Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I'm Dr F. Perry Wilson of the Yale School of Medicine.
When I was 12, I learned about birth control with 20 other boys in my class in a series of 45-minute sessions with my gym teacher — you know, as nature intended.
I remember very little, save for the fact that he referred to mammary glands as "mammalary" glands.
But pre-teens and teens don't get their information about sex from misinformed gym teachers anymore. We live in the Information Age, where virtually every bit of knowledge on a subject is accessible from the palms of our hands. We are all walking around with thousands of Libraries of Alexandria in our pockets.
And so, of course, the kids get their information from YouTube.
A new study, "What Do Social Media Influencers Say About Birth Control? A Content Analysis of YouTube Vlogs About Birth Control," appearing in the journal Health Communication, posits that this new source of information — the YouTube influencer — is biased. Against birth control. Or at least, against hormonal birth control.
I'll say up front that I think this is an important topic. Where people get their medical information from is something I have spent a lot of time thinking about (and discuss a lot in my book, How Medicine Works and When It Doesn't, coming out later this month).
But I have some issues with the study design that I'll get to in a moment. First, let's look at how the study was done.
Researchers Emily Pfender and Marie Devlin, from the University of Delaware, searched YouTube to find influencers (here defined as people with more than 20,000 subscribers) who were talking about their experience with birth control between 2019 and 2021. Videos from medical professionals were excluded, but of course no one listens to us anyway. They watched 50 videos. During each video, they painstakingly coded the information that was being conveyed about birth control.
These were popular YouTube channels, with an average subscriber count of more than 350,000 individuals.
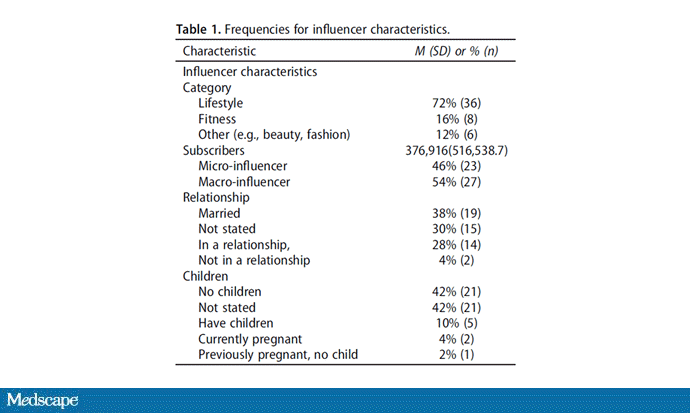
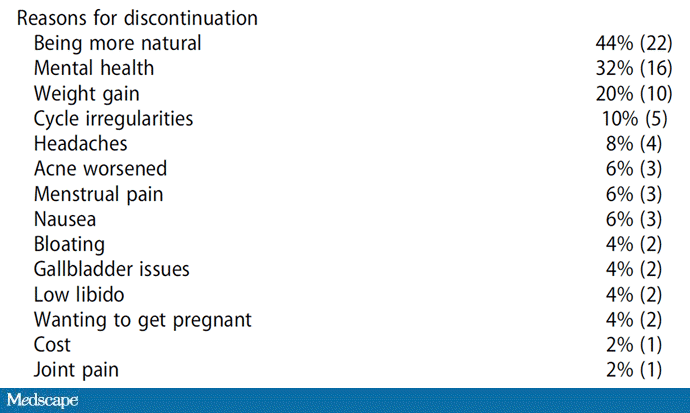
Of the 50 influencers, almost all reported having been on hormonal birth control. And three fourths of the videos (37 out of 50) discussed why those influencers decided to stop hormonal birth control.
The reasons were varied: wanting to be more "natural"; concerns that hormonal contraception was hurting their mental health; weight gain; and so on. It's not that this is misinformation — hormonal contraception can certainly have these side effects; it's that the videos that come up on YouTube focus on these side effects, which may lead impressionable minds to… well, to what exactly?
Most of these influencers who reported stopping hormonal contraceptives did not discuss any alternatives. Of the 20 who mentioned some form of nonhormonal contraception, 15 discussed cycle tracking with an app like Daysy, the most popular app in this space. Just two mentioned condoms and two mentioned IUDs.
In other words, if you get your impression on how contraception works from YouTube influencers, you may come to believe that hormonal birth control is terrible and fertility tracking is a good method of birth control, and that's pretty wrong.
The Daysy app that people keep talking about is basically a cycle-tracking app — charting period days, basal body temperature, cervical mucus, etc. The company touted its product as more than 99% accurate in a paper published in Reproductive Health. That paper has since been retracted for cherry-picking data. And, of course, none of these influencers mentioned that.
I told you up front that I had some issues with study design here and that's true. The authors used the phrase "birth control experience" to find these videos. And I can confirm that when I use that phrase, I get a lot of influencers complaining about hormonal contraception.
But is "birth control experience" the search term most young people would use? If you just search for "birth control," you get a more balanced group of videos — more informative and less, you know, influencer-y. Of course, we all know how easy it can be to fall down the YouTube rabbit hole.
Perhaps the influencer thing is the problem. Multiple studies have shown that influencers online have outsized influence on our opinions. Compared with some fact-spitter like me, what makes someone an influencer is that their viewers feel they are in a relationship together, that they are friends. They do this by fostering a sense of community and of course by revealing personal details about their lives (like their experiences with birth control).
And the trust built through that mechanism, that sharing, however misplaced, is powerful. It's why marketers pay influencers; they have a hold over their subscribers that is quite valuable. And if marketers are paying attention to them, we should be too — because our kids will.
Not being an influencer myself, I can't hope to change too many minds watching this, but I will close with one thing. Young people, it's true that hormonal contraception can have side effects. Talk to your doctor about them. But if you do choose to go off hormonal contraception, please, please don't use the rhythm method. It's not as successful as the influencers will lead you to believe. And it doesn't protect against sexually transmitted infections. Condoms do. And you don't even need an app for that.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale's Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn't, is available for pre-order now.