Robert and Karen Bonta, married 50 years last summer, explored all seven continents as they charged into their 70s.
So Amy Bonta Ferin didn’t worry about her parents each winter when they left their chilly Iowa home for the saguaro-dotted desert hills near Phoenix. Her mother, Ferin said, who also kept a bag packed to travel to events involving her three children and 10 grandchildren, lit up a room with her hopeful, smiling face.
“One of the hardest things to see was her in a casket,” Ferin said. “She didn’t have a smile on her face.”
A Ford Explorer driven by 27-year-old Alex Bradshaw hopped a curb and hit them as they stood on a sidewalk. Canadians Patti Lou and Ronald Doornbos, both 60, were also struck by the SUV as they walked toward the corner in a marked crosswalk. Patti Lou died immediately;
Ronald died June 12.
The four deaths highlight a growing danger for America’s most vulnerable road users: Death by SUV.
The scene after a Ford Explorer jumped a curb, striking four people in Fountain Hills, Arizona, on March 13. Three people were killed and another…Show more
ROBERT GUNDRAN
A Detroit Free Press/USA TODAY NETWORK investigation found that the
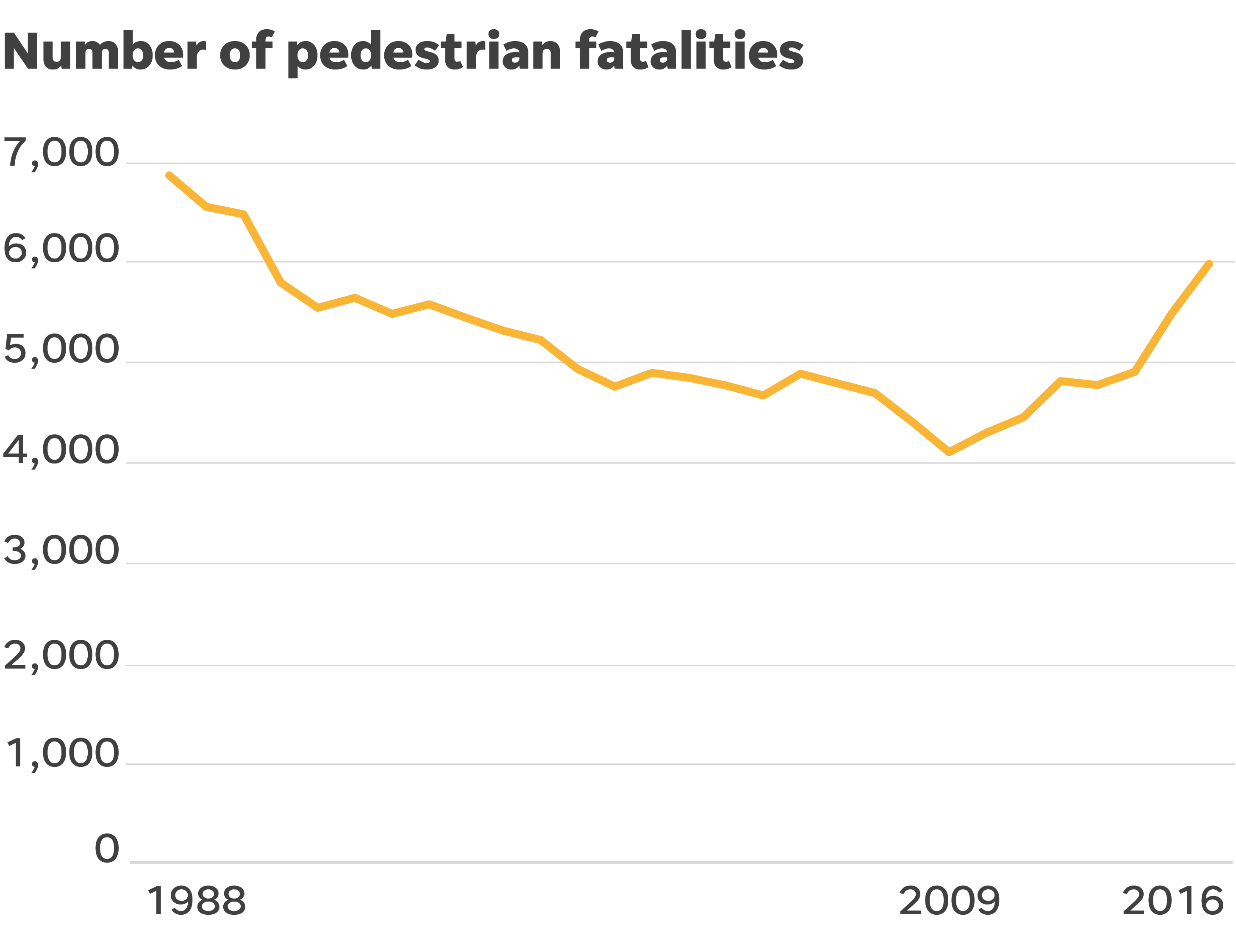
SUV revolution is a key, leading cause of escalating pedestrian deaths nationwide, which are
up 46 percent since 2009.
Almost 6,000 pedestrians died on or along U.S. roads in 2016 alone — nearly as many Americans as have died in combat in Iraq and Afghanistan since 2002. Data analyses by the Free Press/USA TODAY and others show that SUVs are the constant in the increase and account for a steadily growing proportion of deaths.
Our investigation found:
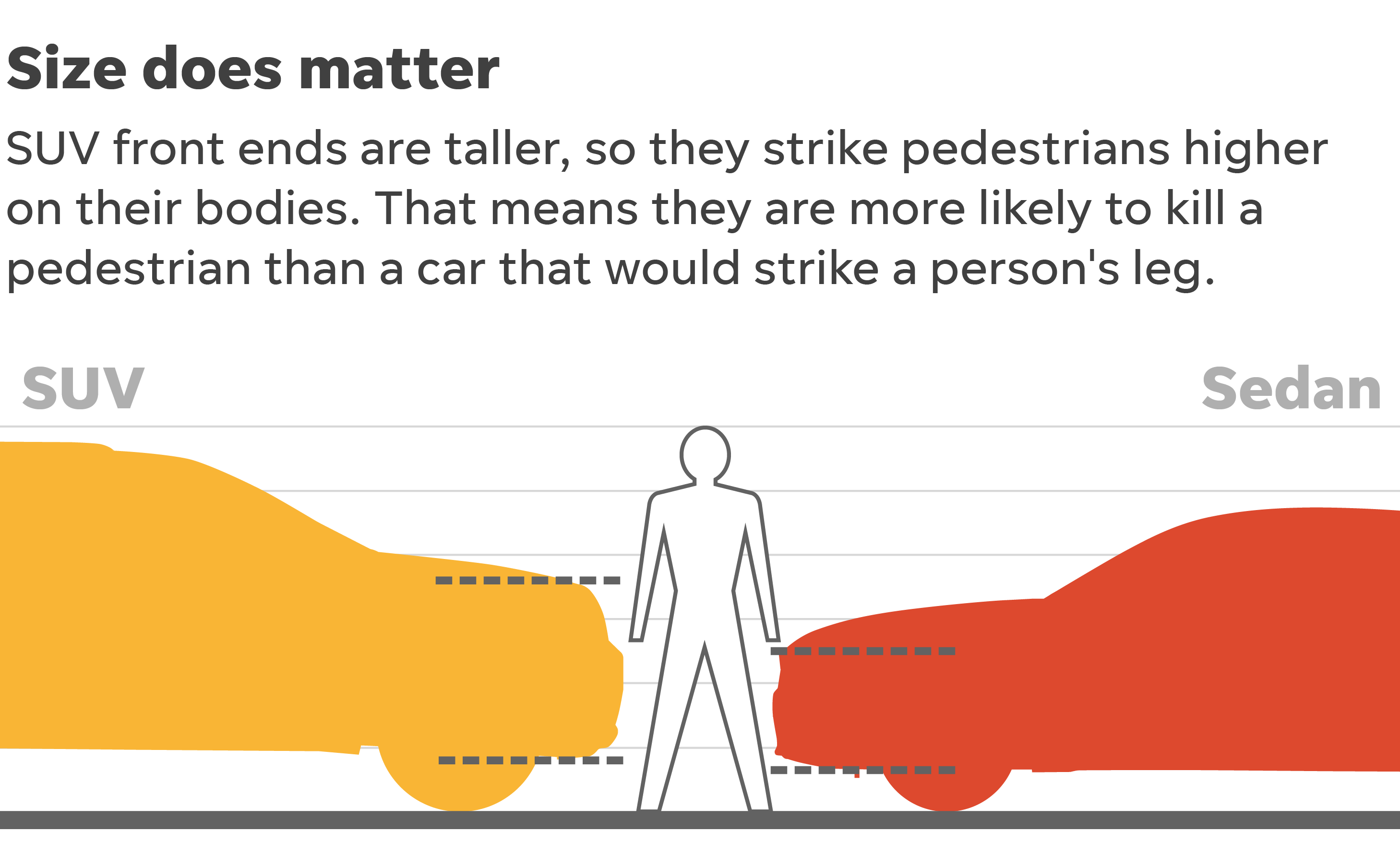
- Federal safety regulators have known for years that SUVs, with their higher front-end profile, are at least twice as likely as cars to kill the walkers, joggers and children they hit, yet have done little to reduce deaths or publicize the danger.
- A federal proposal to factor pedestrians into vehicle safety ratings has stalled, with opposition from some automakers.
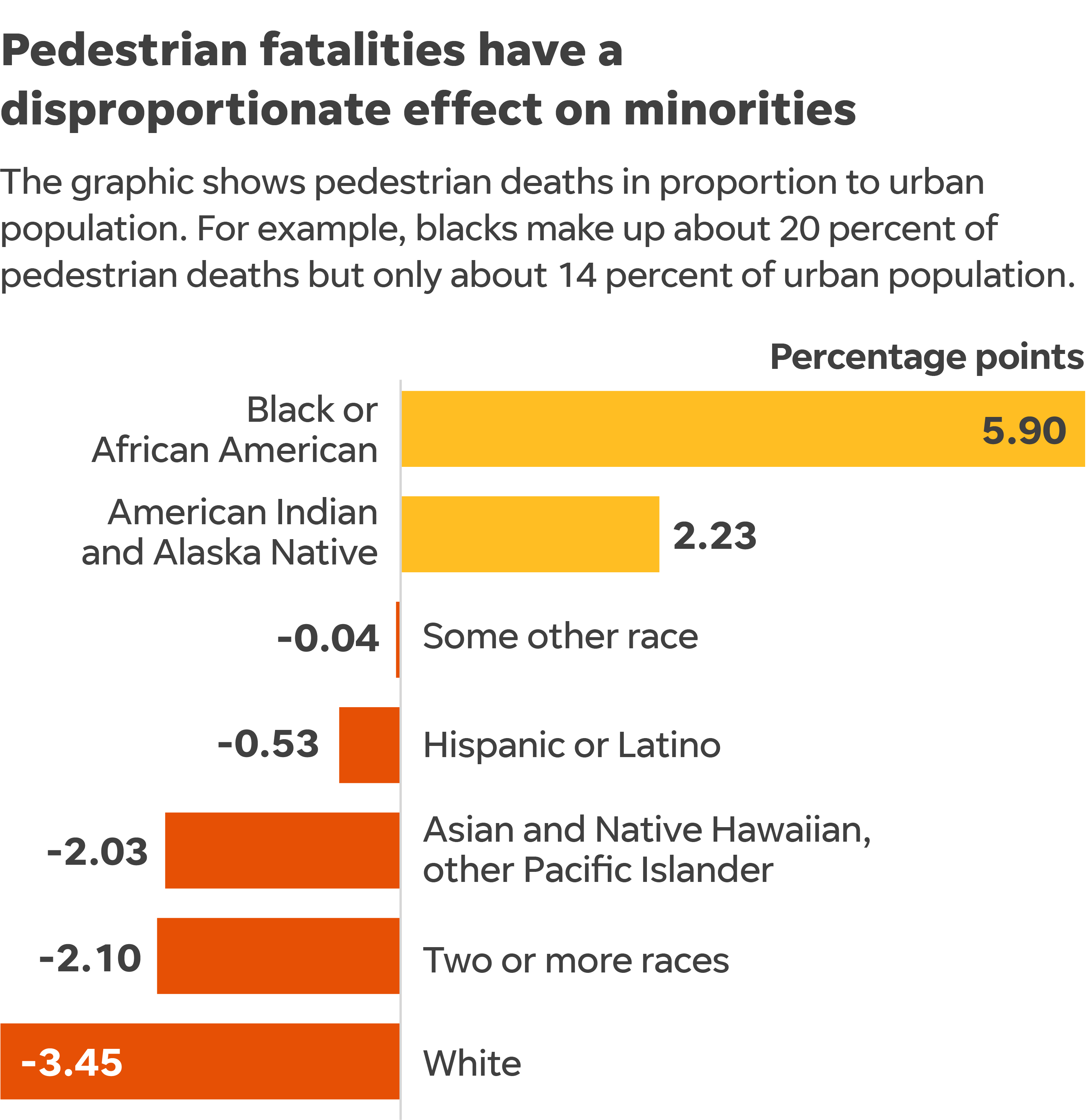
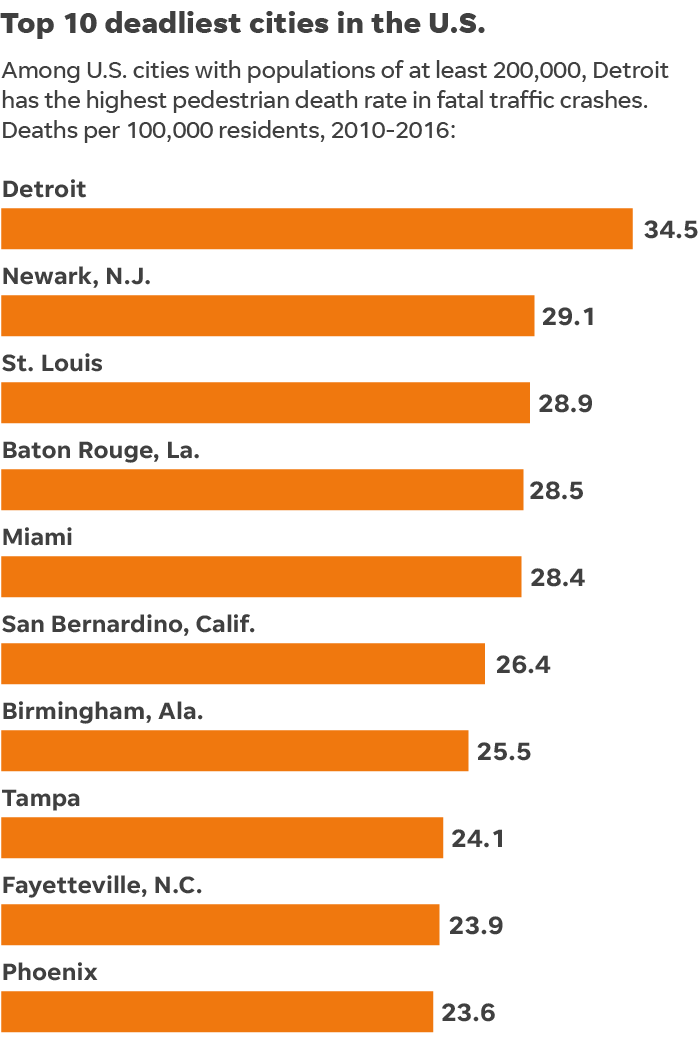
- The rising tide of pedestrian deaths is primarily an urban plague that kills minorities at a disproportionate rate.
- It is most prominent in cities both in the industrial heartland and warm-weather spots on the nation’s coasts and Sun Belt. Detroit; Newark, New Jersey; St. Louis; Baton Rouge, Louisiana; Miami, San Bernardino, California, Birmingham, Alabama; Tampa; Fayetteville, North Carolina; and Phoenix had the 10 highest per-capita death rates among cities with populations of at least 200,000 in 2009-16.
Vehicle safety measures, which the federal government says could save hundreds of pedestrian lives every year, are available but not widely employed by some automakers — nor are they required.
Along with automakers, cities can take action that saves pedestrians. New York City, for example, cut such deaths nearly in half in just four years. The need for steps such as lower speed limits, more midblock crosswalks and better lighting grows in urgency as automakers move strongly toward truck and SUV production.
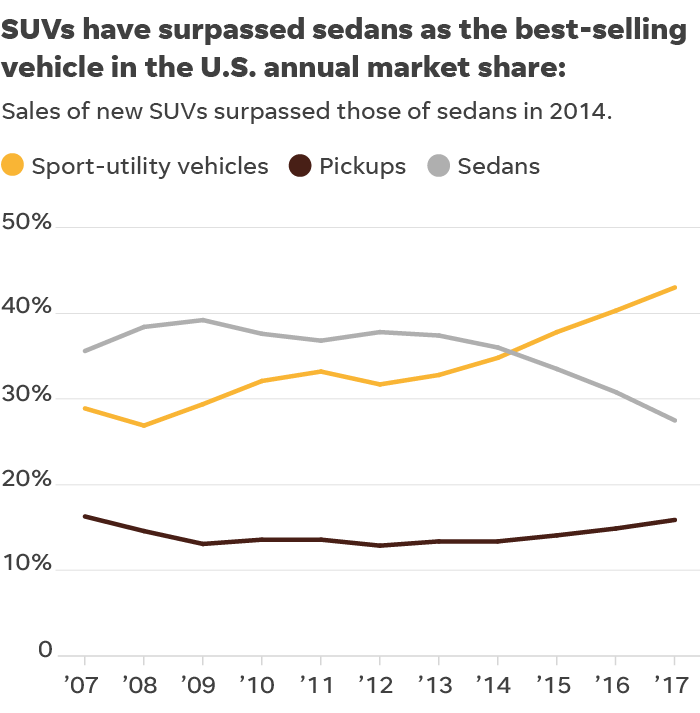
SUV sales topped sedans in 2014; pickups and SUVs now account for 60 percent of new vehicle sales.
Ford recently announced plans to discontinue U.S. sales of most passenger cars, while
Fiat Chrysler has already done so.
Distraction and other factors
It might seem obvious that a larger vehicle can cause more damage in a crash, whether to a smaller car or an unprotected skull, but some researchers have been hesitant to assign blame for the spike in pedestrian deaths to America’s love of SUVs, in part because various factors are at play in every crash.
Each of the 5,987 pedestrians who died in 2016, according to federal data, had his or her own tragic ending.
Many who died were males, were jaywalking or had alcohol in their systems on multilane roads in urban areas at night.
Some might have been distracted, just as vehicle drivers could have been, by texting or talking on cellphones, although data is lacking to quantify distraction.
Some of these other factors also saw increases in recent years, but the SUV component stands out.
Data and safety experts verified that long-standing common factors in pedestrian deaths, such as alcohol and jaywalking at night, did not account for the growth.
A key factor consistently backed by data is growing involvement of higher-profile, blunt-nosed SUVs.
The Insurance Institute for Highway Safety calculated an 81 percent increase in single-vehicle pedestrian fatalities involving SUVs in 2009-16. The Free Press/USA TODAY analysis of the same federal data, counting vehicles that struck and killed pedestrians rather than the number of people killed, showed a 69 percent increase in SUV involvement. The assessment also showed increases each year in the proportion of fatal pedestrian crashes involving the popular vehicles.
Safety standards stalled
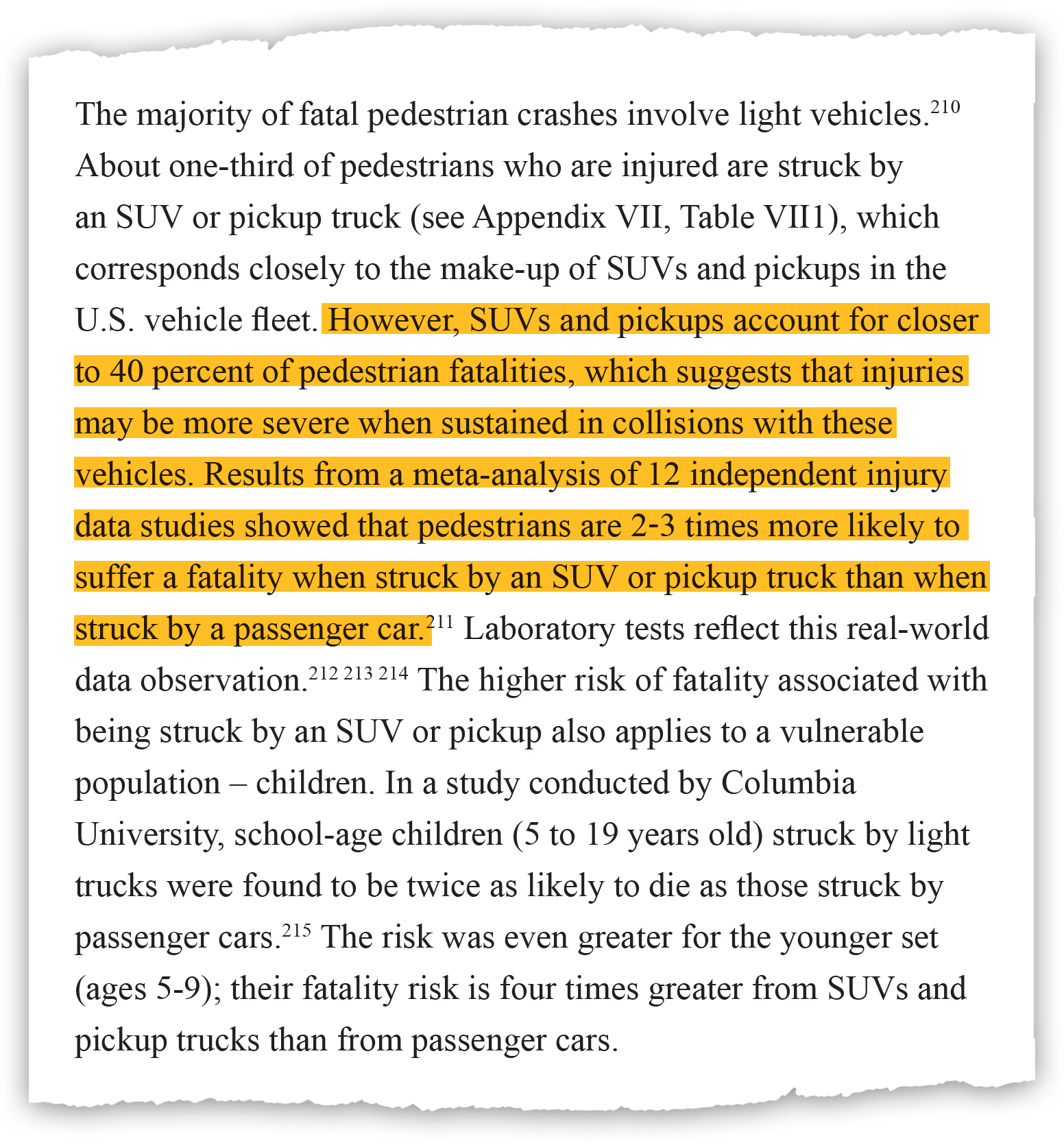
The National Highway Traffic Safety Administration made the connection in 2015 that SUVs were deadlier for pedestrians than cars, referenced on page 90 of a 195-page report. That report, citing 12 independent studies of injury data, said pedestrians are two to three times “more likely to suffer a fatality when struck by an SUV or pickup than when struck by a passenger car.”
That report also noted that SUVs and trucks were involved in a third of pedestrian injuries but 40 percent of deaths, indicating that injuries “may be more severe when sustained in collisions with these vehicles.” The proportion of SUVs on the road has only grown in the three years since.
NHTSA, citing the findings in December 2015, announced a plan to overhaul its vehicle-safety rating system to include a new score for pedestrian safety. The plan was to roll out an overhauled New Car Assessment Program, or NCAP, in 2018 for 2019 model-year vehicles.
But that hasn’t happened.
NHTSA did not respond to questions about what caused the delay, although the agency has been without a permanent administrator since President Donald Trump took office. In a statement to the Free Press this week, the agency said it is “working on a proposal for a standard that would require protection against head and leg injuries for pedestrians impacted by the front end of vehicles.”
The agency noted that it is studying interactions between motorists, pedestrians and bicyclists, distractions, and strategies that states can use to protect pedestrians and improve education on “this important topic.”
NHTSA said earlier that it “plans to continue our efforts to update NCAP by following our process for public engagement, including a public meeting during summer 2018.”
That meeting has not been scheduled and the SUV finding has not been widely shared. The Governors Highway Safety Association earlier this year, for example, reported on its
estimates of pedestrian deaths in 2017 and did not cite SUVs as a factor, even speculating that legal marijuana has played a role.
A known factor
As early as 2001, researchers at Rowan University in New Jersey predicted a deadly trend that would reverse a historic drop in pedestrian fatalities, which are now the highest they have been since the George H.W. Bush presidency.
“In the United States, passenger vehicles are shifting from a fleet populated primarily by cars to a fleet dominated by light trucks and vans,” according to their research paper, referencing “light trucks,” which includes SUVs. “Because light trucks are heavier, stiffer and geometrically more blunt than passenger cars, they pose a dramatically different type of threat to pedestrians.”
Hampton Clay Gabler, a professor in the department of biomedical engineering and mechanics at Virginia Tech, wrote that paper with Devon Lefler. Gabler’s interest in the pedestrian issue came from research in other areas showing high death rates for those in cars struck by SUVs.
He described the vulnerability of pedestrians when struck by an SUV as a geometry problem of sorts because SUVs and pickups tend to be tall compared with pedestrians and have a blunter front end. That positioning is more likely to put someone’s head or chest in line to be struck during the initial impact with a vehicle.
“(Not to diminish leg injuries but) serious head and chest injuries can actually kill you,” Gabler said in a telephone interview.
More power
Size and profile are not the only vehicle factors involved in the increased fatalities. Power also increased. A report by the Insurance Institute noted that the trend toward more powerful vehicles could contribute to higher speeds, which, in turn, could lead to more crashes and more severe injuries.
“The increasing popularity of SUVs and higher vehicle speeds associated with more powerful vehicles could have contributed to how crashes involving pedestrians have become deadlier,” the study said.
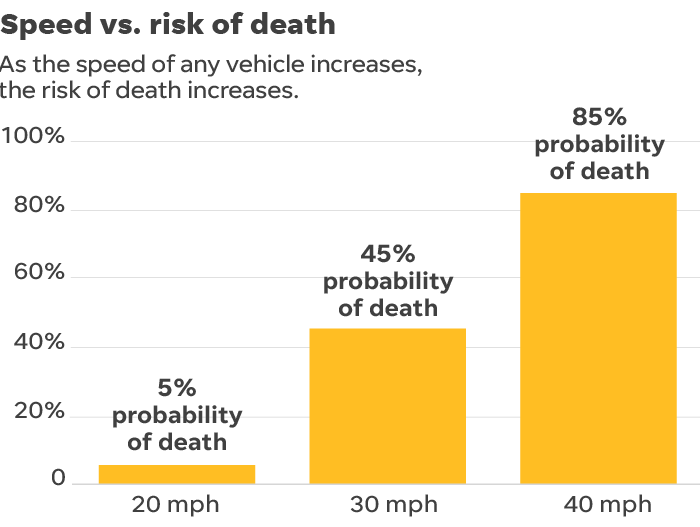
And speed can clearly kill.
At crashes where a vehicle is traveling 20 mph, 5 percent of pedestrians die. At 30 mph, the percentage increases to 45 percent. At 40 mph, the percentage skyrockets to 85 percent, according to research from 1995 cited by the European Commission, an arm of the European Union.
“Speeding is the most important determinant of whether a pedestrian dies in a crash,” said John Wetmore, a national pedestrian advocate who hosts the public access program “Perils for Pedestrians.”
That belief is supported by Dr. Joe Patton, division head of trauma and acute care surgery at Henry Ford Hospital in Detroit, a doctor on the front lines of treatment for those injured in crashes.
“Speeding is the most important determinant of whether a pedestrian dies in a crash.
John Wetmore, national pedestrian advocate
“Certainly, big cars going fast are worse than little cars going fast, but the speed has a lot to do with it,” Patton said. “I really think the speed makes more of an impact than the size of the vehicle, so you’d rather get hit by a big car going real slow than a small car going real fast because the velocity and the energy of that velocity that it imparts on the person they hit probably plays a bigger role than the size of the car but certainly people are driving bigger cars now.”
Patton called it “intuitive” that bigger vehicles cause worse injuries.
Overall traffic fatalities drop
Pedestrians deaths are not a new phenomenon.
The toll that automobiles have taken on pedestrians dates to the beginnings of the automotive age. In 1896, Britain saw its first pedestrian death by a motor vehicle when a woman was struck in south London. That same year, the country raised its speed limit from 4 to 14 mph, according to Steve Parissien’s “The Life of the Automobile.”
The first U.S. pedestrian death by automobile came in 1899 when a man was struck and killed in New York after hopping off a trolley, Parissien noted.
The more than 8,000 pedestrians killed in the United States in 1979 represent a high point, according to the Insurance Institute, but more than 51,000 people died in motor vehicle crashes that year. Motor vehicle crash deaths had fallen to 37,461 in 2016, according to NHTSA data, as vehicle safety improved.
Pedestrians are not seeing the benefits of the lifesaving safety improvements that have helped reduce total traffic fatalities. Pedestrians represent 16 percent of those killed in traffic crashes in 2016, a steady increase over the past decade.
Those who die, however, are not simply statistics.
In Memphis, 70-year-old Lee Soult was one of eight pedestrians killed so far this year. Soult was struck by a pickup and killed as he crossed a city street outside a crosswalk on an April evening. His brother, Bob Soult, mourned the fact that Lee, who retired from a glove company in 2013, would not “get to enjoy his retirement and his life a little while longer.” The truck driver was not charged in the crash.
In Detroit, the 2016 death of 64-year-old Maurice Parker Mims prompted a campaign to track down the hit-and-run driver of a Chevrolet Impala, which struck Mims in a crosswalk on Veterans Day, authorities said. Mims, a Marine veteran and street artist in Detroit’s Greektown neighborhood, had been picked as metro Detroit’s “Most Outstanding Volunteer” by the American Red Cross.
Gilberto Ramon Ortiz, 23, was accused of taking the car to a repair shop to have the windshield replaced after the crash, according to the Wayne County Prosecutor’s Office. A jury trial on charges of tampering with evidence and obstruction of justice is scheduled for July.
Robert Bonta, 72, and Karen Bonta, 71, were avid travelers and visited every continent. The Iowa couple was killed in a crash in Fountain Hills,…Show more
AMY BONTA FERIN
Back in Phoenix, Karen Bonta died at the scene of the March crash. Her husband, Robert, died 61 minutes later at an area hospital.
Ronald Doornbos, whose wife was killed, died this month in Calgary, where his family said he had been “minimally conscious.”
The crash on a multilane road with a 35-mph speed limit came during a deadly stretch this spring for pedestrians in the nation’s fifth-largest metro area, with 10 people dying in nine days.
Authorities have said Bradshaw, the driver, didn’t appear to be impaired. They have not disclosed how fast they think he was driving, but whether he was distracted remains part of the investigation.
Tim Budnick, a business owner near where the crash happened, said he heard tires squealing and noise he thought was the SUV ramming into a concrete curb. When he walked outside, he learned the sound was actually the vehicle hitting people.
“When I saw them, I was expecting some of them to start getting up, saying things like ‘Oh, my wrist,’ or ‘My shoulder hurts,’ ” Budnick said. “I heard nothing. All four of them were lying there.”
Known safety measures
As the number of pedestrian fatalities has spiked, some communities have worked to change the narrative.
Pedestrian safety advocates have pointed to efforts like those in New York as examples for other cities. Through a combination of enforcement targeted at driver behavior, lowered speed limits and training for cab drivers, the city saw its pedestrian deaths last year drop to their lowest number, 101, since the city began tracking the statistic in 1910.
In Seattle, Rainier Avenue in 2015 was reduced from four lanes to three, enforcement was stepped up and other changes made it easier for pedestrians to cross. Eleven people died between 2004 and 2014 on one portion of the road, but no one has died in that section since the changes were made, according to a
Seattle Department of Transportation report.
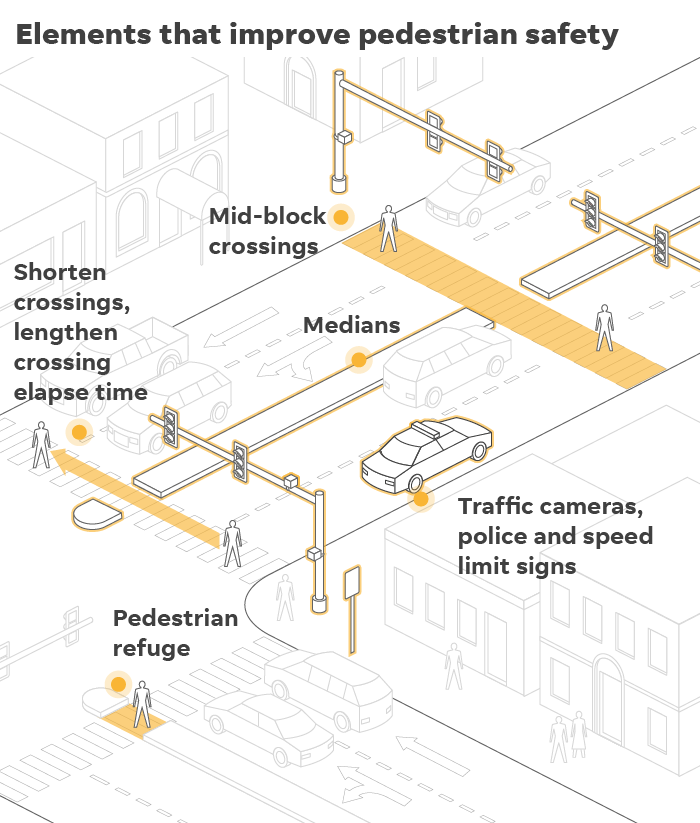
Infrastructure changes designed to better protect pedestrians by reducing traffic lanes, adding pedestrian refuge islands and midblock crossings are often credited with reducing speeds and improving safety. That’s part of the vision for a major thoroughfare on Detroit’s east side. East Jefferson Avenue, a multilane street that connects the city to the suburban Grosse Pointe communities, is undergoing a “road diet,” dropping from seven lanes to five, adding protected bike lanes and improving crosswalks.
In Detroit, which has the highest per-capita pedestrian death rate among large cities, deaths dropped in 2016, after the city, as part of its emergence from bankruptcy,
added more than 60,000 new streetlights.
Nationally, speed and red-light cameras are also credited with making streets safer for pedestrians. As of May, 421 communities were using red-light cameras and 143 communities were using speed cameras to enforce traffic laws, according to the Insurance Institute.
Cities, including Honolulu and Montclair, California, have focused on pedestrians to reduce fatalities. Both cities passed laws against texting and walking when crossing streets. Honolulu council member Brandon Elefante told the Free Press in May that “the hope is more municipalities will adopt similar language looking at pedestrians and vehicles.”
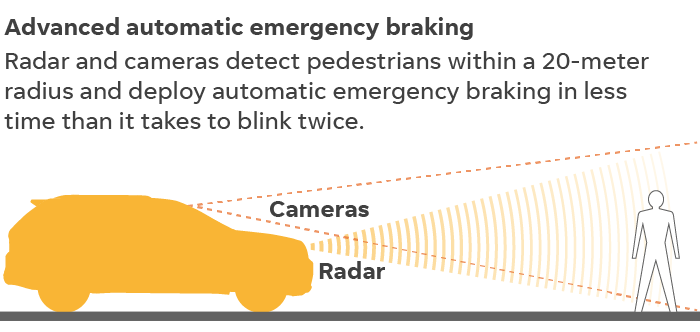
Automatic braking
Vehicle safety features, however, are believed to be just as crucial to reducing pedestrian deaths.
Researchers at the U.S. Department of Transportation’s Volpe Center have found that the use of pedestrian crash avoidance/mitigation systems and features such as automatic emergency braking, could reduce up to 5,000 vehicle-to-pedestrian crashes and 810 fatal crashes per year.
Most automakers have voluntarily committed to installing low-speed automatic emergency braking systems by 2022, but the progress to date varies greatly, according to NHTSA.
Some brands make automatic emergency braking standard — Tesla (99 percent), Mercedes-Benz (96 percent), Volvo (68 percent) and Toyota (56 percent).
Others, as of last year, produced only a small portion of their fleet with the technology — Fiat Chrysler (6 percent), Mitsubishi (3 percent), Ford (2 percent) and Jaguar/Land Rover and Porsche (none). General Motors produced 20 percent of its fleet with AEB.
Fiat Chrysler spokesman Eric Mayne, said the automaker will meet the standard by 2022. He noted that automatic emergency braking is currently available on 15 models in nine segments.
Elizabeth Weigandt, a Ford spokesperson, said Ford began offering its pre-collision assist with AEB on the 2017 Fusion and now makes it available on seven other models.
“We will standardize AEB on 15 percent of vehicles in 2018 and are well ahead of meeting the agreement to standardize across our lineup by 2022,” she said.
General Motors spokesman Tom Wilkinson noted that “GM was part of the agreement to make AEB standard in the U.S. by the end of 2022 and we will meet that target. More than two-thirds of our models now have AEB available.”
Catherine Chase, president of Advocates for Highway and Auto Safety, said the voluntary nature of the 2022 commitment means automakers can walk away if they choose and pedestrian-specific crash avoidance technology might not be included.
“We think that they should be put in as standard equipment in all vehicles,” she said.
The group’s research director, Shaun Kildare, noted that it’s not simply a delay of a year or two. Because it takes about 10 years for the fleet to change, delays in implementing new technology can mean decades before the improvements are in most vehicles on the road.
“This is a fundamental technology to reaching autonomous vehicles. … Why isn’t every automaker putting these in so we know we’re not killing people needlessly?”
Shaun Kildare, research director, Advocates for Highway and Auto Safety
From a practical standpoint, automakers should be pushing forward because of the rush to develop autonomous vehicles, Kildare said.
“This is a fundamental technology to reaching autonomous vehicles. You need to know how your system is going to identify objects on the road and if you’re going to be able to respond to it,” Kildare said, noting the risks highlighted by this year’s fatal self-driving Uber crash in Arizona. “Why isn’t every automaker putting these in so we know we’re not killing people needlessly?”
But Chase said automakers tend to resist mandates, preferring to decide on their own what should and should not go into a vehicle. Some of that resistance involves concerns about cost.
Once a technology is in wide use, however, the cost tends to decrease, Chase said. That technology can also become a selling point, she said, using the example of backup cameras. Chase said there had been resistance to adding backup cameras, which became required on new vehicles in the U.S. in May, but drivers who are familiar with them now demand them.
The Alliance of Automobile Manufacturers, which represents the industry on policy issues, views advanced driver-assistance and crash avoidance technology “as a much better approach” to improving pedestrian safety than an overhauled New Car Assessment Program that had been proposed by NHTSA, spokeswoman Gloria Bergquist said in an email.
“These technologies are well researched and have proved to be beneficial,” Bergquist said.
The alliance’s members appear to be split on whether the pedestrian protection rating is a good move.
For example, General Motors told NHTSA regulators in a February 2016 letter that it did not support a separate rating for pedestrian safety, saying “an overall crash performance category is the appropriate place to address the crashworthiness elements of pedestrian protection.”
But Toyota enthusiastically supported the agency’s recommendation. It “will allow consumers to more easily understand a vehicle’s safety performance,” the Japanese automaker told NHTSA in its own February 2016 letter.
European standards
Automakers face a different landscape in Europe, where pedestrian safety is a key rating component. The rating agency Euro NCAP includes detailed information on its website about various vehicles. Color-coded images even show where pedestrian impact protection is good, such as on the hood (or bonnet) of a 2017 BMW 6 Series GT, or where it is poor on the same vehicle, such as along a strip above the grille.
This is an image from a video showing how vehicles are tested in Europe to determine pedestrian safety ratings. (Courtesy of Euro NCAP)
EURO NCAP
“Euro NCAP has encouraged vehicle manufacturers to consider pedestrian impacts in the vehicle design and this can be seen most commonly as space available beneath the hood of the vehicle, padding to bumper areas, and more (compliant) structures at the base of the windscreen and on the bonnet leading edge. The space between the hood and engine allows the bonnet to absorb the impact of the pedestrian’s head before it contacts the very hard engine structures beneath. A similar principle is also applied to the bumper/front end to protect the vulnerable knee joint of a pedestrian,” according to the agency
The agency said that the testing had led to innovative countermeasures such as the deployable hood, which can lift up slightly, and external airbags, both designed to cushion the blow.
“The technology is really going to be our savior. In the short term, we’ve been getting dumber faster than our cars have been making us smarter.”
Tom Mayor, industrial manufacturing strategy practice leader at KPMG
Euro NCAP, which recently added testing of emergency braking systems to cover cyclists, noted that about 25,000 people die in traffic crashes in Europe each year and almost half of those killed in 2017 were vulnerable road users.
“Moreover, for every person killed in traffic crashes, about five more suffer serious injuries with life-changing consequences. Serious injuries are common and often costlier to the society because of longtime rehabilitation and health-care needs. The majority of the seriously injured on Europe’s roads are vulnerable road users, i.e. pedestrians, cyclists and drivers of powered two-wheelers,” the agency said.
“The technology is really going to be our savior,” said Tom Mayor, industrial manufacturing strategy practice leader at the consulting firm KPMG, who has had discussions with auto companies about improving in-vehicle infotainment systems. “In the short term, we’ve been getting dumber faster than our cars have been making us smarter.”
Contact Eric D. Lawrence: elawrence@freepress.com. Follow him on Twitter: @_ericdlawrence. Jason Pohl of the Arizona Republic, Yolanda Jones of The (Memphis) Commercial Appeal, and Chris Woodyard and Zlati Meyer of USA TODAY contributed to this report.