The Biden administration may have failed to convince Congress to double Medicaid spending on home healthcare in 2021, but the funding increase occurred anyway.
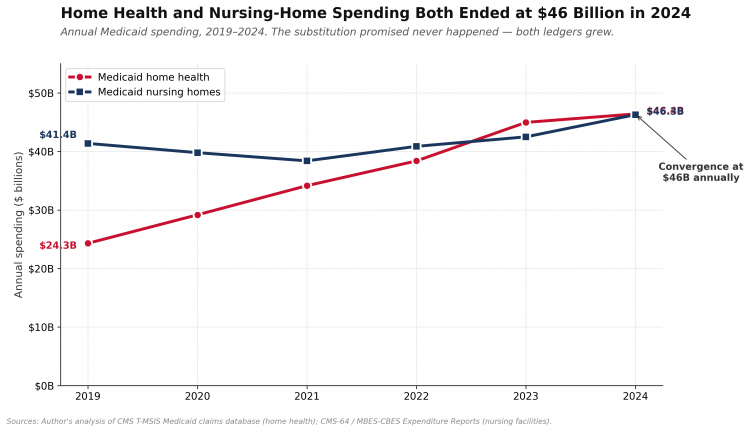
An RCI analysis of federal data has found that spending on the program, which pays health aides and family members to act as caregivers for elderly and disabled adults, nearly doubled between 2019 and 2024, to $46.4 billion a year – an amount nearly identical to the $50 billion per year Biden wanted. As a result, American taxpayers paid more than $217 billion for home-based care under the program during that five-year span.
Lacking congressional approval, policymakers simply moved the initiative out of Washington and down to the state Medicaid agencies.
Although the expansion was promoted as a way to reduce reliance on more expensive nursing homes, federal data show that did not happen. Medicaid spending on nursing facilities rose by nearly $5 billion in the same five years, to $46.3 billion. In addition, the sprawling home care program has become the subject of a growing set of fraud probes and prosecutions involving the billing codes at the center of the new spending.
The data suggest that the complex landscape of healthcare offers myriad ways for states and providers to access large amounts of federal funding.
Promises
The spending boom traces back to a March 2021 White House proposal. As part of its American Jobs Plan, the Biden administration called for $400 billion in new federal spending over eight years to expand home and community-based care under Medicaid. “President Biden believes more people should have the opportunity to receive care at home, in a supportive community, or from a loved one,” the White House said in its rollout.
Advocacy groups had long sought a vast expansion of home care. AARP told policymakers that home- and community-based services would “prevent or delay frail seniors and persons with disabilities from being admitted to nursing homes,” and that the cost would be a fraction of facility-based care – about $1,300 per person per year for community support against $25,000 to $37,000 per year for a Medicaid nursing-home bed. Justice in Aging, a national legal advocacy organization focused on older adults, said nursing home care was four times more expensive than community-based services and that older adults without home-care access were five times more likely to enter a nursing home.
The federal government put a number on the projected savings. The Department of Health and Human Services’ Office of the Assistant Secretary for Planning and Evaluation projected that for every additional dollar Medicaid spent on home care, nursing-home spending would drop by about 26 cents. Those were the figures used to make the case to Congress and to the public.
Justice for Aging and the Department of Health and Human Services did not respond to requests for comment.
Congress Unconvinced
President Joe Biden's proposal for a vast expansion of home care was never passed by Congress but the funding flowed anyway.
AP
Congress was not convinced. The home-care expansion was cut to $150 billion in the Build Back Better Act, which did not win passage and then dropped entirely from the Inflation Reduction Act, which Biden signed into law in 2022.
Much of the money was spent anyway. When federal legislation stalled, the mechanism for delivering funding shifted from Congress to state Medicaid agencies. The Centers for Medicare and Medicaid Services worked with state programs to expand existing waivers, raise reimbursement rates paid to home-care providers, and build out programs that pay family members to act as caregivers. States that wanted to grow their spending pulled the regulatory levers they already had. States that hesitated were offered federal matching dollars, technical assistance, and a steady drumbeat of CMS guidance encouraging them to expand.
By 2024, Medicaid spending on the home-health bundle – personal-care services, home health aides, skilled nursing in the home, and the related billing codes that capture the bulk of the dollars – was $22 billion higher per year than in 2019. That increase amounted to roughly 44% of the annual expansion the Biden White House had originally sought from Congress, achieved without Congress ever approving the program.
Blue State Windfall
Most of the dollars were accessed by Democratic-controlled states. New York alone reached $15.67 billion in Medicaid home-health spending by 2024 – roughly a third of the national total – through its Consumer Directed Personal Assistance Program, which allows beneficiaries to hire a relative as the paid caregiver. Massachusetts, New Jersey, Illinois, California, and Pennsylvania all rank in the top tier of absolute spending growth. Pennsylvania’s home-health bill grew more than twelvefold over five years.
The fastest percentage growth between 2019 and 2024 came in Republican-controlled states with smaller base programs. Texas grew its Medicaid home-health spending by 330%. Arkansas grew by 352%. Alabama, 250%. Spending rose in every state in the union.
These numbers may grow due to lengthening waiting lists for people seeking home-care services. According to a Kaiser Family Foundation analysis of state Medicaid agency data, the number of Americans on waiting lists for Medicaid home- and community-based services has risen rather than fallen since 2019, despite the $217 billion expansion. Advocates say this is a reflection of the growing need for such services.
As the home-care proponents predicted, the number of Medicaid beneficiaries actually living in nursing homes did fall during the five-year period. Unique Medicaid nursing home users went from 1.57 million in 2019 to 1.29 million in 2023, a 17.7% decline. Most of the drop happened during the pandemic, when COVID-19 swept through nursing facilities and prompted admissions freezes at many homes in 2020 and 2021. Since 2021, the Medicaid nursing home population has been climbing again.
Rising Prices
But this did not produce savings, as states sharply increased the rates they paid to facilities. Medicaid spending on nursing homes grew from $41.4 billion in 2019 to $46.3 billion in 2024. The cost per resident per day at Medicaid-certified nursing facilities climbed from $313.66 in 2019 to $401.98 in 2024, a 28% increase.
The same dynamic occurred with reimbursements for home care. State Medicaid agencies raised home-care reimbursement rates sharply during and after the pandemic – 15% to 30% in many states – and most of those increases were never rolled back.
The official justification was a workforce shortage. The claims-level data show a different pattern. While Medicaid spending on home health grew 91% over five years, the number of providers billing Medicaid for these services barely grew, and the number of unique beneficiaries grew only modestly. What climbed each year was the price per claim and the price per beneficiary.
The larger share bought expanded eligibility – programs designed to enroll people who would not otherwise have entered a nursing home. The clearest example is New York’s Consumer Directed Personal Assistance Program, which allows the Medicaid beneficiary to hire a relative as the paid caregiver. According to a claims-level analysis of CMS Transformed Medicaid Statistical Information System (T-MSIS) data, the New York program grew from a niche state option into the single largest line item in Medicaid home-care spending nationally.
The total number of people involved in the program is hard to discern because federal claims data do not separate individual family caregivers from agency providers. In a self-directed Medicaid program such as home-care, the beneficiary – not an agency – picks and hires the caregiver, and the state pays that caregiver directly. The caregiver is most often a family member, a friend, or a neighbor. In states with large self-directed programs, the count of paid family caregivers is likely to be in the tens of thousands of individuals. State enrollment standards for self-directed and family caregivers were also relaxed during the pandemic, with documentation requirements reduced and licensing barriers lowered to expand the workforce.
Fraud Magnet
The expansion has become a documented vehicle for fraud. The U.S. Department of Justice and the HHS Office of Inspector General have brought a growing number of prosecutions involving the T1019 personal-care billing code – including fraudulent hours never worked, billing for deceased beneficiaries, and family-member billing schemes in which the care was either never delivered or was billed at a fraction of the claimed hours.
In December 2024, Pennsylvania Attorney General Michelle Henry announced charges against a suburban Philadelphia home-care agency, its owner, and 18 other people in a scheme that allegedly defrauded the state’s Medicaid program out of millions of dollars. The Department of Justice’s Health Care Fraud Unit listed multiple home-health prosecutions in its 2025 national case summaries.
Vice President JD Vance said he's directing the Federal Fraud Task Force to examine home-care spending.
AP
The Daily Wire’s recent investigation of Ohio’s multi-billion-dollar home-care industry found a lack of oversight. “Since the services are performed inside private residences, there is no way to know whether the workers went at all, or what they’re actually doing in exchange for taxpayer funds,” Luke Rosiak reported. “An infinite number of small black boxes inside a black box. Multiple signs said the service provided, and billed to the government, was sometimes just ‘companionship & conversation.’”
Even as Ohio says it has ongoing probes into its home-care spending and Vice President JD Vance announced he’s directing the federal Fraud Task Force he heads to examine the Buckeye State, RCI’s analysis suggests a deeper problem – the extent to which massive federal dollars can flow without congressional approval.
Budget hawks say fraud must be addressed, but even that does not address the underlying mechanisms – massive funding with relatively little oversight – that invite runaway spending and abuse. The recent history of home-care funding also highlights the often false premises on which many government programs are sold to the American people.
Walter Curt is a Senior Fellow at Restoration of America and the founder of The W.C. Dispatch. Follow him on X at @wcdispatch and at wcdispatch.com.
https://www.realclearinvestigations.com/articles/2026/05/14/unbridled_spending_billions_for_medicaid_program_congress_never_approved_1182576.html?mc_cid=c84364dbbc&mc_eid=0622ebfa37