are accessible to all and where respect, dignity and appreciation are the standard," said Dr. Ezike. "We're not changing our focus. This is part of our DNA at Sinai Chicago. A commitment to diversity, equity and inclusion has been a hallmark of our work since Mount Sinai Hospital opened its doors in 1919 to serve the Jewish immigrants who lived on Chicago's West Side. Over the years, the demographics of our population changed, but Sinai stayed focused on caring for immigrants and marginalized populations."
Albert L. Wright Jr., president and CEO of WVU Medicine West Virginia University in Charlottesville, said he'll continue to prioritize building a diverse, inclusive and skilled workforce to shape the system's culture and overcome complex issues.
"From a practical standpoint, the day-to-day reality of our workforce challenges requires us to cast a broad net in our recruitment efforts well outside our service area," he said. "Our home state cannot always meet our workforce needs in many critical areas; the homegrown numbers simply are not there to sustain our recruitment efforts."
Dr. Wright said the system has "hardwired" diversity and inclusiveness into daily routines, with the only litmus test being whether teams and caregivers do exceptional work.
"Culturally, we've built a health system that embraces diversity and recognizes it as a great asset, not a negative liability or a threat," Dr. Wright said. He later added, "We think fielding that A-Team of professionals requires having people who come from different backgrounds, experiences and beliefs. It's really that simple."
Dr. Ezike echoed this sentiment.
"Our collective goal needs to be creating healthier communities for all human beings, regardless of who they are, where they live or how much money they have," she said. "Healthcare's a fundamental human right, not a privilege."
Deborah Visconi, CEO of Bergen New Bridge Medical Center in Paramas, N.J., is taking a measured approach by recruiting diverse talent from the frontline staff to executive leadership with the goal of representing the community served, and advancing health equity.
"DEI is health equity, and these efforts must be both meaningful and measurable," she said, later noting, "I always say we are only as healthy as our least healthy community members. We use data to identify disparities in care and work with the community to close those gaps by strengthening public outreach programs and addressing the social determinants of health that impact patient outcomes."
Population-based projects
Kaiser Permanente, which includes 40 hospitals, 24,605 physicians and 12.5 million-member health plan, has a long history of population-based projects focused on health equity and value-based care.
"At The Permanente Medical Group, our dedicated physicians and clinicians strive to advance health equity and deliver culturally relevant care to all populations in our communities," said Maria Ansari, MD, FACC, CEO and executive director of The Permanente Medical Group, president and CEO of Mid-Atlantic Permanente Medical Group, and co-CEO of the Permanente Federation. "Our efforts helped Kaiser Permanente Northern California achieve five-star ratings in the category of 'Prevention and Equity' by the National Committee for Quality Assurance."
One example of The Permanente Medical Group's efforts is their colorectal cancer screening program, designed to eliminate racial disparities in screening and death rates between Black and White members. In 2009, the colorectal cancer death rate was 54.2 per 100,000 patients for Black members and 32.6 per 100,000 for White members.
"Through enhanced outreach, death rates fell by more than half among Black members by 2019," said Dr. Ansari. "This concerted effort and commitment saved lives."
Kaiser Permanente also launched the Kaiser Permanente Center for Black Health and Wellness in Portland, Ore., in 2023 to focus on reducing care disparities and improving outcomes for Black members while elevating the care experience and creating a culturally responsive environment to share across Kaiser Permanente.
Faith-based health systems also have a mission of providing care to diverse underserved populations. Cleveland, Ohio-based Sisters of Charity Health System has a 174 year history of providing care to those on the "fringes of society," according to CEO Michael Goar.
"As a Catholic organization committed to serving all God's people, we have worked closely with marginalized and vulnerable groups, fighting injustice that threatens the dignity of people, and cultivating an ethos of inclusion and belonging," he told Becker's. "The CSAs provided resources and developed ministries that served individuals of all colors, orphans, unwed mothers, alcoholics, AIDs victims and their families, those experiencing homelessness, victims of human trafficking, refugees and immigrants, struggling families, and children – all vulnerable populations."
His team is focused on healing the whole person, which includes providing opportunities for growth and fulfillment to all people.
"When systematic structures oppress marginalized groups, the CSAs and their collaborators have always spoken up to bring about just conditions for all people who may otherwise be overlooked and silenced," said Mr. Goar. "The CSAs have always embraced diversity and encourage important dialogue guided by the spirit of truth and wisdom. True to Catholic social teaching, we root our efforts and initiatives through the CSA lens of love, which is expressed in their motto, 'In all things charity' and in the core values that shape our family of ministries and programs, located in Cleveland, Canton, Ohio, and throughout the state of South Carolina."
The executive orders and move away from DEI in other sectors won't affect Sisters of Charity's approach to care, Mr. Goar said.
"We are remaining steadfast to our mission of honoring and serving all people, regardless of race, income, religion, or social and economic status. We recognize the dignity of all people and are working to especially serve the neediest among us," he said.
Victorville, Calif.-based Desert Valley Medical Group CEO Marie Langley is similarly elevating the group's mission of accessible, compassionate and effective healthcare for all community members. She pushed back on the notion that DEI efforts hinder the organization.
"Diversity, equity and inclusion are naturally embedded in this mission, not as barriers or bureaucratic hurdles, but as guiding principles helping us meet the unique news of our diverse patient population," said Ms. Langley. "Healthcare is, at its core, about treating individuals and communities. While policies and regulations evolve, our focus remains on delivering the best care to our patients."
Compliance vs. community
As federal and state regulations change, C-suites are working with their boards and legislators to ensure they're able to carry out their mission. Dr. Ezike said she and her team are watching the new administration closely to see how it defines healthcare priorities, but will remain focused on advancing health opportunities for the community and addressing long-term health disparities.
"We will continue working with local, state and federal leaders to advocate on health equity. This mission is more important than ever," she said. "Our mission of service to our community remains the same. The fact is, we look like the community we serve – we are that community. Many of our patients and our caregivers are immigrants. Many of our caregivers were born, raised and live in our community. And we believe that all should feel safe, respected and valued in our community – our employees and trainees, our patients and our neighbors."
Bergen New Bridge is moving forward with its health equity work and preparing for the possibility of lost funding. The hospital recently expanded clinical and non-clinical team training for cultural awareness, implicit bias education, and best practices for equitable treatment and outcomes to boost patient care.
"The recent executive orders have sparked conversations regarding funding, compliance, and long-term sustainability," said Ms. Visconi. "While we are mindful of potential shifts in policy, our approach remains focused on what is best for our patients, residents and our team members. We are evaluating how these policies may affect grant funding, reimbursement models and other financial considerations. However, we are also working with community partners and private organizations to ensure key programs fundamental to our mission continue, regardless of federal policy shifts."
And Bergen New Bridge will keep its commitment to inclusion, too.
"Compliance is important, but our equity efforts are about doing the right thing for our patients, residents and employees. Regardless of political changes, we remain committed to fostering a workplace where everyone feels valued and safe while ensuring every patient receives care that is respectful and responsive to their needs. At the end of the day, we remain dedicated to providing exceptional, accessible, and equitable healthcare to our community. That is simply good, responsible healthcare," said Ms. Visconi.
Ms. Langley sent a similarly strong message about Desert Valley Medical Group's DEI plans amid the executive orders: the team will continue to prioritize patient care.
"While we continuously assess and refine our practices to align with regulatory requirements, we do so with the singular goal of enhancing patient outcomes and experiences," she said. "Our commitment to compassionate, evidence-based care will always be the foundation of how we operate, regardless of external changes."
https://www.beckershospitalreview.com/health-equity/what-happens-next-to-dei-at-health-systems.html