When airports are screening passengers for a communicable disease,
you know it’s serious. No one wants another H1N1. As of this writing,
the Wuhan China outbreak of coronavirus has infected more than 800,
killed 41 people, and found its way to the United States in two
confirmed cases. No doubt tomorrow’s news will broadcast even larger
numbers. Public health officials are still working to figure out exactly
how the coronavirus is spreading, but they are clear on one point: It
needs to be contained. Data visualization can help them do that.
From a public health perspective, containment and, eventually,
eradication are always the goals for communicable diseases. Smart public
health officials understand that containment requires educating the
public about how diseases spread, with an urgency that gets folks to pay
attention.
But traditionally, public health officials have focused their
communication efforts at other public health officials and when nerds
talk to nerds they use nerd-speak. Which means communication looks
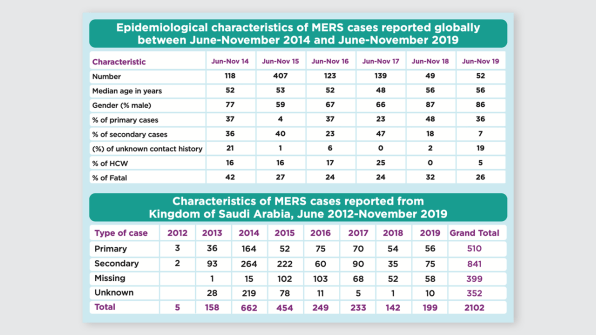
something like this: [Image: WHO]
Which is from a World Health Organization report
on a strain of coronavirus. A table of numbers doesn’t inspire much
action among the public because tables are dense, our brains don’t
process them well, and nothing meaningful pops out.Enter data
visualization. Graphics can teach people where diseases are, how they
spread, and how to stop the outbreak. I know because I am a data visualization nerd,
and I teach people how to communicate their data more effectively. I
have worked with public health agencies from Alaska to Florida, from
community health departments to our national Centers for Disease Control
and Prevention, to help them improve their visuals (and, as a result,
save some lives).
Though public health officials have been knee deep in data for
decades, visualizing it effectively is still a work in progress. It’s
more important than ever for public health agencies to use data
visualization to communicate with the masses, as the public is bombarded
with more information each day and in need of a way for the most
pressing issues to cut through the noise. Here are three ways data
visualization and design are helping public health officials stop the
spread of infectious diseases.
The What/Where Stage
The first stage of visualizing communicable disease data is typically
to show where the disease has been identified on a map. This is the
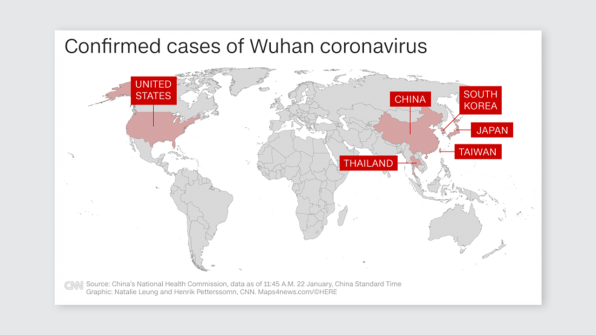
What/Where stage – what is happening and where. CNN recently showed this map of the coronavirus.
[Image: CNN]
The simple visual aid of the color red in the United States will get
some Americans to perk up and pay attention. This isn’t something just
happening in Wuhan.
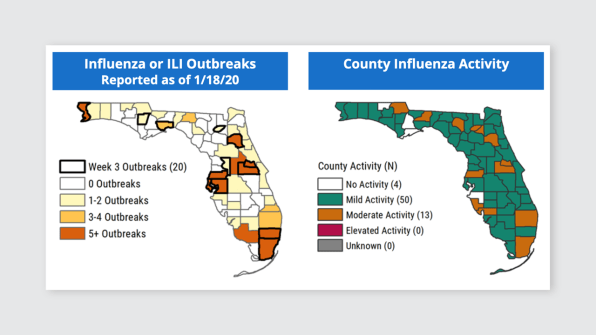
Many states, including Florida, use a similar visual to plot out where more common viruses, like flu, are located: [Image: Florida Department of Health]
It is definitely important to know where activity is present. But
just knowing what a virus is and where it is infecting people isn’t
going to stop it’s spread. Public health officials can actually move the
public to a deeper understanding by creating graphics that answer more
intense questions.
The So What Stage
The So What stage of visualizing communicable diseases requires
public health officials to tell a bit of a story with their data.
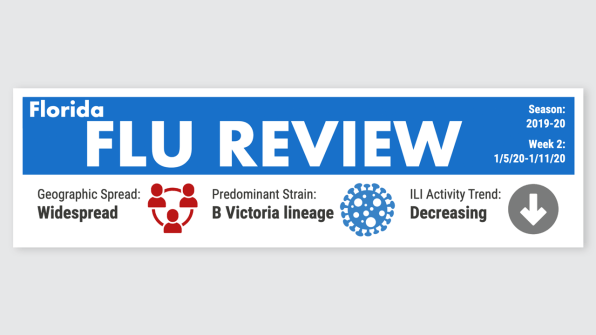
The very top of Florida’s weekly flu review includes So What information: [Image: Florida Department of Health]
They use icons to indicate that, though the flu virus is widespread, it is decreasing. Helpful info.
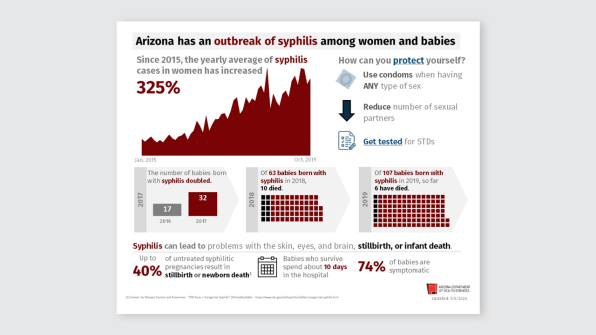
Arizona Department of Health
addressed So What in their reporting on syphilis by including
historical data in a red area graph pointing to a substantial increase
and using black squares in their icon arrays to tell a story about
deaths among babies born with the communicable disease. Ugh, it hurt my
heart just to write that sentence. Yes, data visualization can do that. [Image: Arizona Department of Health Services]
And while the visuals might not be as sophisticated as those from The New York Times,
this isn’t a moment when an interactive, exploratory,
so-beautiful-it-is-almost-art design makes sense. We need something
quick and easy-to-understand by folks who range in ages, abilities, and
languages.
The So What stage is where public health officials lay out the
consequences of the disease, to communicate to the public the urgency of
the situation and make them feel some emotion. Now folks are paying
attention. This is exact when public health officials swoop in with a
visual for the next stage, which aims directly at containment and
eradication.
The Now What Stage
Once public health officials give the data meaning, the public is
likely to understand the significance and scope of the problem. They are
ready to take action. They are asking, “Now what?”
The Now What stage of visualizing communicable disease data is where
public health officials have the chance to educate a worried
constituency on the exact actions that need to be taken to safeguard
ourselves and each other. Arizona answered “Now what?” in the graphic
above in their “How can you protect yourself?” section. Centers for Disease Control and Prevention
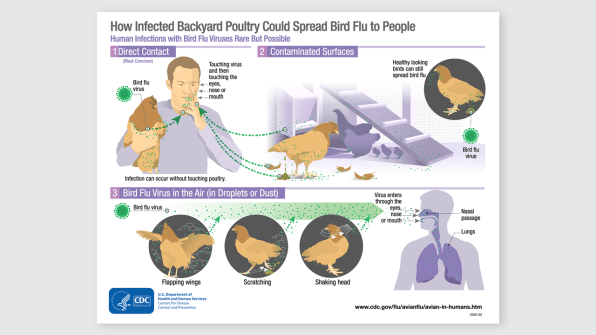
has been making strides to speak to “Now what?” by translating their
depth of health knowledge through educational infographics, like how
bird flu can spread to humans.
[Image: CDC]
What had traditionally been communicated in paragraphs of text, which
followed a dense statistical table, is now an illustrated poster that
can hang in a clinic waiting room.
With something as globally threatening as the Wuhan coronavirus, we
need to take action quickly. Public health officials should take note of
successful data visualization and designs used in other awareness
campaigns. And we, the public, should ask for the data, presented with
clear messaging and strong visuals. Particularly in an age where some
real news is labeled as fake and some fake news looks all too real, the
more we ask What? So What? and Now What? from our news sources, the more
we can do our part to contain and eradicate before an outbreak becomes
widespread. https://www.fastcompany.com/90455933/how-design-can-stop-the-spread-of-the-wuhan-coronovirus
If the Food and Drug Administration follows the advice of its outside
advisers, the agency will within days grant the first-ever approval to a
drug designed to make peanut allergy sufferers less likely to have a
dangerous reaction.
Called Palforzia, the drug was developed by the California-based
biotech Aimmune. It’s in close competition with a French company called
DBV Technologies, which should see the FDA decide on its patch-based
peanut allergy treatment by August.
Both rely on a strategy that allergists have tried outside of the FDA
approval pathway for some time: exposing patients to tiny and
increasing amounts of peanut-related proteins, in theory making it
possible for them to tolerate accidental exposures. Aimmune uses peanut
flour, while DBV uses peanut antigen.
But the effort to gain wider acceptance of this treatment approach
has stirred controversy. Critics have pointed to the risk of dangerous
anaphylactic reactions for patients undergoing treatment, while payers
may question the value of the treatment compared to avoidance of peanut
exposure.
Palforzia is peanut flour that has been processed using FDA-approved
good manufacturing practices to standardize doses — peanut flour has
been used as an oral immunotherapy, but not ever approved by the FDA.
Patients begin with a small dose and increase gradually to 300
milligrams daily.
Aimmune hopes to win approval for Palforzia in patients aged 4 to 17.
In this group, a significantly greater number who had taken Palforzia
were able to tolerate a food challenge at the conclusion of Aimmune’s key trial than patients who received placebo.
Although positive, results also showed more study participants taking
Palforiza discontinued treatment than those on placebo, while
experiencing a higher rate of allergic reactions and increased use of
epinephrine.
In both the active treatment arm and the placebo group, patients were applying strict avoidance practices.
“I think it’s hard to argue that this product is safe when it
increases the risk of the thing it is designed to prevent,” John Kelso, a
member of the FDA advisory committee that reviewed the Palforzia
application and an allergist with the Scripps Clinic in San Diego, said
during the committee’s hearing. Kelso was one of two votes against
approving Palforzia on the nine-member panel.
Most, however, were supportive and argued Palforiza met the standards for approval.
Insurer coverage is also a question. The Institute for Clinical and
Economic Review, a non-profit that measures the cost effectiveness of
drugs, said Palforzia would push healthcare spending above its budget impact threshold
if priced at an assumed cost of $4,200 per year. Only 41% of eligible
patients would be able to take Palforzia while keeping spending below
the group’s $990 million budget ceiling.
Aimmune is considering pricing Palforzia, if approved, at a cost
between $3,000 and $20,000, according to a recent company presentation.
ICER’s own advisors, called the California Technology Assessment
Forum, voted 12-4 that the net health benefit of Palforzia and avoidance
had not been proven superior to avoidance alone.
That organization was also asked to assess DBV’s patch product,
called Viaskin Peanut. A similar negative 12-4 vote was cast on its net
health benefit.
Both treatments provide only a small patient benefit, according to
the ICER report, adding 0.75 “quality adjusted life year,” or QALY — a
measure of health improvement — over avoidance in the case of Palforzia,
and 0.26 in the case of Viaskin Peanut.
If the FDA decides to approve Palforzia, it could require risk mitigation measures that could limit initial uptake.
Stifel analyst Derek Archila, citing these potential restrictions,
wrote in a Jan. 7 note to clients he believes investor estimates are
“aggressive.” He forecasts $65 million in 2020 sales.
In addition, uptake may be restrained by the need for allergists to
learn how to use it and issues with patient adherence because of side
effects and complicated dosing, Archila wrote.
DBV, meanwhile, has submitted Viaskin Peanut to the FDA, and an
advisory committee is likely to be convened to consider its application. https://www.biopharmadive.com/news/aimmune-fda-decision-palforzia-peanut-allergy/571050/
As infectious disease specialists and epidemiologists race to contain
the outbreak of the novel coronavirus centered on Wuhan, China, they’re
getting backup that’s been possible only since the explosion in genetic
technologies: a deep-dive into the DNA of the virus known as 2019-nCoV.
Analyses of the viral genome are already providing clues to the
origins of the outbreak and even possible ways to treat the infection, a
need that is becoming more urgent by the day: Early on Saturday in
China, health officials reported 15 new fatalities in a single day,
bringing the death toll to 41. There are now nearly 1,100 confirmed
cases there.
Reading the DNA also allows researchers to monitor how 2019-nCoV is
changing and provides a roadmap for developing a diagnostic test and a
vaccine.
“The genetics can tell us the true timing of the first cases” and
whether they occurred earlier than officials realized, said molecular
biologist Kristian Andersen of Scripps Research, an expert on viral
genomes. “It can also tell us how the outbreak started — from a single
event of a virus jumping from an infected animal to a person or from a
lot of animals being infected. And the genetics can tell us what’s
sustaining the outbreak — new introductions from animals or
human-to-human transmission.”
Scientists in China sequenced the virus’s genome and made it available
on Jan. 10, just a month after the Dec. 8 report of the first case of
pneumonia from an unknown virus in Wuhan. In contrast, after the SARS
outbreak began in late 2002, it took scientists much longer to sequence
that coronavirus. It peaked in February 2003 — and the complete genome
of 29,727 nucleotides wasn’t sequenced until that April.
Since the sequencing of the first 2019-nCoV sample, from an early
patient, scientists have completed nearly two dozen more, said Andrew
Rambaut of the University of Edinburgh, an expert on viral evolution.
That pace is “unprecedented and completely unbelievable,” said Andersen,
who worked on sequencing the Ebola genome during the 2014 outbreak.
“It’s just insane.”
The genome of the Wuhan virus is 29,903 bases long, one of many clues
that have led scientists to believe it is very similar to SARS.
By comparing the two dozen genomes, scientists can address the “when
did this start” question. The 24 available samples, including from
Thailand and Shenzhen as well as Wuhan, show “very limited genetic
variation,” Rambaut concluded on an online discussion forum where
virologists have been sharing data and analyses. “This is indicative of a
relatively recent common ancestor for all these viruses.”
Given what’s known about the pace at which viral genomes mutate, if
nCoV had been circulating in humans since significantly before the first
case was reported on Dec. 8, the 24 genomes would differ more. Applying
ballpark rates of viral evolution, Rambaut estimates that the Adam (or
Eve) virus from which all others are descended first appeared no earlier
than Oct. 30, 2019, and no later than Nov. 29.
The progenitor virus itself was almost certainly one that circulates
harmlessly in bats (as SARS does) but has an “intermediate reservoir” in
one or more animals that come into contact with people, Andersen said.
Presumably, that reservoir is one of the species of animals at the Wuhan
market thought to be ground zero for the outbreak. The ancestor of
2019-nCoV existed in that species for some unknown time, never infecting
people, until by chance a single virus acquired a mutation that made it
capable of jumping into and infecting humans.
The genome sequences suggest that was a one-time-only jump. “The
genomes [from the 24 samples] are very uniform,” Andersen said. “If
there had been multiple introductions,” including from many different
animals, “there would be more genomic diversity. This was a single
introduction.”
That means that what’s sustaining the spread is human-to-human
transmission (suggesting that closing Wuhan’s animal market is very much
an after-the-horse-has-fled-the-barn reaction).
Unfortunately, genetic analysis can’t identify what animal species
the coronavirus jumped from into humans. But an analysis by a team from
the Wuhan Institute of Virology, posted
to the preprint server bioRxiv, determined that the genome of this
coronavirus (the seventh known to infect humans) is 96% identical to
that of a bat coronavirus, suggesting that species is the original
source. (Writing in the New England Journal of Medicine on Friday,
another team of scientists in China reported that the new coronavirus is 86.9% identical to the bat SARS-like coronavirus.)
Virologists differ on whether it’s possible to read out viral
properties from just the genome sequence, such as whether the microbe is
spread by coughing, sneezing, touching, or merely breathing. But the
analysis by the Wuhan Institute team found that it enters human cells
using the same doorway that SARS did. Called angiotensin converting
enzyme 2 (ACE2), the door is a receptor to which a “spike protein” on
the virus’s surface first attaches and then enables the virus to fuse
with the host cell.
If ACE2 is “druggable,” blocking it could conceivably treat
2019-nCoV. “It should be expected and worth to test if ACE2 targeting …
drugs can be used for nCoV-2019 patients,” the scientists wrote.
The genome sequences have more to give. They “will be crucially
important for development of diagnostics [and] vaccines,” said biologist
Richard Ebright of Rutgers University.
For instance, the genome-editing technology CRISPR is the basis for Cambridge, Mass.-based startup Sherlock Biosciences’
diagnostics, which promise to slash how long it takes to make a
definitive identification. In the U.S, that’s now done only by sending
samples to the Centers for Disease Control and Prevention, which uses a
technology invented in the 1980s, polymerase chain reaction or PCR, to
identify the presence of coronavirus.
“Our vision is that our [CRISPR-based] SHERLOCK and INSPECTR
platforms are tailor-made for outbreaks like coronavirus,” said Sherlock
CEO Rahul Dhanda, who declined to discuss “specific plans related to
coronavirus.”
And as scientists keep adding 2019-nCoV genome sequences to their
collection, they could get an early glimpse of whether the virus is
mutating in a way that could make it more dangerous or more
transmissible. “You need continuous sequencing,” Andersen said.
Two papers published Friday in the journal the Lancet offer some of the first rigorous analyses of patients who contracted a novel coronavirus that has broken out in China
and spread to other countries. Among their discoveries: The virus does
not only affect people with other, underlying health conditions, and
people who are not showing symptoms can still be carrying the virus.
In one study,
researchers analyzed data from the first 41 patients who were admitted
to hospitals with confirmed cases of the infection in the central
Chinese city of Wuhan, where the outbreak is believed to have originated
last month. Two-thirds had been to a large seafood market that also
sold wild animals for meat and is thought to be where the virus jumped
from an animal source to people. The median age of the patients was 49.
The patients displayed a wide range of symptoms, many of which were
similar to those caused by SARS, another coronavirus, which caused a
global outbreak in 2002-2003 that started in China. All of them had
pneumonia, and most had fever and cough. Some people had fatigue; rarer
symptoms included headache and diarrhea. The researchers noted that
patients with SARS more frequently had runny noses, sore throats, and
diarrhea than those with the novel coronavirus, which is provisionally being called 2019-nCoV.
One key finding: It’s not only people with other health conditions
that are getting sick, the researchers reported. Some of the fatal cases
caused by the virus have been among people with underlying diseases
like diabetes, liver disease, and hypertension, but the majority of the
first 41 patients infected with the disease in Wuhan were healthy. The
researchers noted that SARS infections similarly did not only affect
people with other conditions.
About a third of the 41 patients needed intensive care, and six of
them died. Some of the patients with more serious illnesses suffered
from a dangerous immune system overreaction called a cytokine storm, but
the researchers said they still did not have a good understanding of
how the virus affects the immune system.
As of Friday, there were more than 830 cases of the coronavirus
infection in China, with 25 deaths, and a handful of cases in places —
including Thailand, Japan, South Korea, and the United States — that were in people who traveled to those countries from China.
The second paper
focused on one family who came down with pneumonia in Shenzhen. Five
family members had recently traveled to Wuhan and had the virus, as did
one relative who had not traveled to Wuhan.
So far, authorities have only confirmed human-to-human transmission of the virus
among families and in health care clinics — settings where people are
likely to be in close contact with each other, according to the World
Health Organization. This appears to be the case with the family that
was studied. Still, health officials do not know exactly how efficiently
the virus can pass among people.
One child with the virus did not show any symptoms. Health
authorities have said that people with the virus have shown a range of
symptoms, from very mild to very severe. But an asymptomatic infection
raises the question of whether people have to be showing signs of the
disease to pass it to people, a question that experts are rushing to
answer.
“Because asymptomatic infection appears possible, controlling the
epidemic will also rely on isolating patients, tracing and quarantining
contacts as early as possible, educating the public on both food and
personal hygiene, and ensuring health care workers comply with infection
control,” Dr. Kwok-Yung Yuen from the University of Hong Kong-Shenzhen
Hospital, who led the research, said in a statement.
In a commentary piece
also published Friday by the Lancet, Dr. David Heymann, an infectious
disease epidemiologist at the London School of Hygiene and Tropical
Medicine, wrote that “the picture these two manuscripts paint is of a
disease with a 3-6 day incubation period and insidious onset.”
The researchers who wrote the two papers and other experts cautioned
that these were small studies with limited numbers of patients in a
rapidly evolving outbreak. But they noted that sharing information like
this as quickly and rigorously as possible can help shape the response.
“The information in these articles are pieces of the jigsaw puzzle
that are being fit together by WHO as it continues to collect official
reports and informal information from its virtual groups of national
clinicians, epidemiologists, and virologists working at outbreak sites
and brought together from around the world,” Heymann wrote. “When pieced
together, these emerging data will permit regular refinement of the
risk assessment, and real-time guidance to countries for patient
management and outbreak control, including the best case definition for
use in surveillance around outbreak sites and elsewhere.”
The new coronavirus rapidly spreading in China and nearby countries
seems to trigger symptoms similar to those seen in the severe acute
respiratory distress syndrome (SARS) coronavirus outbreak in 2003, two
new studies show.
Published Jan. 24 in The Lancet journal, these are the first
clinical studies conducted on patients struck by the new coronavirus,
dubbed 2019-nCoV. As of Friday morning, there were 830 confirmed cases
and 26 deaths in China tied to the coronavirus, which originated in the
central Chinese city of Wuhan.
Officials at the U.S. Centers for Disease Control and Prevention on Friday also announced a second U.S. case of the virus,
in a person in Illinois. The first case occurred in a man in Washington
state. Both patients had returned from travel in China, the CDC said,
and are being monitored.
The two new studies examine the course of infection in some of the first cases of the Wuhan virus.
In one study, researchers looked at clinical records, laboratory
results, imaging findings and epidemiological data on the first 41
infected people admitted to the hospital in Wuhan between Dec. 16, 2019
and Jan. 2, 2020.
Patients were typically middle-aged (average age 49), three-quarters
were men, and two-thirds had visited a local seafood market thought to
be where the virus originated.
Similar to the 2003 SARS outbreak in China, most patients who came
down with the Wuhan coronavirus were healthy, without any chronic
underlying health issues. And symptoms also resembled those of SARS,
said Chinese researchers led by Bin Cao, from the China-Japan Friendship
Hospital and Capital Medical University, both in Beijing.
All of the hospitalized patients
had developed pneumonia, nearly all (98%) had a fever, three-quarters
developed a cough, 44% felt fatigued, and 55% had some shortness of
breath. Symptoms such as headache or diarrhea were rare, however.
On the other hand, “despite sharing some similar symptoms to SARS
[such as fever, dry cough, shortness of breath], there are some
important differences,” Cao said in a Lancet news release.
For example, people with the new virus typically didn’t have runny
noses or other symptoms involving the upper respiratory tract, he said.
And very few had intestinal symptoms such as diarrhea, which occurred in
about a quarter of SARS patients.
Severe illness—enough to require admittance to the ICU—occurred in
about a third of the hospitalized patients, Cao’s team said, and six
patients died.
A condition involving immune system dysfunction known as a “cytokine
storm” occurred in some of these very ill patients, but it’s not yet
clear how the new virus affects the immune system, the researchers said.
As of Jan. 22, a majority of patients in the study (68%) have
recovered enough to be discharged from the hospital, the report noted.
In the second study, the first to involve gene analysis, researchers
tracked the course of 2019-nCoV in a family of seven people. Five family members
had recently traveled to Wuhan and were found to carry 2019-nCoV, and
one family member who had not traveled with them also was found to be
infected with the virus.
None of the infected family members had visited food markets or
animals while in Wuhan, suggesting that person-to-person transmission
was at play.
The seventh family member—a child whose mother said had worn a
surgical mask during their stay in Wuhan—was not infected with the
virus.
As well, a second child was infected but showed no clinical symptoms
of the illness, according to researchers led by Dr. Kwok-Yung Yuen, from
the University of Hong Kong-Shenzhen Hospital. That suggests that
2019-nCoV could be spread person-to-person by people who don’t even
realize they are infected, the researchers said.
“Our findings are consistent with person-to person transmission of
this new coronavirus in hospital and family settings, and the reports of
infected travelers in other countries,” Yuen said in the release.
“Because asymptomatic infection appears possible, controlling the
epidemic will also rely on isolating patients, tracing and quarantining
contacts as early as possible, educating the public on both food and
personal hygiene, and ensuring health care workers comply with infection
control.”
Examining the course of illness among the various family members,
symptoms appeared to develop within a few days of contact with sick
individuals.
Gene tests revealed that five of the family members carried a form of
2019-nCoV that had a type of protein allowing it to enter healthy
cells. Yuen’s team was also able to use samples from two patients to map
the full genome of 2019-nCoV.
“With the improved surveillance network and laboratory capability
developed following the SARS pandemic, China has now been able to
recognize this new outbreak within a few weeks and has made the virus
genome publicly available to help control its spread,” said study
co-author Dr. Rosana Wing-Shan Poon, from the University of Hong Kong.
“Learning the lessons from SARS, which started as animal-to-human
transmission, all game meat trading should be better regulated to
terminate this potential transmission route,” Poon said. “Further
investigations are needed to clarify the potential threat posed by this
emerging virus and asymptomatic cases.”
There remains a controversy in scientific circles today regarding the
value of lithium therapy in treating Alzheimer’s disease. Much of this
stems from the fact that because the information gathered to date has
been obtained using a multitude of differential approaches, conditions,
formulations, timing and dosages of treatment, results are difficult to
compare. In addition, continued treatments with high dosage of lithium
render a number of serious adverse effects making this approach
impracticable for long term treatments especially in the elderly.
In a new study, however, a team of researchers at McGill University
led by Dr. Claudio Cuello of the Department of Pharmacology and
Therapeutics, has shown that, when given in a formulation that
facilitates passage to the brain, lithium in doses up to 400 times lower
than what is currently being prescribed for mood disorders is capable
of both halting signs of advanced Alzheimer’s pathology such as amyloid plaques and of recovering lost cognitive abilities. The findings are published in the most recent edition of the Journal of Alzheimer’s Disease. Building on their previous work
“The recruitment of Edward Wilson, a graduate student with a solid
background in psychology, made all the difference,” explains Dr. Cuello,
the study’s senior author, reflecting on the origins of this work. With
Wilson, they first investigated the conventional lithium formulation
and applied it initially in rats at a dosage similar to that used in
clinical practice for mood disorders. The results of the initial
tentative studies with conventional lithium formulations and dosage were
disappointing however, as the rats rapidly displayed a number of
adverse effects. The research avenue was interrupted but renewed when an
encapsulated lithium formulation was identified that was reported to
have some beneficial effects in a Huntington disease mouse model.
The new lithium formulation was then applied to a rat transgenic
model expressing human mutated proteins causative of Alzheimer’s, an
animal model they had created and characterized. This rat develops
features of the human Alzheimer’s disease, including a progressive
accumulation of amyloid plaques in the brain and concurrent cognitive
deficits.
“Microdoses of lithium at concentrations hundreds of times lower than applied in the clinic for mood disorders
were administered at early amyloid pathology stages in the
Alzheimer’s-like transgenic rat. These results were remarkably positive
and were published in 2017 in Translational Psychiatry and they
stimulated us to continue working with this approach on a more advanced
pathology,” notes Dr. Cuello.
Encouraged by these earlier results, the researchers set out to apply
the same lithium formulation at later stages of the disease to their
transgenic rat modelling neuropathological aspects of Alzheimer’s
disease. This study found that beneficial outcomes in diminishing
pathology and improving cognition can also be achieved at more advanced
stages, akin to late preclinical stages of the disease, when amyloid
plaques are already present in the brain and when cognition starts to
decline.
“From a practical point of view our findings show that microdoses of
lithium in formulations such as the one we used, which facilitates
passage to the brain through the brain-blood barrier while minimizing
levels of lithium in the blood, sparing individuals from adverse
effects, should find immediate therapeutic applications,” says Dr.
Cuello. “While it is unlikely that any medication will revert the
irreversible brain damage at the clinical stages of Alzheimer’s it is
very likely that a treatment with microdoses of encapsulated lithium
should have tangible beneficial effects at early, preclinical stages of
the disease.” Moving forward
Dr. Cuello sees two avenues to build further on these most recent
findings. The first involves investigating combination therapies using
this lithium
formulation in concert with other interesting drug candidates. To that
end he is pursuing opportunities working with Dr. Sonia Do Carmo, the
Charles E. Frosst-Merck Research Associate in his lab.
He also believes that there is an excellent opportunity to launch
initial clinical trials of this formulation with populations with
detectable preclinical Alzheimer’s pathology or with populations
genetically predisposed to Alzheimer’s, such as adult individuals with
Down Syndrome. While many pharmaceutical companies have moved away from
these types of trials, Dr. Cuello is hopeful of finding industrial or
financial partners to make this happen, and, ultimately, provide a
glimmer of hope for an effective treatment for those suffering from
Alzheimer’s disease.
“NP03, a Microdose Lithium Formulation, Blunts Early Amyloid
Post-Plaque Neuropathology in McGill-R-Thy1-APP Alzheimer-Like
Transgenic Rats,” by Wilson, Do Carmo, Cuello, et al. was published
online on December 16, 2019 in the Journal of Alzheimer’s Disease.
More information:
Edward N. Wilson et al, NP03, a Microdose Lithium Formulation, Blunts
Early Amyloid Post-Plaque Neuropathology in McGill-R-Thy1-APP
Alzheimer-Like Transgenic Rats, Journal of Alzheimer’s Disease (2019). DOI: 10.3233/JAD-190862
Sickle cell disease drugs made by Novartis and Global Blood
Therapeutics (GBT) may not be cost effective at current prices, a draft
report published on Friday suggested, widening the debate over U.S.
healthcare affordability.
Novartis and GBT disputed the preliminary conclusions by the
Boston-based Institute for Clinical and Economic Review (ICER). The
institute scrutinised Novartis’s Adakveo and GBT’s Oxbryta, both
approved last year, and Emmaus Medical’s Endari, to treat the inherited
disease that disproportionately affects African Americans.
The finding that the costs of all three medicines would likely have
to be slashed to achieve acceptable cost-effectiveness thresholds comes
as Congress and U.S. President Donald Trump weigh action over high
healthcare costs.
Insurers and governments use privately funded ICER’s conclusions to help set reimbursement rates.
ICER said it concluded that Adakveo’s annual cost should be $25,410,
down from an estimated $88,000 bill, and that Oxbryta must be trimmed to
$9,218 from about $84,000, to meet cost-effectiveness thresholds.
Endari must be cut to $3,859 from $24,000 to be cost-effective, the
group added.
“Treatment costs were the main driver of the cost-effectiveness
results,” said ICER, which is taking public comment until Feb. 20 before
final publication this year.
Shares in GBT fell more than 5.5% on Friday, while Novartis shares closed 0.3% lower.
ICER seeks to measure how many years of good health – a
quality-adjusted life year, or QALY – may be gained with a new
treatment, and the incremental cost for that health gain.
At the current estimated costs for Adakveo, Oxbryta and Endari, all
the QALYs exceeded $1 million, ICER said, well above the $150,000 the
group ordinarily considers an appropriate cost-effectiveness threshold.
Novartis countered that ICER had not appropriately weighed Adakveo’s
benefits, including reducing pain crises suffered by sickle cell disease
(SCD) patients or potentially helping cut hospital stays.
“We look forward to gaining a better understanding of the approach
ICER used to make its assessment and to helping them better understand
the value of Adakveo,” Novartis said.
‘FLAWED, PREMATURE’
San Francisco-based GBT contended that ICER’s review conflicts with
the U.S. Food and Drug Administration’s goal of speeding medicines to
patients.
“ICER’s review is flawed, premature and risks adversely impacting
access to new, potentially transformative therapies,” GBT said.
U.S.-based Emmaus could not immediately be reached for comment.
ICER said its draft report may change based on public comments,
including from drugmakers. It also acknowledged setting a drug’s price
may go beyond traditional measures of clinical effectiveness and
cost-effectiveness, to include other, non-financial considerations.
Recent advances in treating long-neglected sickle cell disease
include the three medicines reviewed by ICER and an experimental gene
therapy from Bluebird Bio Inc..
Still, costs are of particular interest. More than half of the
roughly 100,000 U.S. sickle cell disease patients are covered by
government health insurance. https://www.reuters.com/article/us-health-cost-effectiveness/novartis-gbt-sickle-cell-drugs-too-expensive-draft-u-s-report-says-idUSKBN1ZN224