People who received a new COVID-19 vaccine booster were more likely to contract COVID-19 than people who received no COVID-19 vaccine doses, according to a new study of prisons in California.
Researchers analyzed data from 33 state prisons from January to July 2023 to try to assess the effectiveness of the bivalent shots, which were introduced in the fall of 2022.
Among 96,201 inmates with data on COVID-19 testing and vaccination, researchers identified 2,835 cases.
They found that 1,187 of the cases were among people who had received a bivalent vaccine, versus just 568 cases among the unvaccinated.
The rest were among people who received only monovalent, or old vaccines. That group was excluded from further analysis.
While the population of bivalent recipients was higher than the unvaccinated—36,609 compared to 20,889—the rate of infection was still elevated in the bivalent group owing to nearly double the number of infections, the researchers found.
Infection rates in the group that received bivalent shots was 3.2 percent, over the 2.7 percent in the unvaccinated.
“The bivalent-vaccinated group had a slightly but statistically significantly higher infection rate than the unvaccinated group,” Dr. Robert Mayes of the California Correctional Healthcare Services and the other authors wrote.
Stratifying by age, researchers found that the gap was larger in elderly inmates.
Among inmates at least 65 years old, the infection rate was 6.4 percent among the vaccinated and 4.5 percent among those who had not received a shot. Among inmates at least 50 years old, the rates were 4 percent and 3 percent, respectively.
A person receives a COVID-19 vaccine at Los Angeles International Airport in Los Angeles, Calif., on Dec. 22, 2021. (Frederic J. Brown/AFP via Getty Images)
The former was not statistically significant, researchers said.
“Further research is needed to understand the reasons behind these findings and to consider other factors, such as underlying health conditions. This study underscores the importance of developing vaccines that target residual COVID-19 infections, especially in regard to evolving COVID-19 variants,” the researchers added later.
The group’s corresponding author did not respond to questions, including why they excluded vaccinated people who have not received a bivalent shot.
The group posited that the gap between the vaccinated and unvaccinated may stem from natural immunity or the protection people have after recovering from COVID-19.
They were unable to incorporate natural immunity into their calculations. They also said inmates may not report symptoms, which could skew the results.
Questionable Claims
The researchers acknowledged the negative results, writing that the research “underscores the importance of developing vaccines targeting residual COVID-19 infections, especially regarding evolving COVID-19 variants.”
They also wrote, “This study suggests that while the bivalent vaccine might offer protection against severe outcomes, it may not significantly reduce the risk of overall infections.”
Researchers did not provide evidence from their research supporting the vaccine protecting against severe outcomes.
Dr. Ray Andrews, a retired doctor, said the wording was an example of obfuscation.
“The words ‘may’ and ‘might’ make scientific thesis a personal opinion,” Dr. Andrews told The Epoch Times via email.
“The results showed the vaccines are not ineffective,” he said.
The bivalent vaccines were authorized without clinical trial data and no efficacy data has been produced to this day. U.S. officials are preparing to replace them with new shots owing to poor performance.
Syringes and vials of the Pfizer-BioNTech COVID-19 vaccine are prepared to be administered at a drive-up vaccination site from Renown Health in Reno, Nev., on Dec. 17, 2020. (Patrick T. Fallon/AFP via Getty Images)
Other Studies
Other papers have also found the bivalent shots provide little or no protection.
French researchers, for instance, estimated that a bivalent vaccine added just 8 percent protection against symptomatic infection, while South Korean researchers estimated just 12 percent added protection. Qatari researchers estimated 25 percent relative effectiveness, with lower effectiveness among people with no prior infection.
Cleveland Clinic researchers found in June that employees at the clinic who were “up to date” with their vaccines, or had received a bivalent dose, had a higher risk of becoming infected when compared to others.
“This study highlights the challenges of counting on protection from a vaccine when the effectiveness of the vaccine decreases over time as new variants emerge that are antigenically very different from those used to develop the vaccine,” Dr. Nabin Shrestha and other researchers said at the time.
Observational data has also supported the idea that boosters do not work well.
Earlier papers have provided negative effectiveness estimates for the old vaccines, including for Moderna’s vaccine and Pfizer’s vaccine.
Additional studies have examined bivalent protection against hospitalization or severe illness.
The bivalents as a second or third booster initially boosted protection against severe illness by just 25 percent in the elderly and that protection dropped to 18 percent over time, Italian researchers found.
The U.S. Centers for Disease Control and Prevention found that in healthy adults, those who received a bivalent were more likely to be hospitalized.
Singaporean researchers did find that people with bivalent boosters were less likely to contract COVID-19 or go to the hospital with COVID-19, but they did not adjust for the fact that people who receive vaccines are often healthier than those who do not.
Amid refinery maintenance and rising domestic fuel prices, Russia is set to cut its diesel exports from its ports on the Baltic and Black Seas by nearly 25% in September compared to the export plans for August, Bloomberg reported on Friday, quoting industry data it had seen.
The shipments of diesel out of Russia’s western ports, including some exports from Belarus, are planned at 1.874 million tons in September, or 466,000 barrels per day (bpd), down from about 600,000 bpd planned for August exports, according to Bloomberg’s calculations.
The plan for diesel exports in September lays out the lowest shipments since May this year when spring refinery maintenance was in place.
Now the autumn refinery maintenance is also slashing diesel exports out of Russia.
The primary oil refining capacity that will be offline in Russia is set to soar by 44% in September compared to August amid seasonal maintenance, according to Reuters estimates based on data from industry sources.
As much as 4.635 million metric tons of Russia’s refining capacity is expected to be offline this month, industry sources have told Reuters.
Russia’s authorities are also recommending refineries curb exports and sell more fuel domestically to meet local demand, but the recommendation is not legally binding, according to Bloomberg.
Lower diesel shipments overseas would mean lower export revenues for Russia, which continues to earn billions of U.S. dollars each month from exports of crude and products.
Russia’s crude oil and refined products exports remained steady at some 7.3 million bpd in July, while higher oil prices and narrower price differentials for Russian crude pushed Moscow’s revenues higher compared to June, according to estimates by the International Energy Agency (IEA) in its market report in August. Russia’s export revenues, at $15.3 billion in July, rose by $2.5 billion from June, but they were $4.1 billion lower compared to July 2022, the agency’s estimates showed
This week saw a series of big-ticket funding rounds for biotech companies, with Apollo Therapeutics and Nimbus Therapeutics both pulling in upwards of $200 million, in a positive sign for private financing sentiment.
Top of the table was the $226.5 million Series C for Anglo-US company Apollo Therapeutics led by Patient Square Capital, which adds to its earlier $195 million in financing and will be used to license additional drug candidates, as well as push existing programmes through development.
Apollo calls itself a "hub-and-spoke" biotech, identifying promising drug leads in academic institutions and licensing them for further development. At last count it had more than 20 candidates on its books, and the cash injection enables it to take its "most advanced programmes to key clinical value inflection points," according to chief executive Richard Mason.
The round included a number of new investors, including M&G plc and two of the largest US public pension plans, along with existing investor Rock Springs Capital.
Computational chemistry specialist Nimbus Therapeutics, meanwhile, collected $210 million in financing to support the development of its small-molecule medicines, headed by NDI-101150, an HPK1 inhibitor for treating solid tumours in a phase 1/2 trial, and preclinical-stage candidates for Werner syndrome helicase (WRN) and an undisclosed autoimmune disease target.
The round – co-led by new investor Google Ventures and existing backers SR One and Atlas Venture – adds to a massive $4 billion pocketed by the Massachusetts biotech after Takeda bought its TYK2 programme for psoriasis and other inflammatory diseases earlier this year. Other participants included Bain Capital Life Sciences, BVF Partners, Gates Frontier, Lightstone Ventures, Pfizer Ventures, RA Capital Management, and SV Health Investors.
Mariana Oncology pulled in $175 million in a Series B led by Deep Track Capital and Forbion to help advance its pipeline of precision radiopharmaceuticals into the clinic. Lead candidate MC-339 is due to start human trials in 2024 in small cell lung cancer (SCLC). The drugs are peptide-based molecules designed to penetrate into tumour tissue more effectively than current antibody-based radiopharma therapies.
Atlas Venture, Access Biotechnology, RA Capital Management, and new investors Eli Lilly, Nextech Invest, and Citadel's Surveyor Capital also took part in the round, which follows a $75 million Series A for the Massachusetts biotech in 2021.
South San Francisco-based Star Therapeutics added $90 million to its cash pile with a Series C led by Sofinnova Investments that takes the total raised by the antibody therapy developer to more than $190 million. Proceeds will support the clinical development of VGA039 - a first-in-class antibody that is currently being tested by Star's Vega Therapeutics subsidiary in a phase 1a/1b study for inherited bleeding disorder von Willebrand disease – as well as other companies in Star's portfolio.
New backers included Qatar Investment Authority, Catalio Capital Management, Agent Capital, Soleus Capital, and NYBC Ventures, with existing investors Westlake Village BioPartners, OrbiMed, Redmile Group, RA Capital Management, New Leaf Venture Partners, Cormorant Asset Management, and Cowen Healthcare Investment also taking part.
French start-up Corteria Pharma has just completed its first round – raising €65 million (around $71 million) – that will be used to fund early trials of a trio of heart failure drug candidates, including two in-licensed from Sanofi.
Corteria was founded in 2021 by two former Sanofi execs, Philip Janiak and Marie-Laure Ozoux. Its lead candidate is a once-daily subcutaneous CRF23 agonist that is scheduled to start clinical trials early next year, with a once-monthly follow-up and an arginine vasopressin-targeting antibody following after.
The Series A was co-led by new investors Jeito and Orbimed, with participation from existing investors Kurma Partners, Fountain Healthcare Partners, V-Bio Ventures, Invivo Capital, and Omnes Capital.
Finally, San Diego's Tentarix Biotherapeutics raised $35 million in a Series B led by Amplitude Ventures, with participation from Gilead Sciences and founding investors Versant Ventures and Samsara BioCapital.
The funding comes hard on the heels of a $66 million upfront licensing deal with Gilead and will support the development of its Tentacles drug discovery platform, based on protein therapeutics that target multiple, specific proteins on the surface of cells, but are only active when all are present. Since it emerged in 2021, the biotech has raised $132 million
Congress needs to get tough with Biden administration officials who ignore legitimate requests for information concerning Covid-19, the pandemic that killed more than1.1 millionAmericans.
Many unanswered questions remain about the origins of the virus and the government’s response to the pandemic. While Congressional investigators, especially in the House of Representatives, have been doing an outstanding job, Biden’s officials have nonetheless stymied numerous efforts to secure crucial information on the pandemic. Here are just a few of the many examples:
First, despite Congress unanimously enacting the Covid-19 Origin Act of 2023, which statutorily required the Biden administration to declassify “any and all” information related to the activities of the Wuhan Institute of Virology, the research role of the Chinese military, and initial illnesses of research scientists, the Biden administration has failed to comply.
Under the statute, the only redactions allowed in the report were to protect intelligence “sources and methods.” After missing a June 18 deadline for the delivery of the report, Avril Haines, director of National Intelligence, sent Congress a “paltry” 5-page report on June 23, plus a cover page and a glossary of terms that failed to provide the information required by the statute. On June 27, the law’s authors, Senators Josh Hawley (R-Mo.) and Mike Braun (R-Ind.) demanded that Haines deliver the legally required information within seven days, writing that: “This half-baked effort falls woefully short of the statutory requirements and undermines congressional intent.” In response, Haines told the Senate authors of the law that her scanty report met the spirit and letter of the law. It did not.
Secondly, the Department of Health and Human Services has failed to provide information about Dr. Anthony Fauci’s February 1, 2020, memo to top HHS officials concerning his discussions with top virologists and the origins of the pandemic. Fauci’s memo then confirmed his personal knowledge that “gain of function” experiments — dangerous research designed to enhance the transmissibility and virulence of pathogens — were being conducted at the Wuhan Institute of Virology in China.
On July 13, 2023, Rep. Brad Wenstrup (R-OH), Chairman of the House Select Subcommittee on the Coronavirus Pandemic, requested Xavier Becerra, Secretary of the U.S. Department of Health and Human Services (HHS) to provide all related information concerning Fauci’s February 1, 2020, memo (internal talking points, notes, and any other relevant documents). Wenstrup requested delivery of the information by July 27, 2023, but as of this writing, there has still been no response.
Third, the Department of Justice, unsurprisingly, has also been unresponsive. Senator Rand Paul (R-KY.) has repeatedly requested the Department to conduct an investigation into whether Dr. Anthony Fauci committed perjury in his May 2021 Senate testimony concerning the origins of the coronavirus. The key issue is whether any federal funds, dispensed by Fauci’s National Institute of Allergies Infectious Diseases (NIAD) or any other agency, were used to finance “gain of function” research in China. Under oath, Fauci doggedly denied that there was any federal funding of gain-of-function research in Wuhan.
At the time, Senator Paul found neither Fauci’s wordy explanations nor his heated denials persuasive. And since, further reporting has revealed that certain Chinese research institutions received over $2 million in federal funds over a 7 year period, including the Wuhan Institute of Virology (WIV), which was engaged in gain-of-function coronavirus research. The Institute was a subcontractor of EcoHealth Alliance, a firm that had received substantial American taxpayer funding from the National Institutes of Health (NIH).
On July 21 , Sen. Paul requested the Justice Department to open an investigation into the truthfulness of Fauci’s sworn testimony. Attorney General Merrick Garland ignored that request. On July 14, 2023, Sen. Paul renewed his request, and in his second letter, he cited Fauci’s awareness of dangerous “gain of function” research in Wuhan and NIAD’s documented funding of China’s research into “artificial viruses able to infect human cells”. No response. Finally, Sen. Paul sent a third letter (August 8, 2023) to Matthew Graves, U.S. Attorney for the District of Columbia, citing this circumstantial evidence, and asking him to initiate an investigation. And as of this writing, there has still been no response.
Fourth, on March 28, 2023, Rep. Wenstrup asked Dr. Rochelle Walensky, then Director of the Centers for Disease Control and Prevention (CDC), for documents related to the agency’s actions regarding its guidance on schools’ reopening and potential political interference. American schoolchildren were severely damaged by mandatory school closures during the pandemic and it is worth asking to what extent federal government guidance was dictated by external political considerations.
Walensky ignored this request. On June 1, 2023, Wenstrup again asked for the documents, and Walensky only delivered documents that were already in the public domain under the Freedom of Information Act (FOIA). In his third letter to Walensky on June 28, 2023, Wenstrup once again asked for the relevant documents, including phone records and text messages between her and Randi Weingarten of the American Federation of Teachers (AFT). Upon sending, Wenstrup remarked: “The Department of Health and Human Services is continuing its pattern of obstructing Congress by apparently only producing documents already made publicly available via the FOIA.”
Finally, the most recent example of the Biden administration ignoring Congress comes courtesy of a top NIH official, who used private emails to hide Covid-related information from the public. Sen. Ron Johnson (R-WI), ranking member of the Senate Permanent Subcommittee on Investigations, recently revealed that Dr. David Morens, a senior advisor to Fauci, used his personal email account, rather than his government account, in an apparent attempt to evade requests for information concerning Covid-19 under the Freedom of Information Act (FOIA). Because of unsatisfactory NIH internal probes, Johnson asked the Inspector General of the Department of Health and Human Services (HHS) to investigate the matter. In his August 14, 2023, letter to HHS Inspector General Christi Grimm, Johnson stated: “NIH, which includes NIAD, also appears to have engaged in the destruction of federal records. According to a whistleblower allegation made public on February 22, 2022, NIH has allegedly instructed staff to destroy records, in particular records related to the Wuhan Institute of Virology (WIV).” Grimm responded by saying that she would neither “confirm nor deny” the existence of any ongoing investigations.
Enough is Enough. Congress has the sole responsibility to legislate on behalf of the American people, and its Constitutional power to legislate includes its right to secure information on any topic within its legislative jurisdiction. Congress’s greatest Constitutional power is its power of the purse: its authority to fund or withhold funding of the agencies and operations of federal agencies and compel their compliance with information requests. To stop this non-sense and make the Biden administration answer crucial questions, lawmakers can take three actions.
First, cut federal appropriations to noncompliant agencies and departments of the federal government. For noncompliance, or pending compliance, with congressional requests for information, appropriators, for example, can cut funding for an agency’s office of the Director or Secretary, salaries for political appointees or travel budgets or any public relations contracting, or even zero out funding for the agencies’ legislative affairs or public affairs offices.
Second, invoke the “Holman Rule”. This is a special rule of the U.S. House of Representatives that would permit amendments to House appropriations bills to reduce or eliminate the salary of specific federal officials. Rooted in the nineteenth century, the House of Representatives has not consistently maintained the Holman Rule as standard House rule. In 2019, for example, House Democrats abolished it. In 2023, House Republicans revived it. It is time to invoke it.
Third, place “holds” on Presidential nominees to department or agency positions. Under Senate rules, a Senator can place a “hold” on a nominee by telling the Senate majority or minority leader of the Senator’s objection to Senate approval by unanimous consent. When applied to a particular agency, affecting all the agency’s nominees, a Senator’s hold is called a “blanket hold”. To break a Senate “hold” on the approval of a nominee requires a “cloture” vote, a time-consuming process that eats up precious Senate floor time.
Team Biden’s behavior follows a pattern. When administration officials ignore, delay, or deny legitimate congressional requests for information, they subvert the right of our democratically elected representatives to fulfill their legislative responsibilities. Worse still, they deny the American people’s right to know what happened during the pandemic that took so many of their lives. It’s time for that to change. Congress should take more direct and aggressive actions until the Biden administration complies.
Robert E. Moffit, PhD., is Senior Fellow in Health and Welfare Studies at the Heritage Foundation. Kyle Brosnan, JD, is Chief Counsel for the Heritage Foundation’s Oversight Project.
Leading into the Labor Day holiday weekend, officials in Washington kicked off Medicare's new Drug Price Negotiation Program by naming the first 10 medications to be included. Roughly two-thirds of non-dual eligible Medicare beneficiaries live with multiple chronic conditions. For these patients, many of whom rely on prescription drugs to manage their health, the impacts of the new program could be considerable.
These unprecedented negotiations between the federal government and drug makers, authorized in last year's Inflation Reduction Act, will fundamentally alter Medicare's "Part D" prescription drug benefit – in obvious and not-so-obvious ways.
The Inflation Reduction Act requires officials to select drugs that cost Medicare the most money in total – even if the medicines don't cost beneficiaries that much out-of-pocket. In other words, the law doesn't necessarily target the priciest medicines; rather, it targets widely prescribed ones.
Spending is a function of both price and volume – or how many drugs are sold because of the number of people using them. That raises the question of how patient access will change in the push to save Medicare money.
The list of 10 drugs includes a blood thinner that costs Medicare $370 per month per patient, and an insulin that costs less than $280 a month. They likely made the list not because they are especially expensive, but because of the large number of Medicare beneficiaries who take them.
The IRA could have ensured continued access to these drugs for Medicare beneficiaries with minimal out-of-pocket costs by prohibiting Part D insurance plans from implementing restrictive coverage policies like non-preferred and specialty formulary tier placement, higher cost-sharing, prior authorization, or step therapy requirements. But it didn't.
That failure could have profound consequences. The alignment of incentives among Medicare itself, insurers and their pharmacy benefit managers, and patients and their doctors has been substantially disrupted.
Neither the IRA nor the Administration's implementation of the law will prevent insurers and PBMs from bumping drugs in the Price Negotiation Program into higher cost-sharing tiers on insurance formularies. That means patients' out-of-pocket expenses for each prescription could skyrocket, even as government costs go down.
Meanwhile, to boost their own profits, insurers and PBMs may adjust their formularies to cover comparable but less popular treatments that are currently just as expensive on lower cost-sharing tiers. That's great for PBM bottom lines. But it will create huge disruptions in access.
Patients with chronic conditions who are succeeding on their current drug regimen may face IRA-induced financial pressure to switch medications, with potentially serious health consequences. That's especially true for patients dealing with two or more chronic conditions, where finding the right combination of medications is a matter of both clinical art and science.
More than half of the people Medicare covers live with three or more different chronic conditions. Shifting away from medications that are working to other possible treatments and combinations is risky and should not be necessary. Yet there's ample reason to think the IRA is setting the stage for just that.
In fact, the Congressional Budget Office (CBO) prepared an estimate projecting changes in utilization rates for a similar drug price negotiation program that preceded the IRA. To achieve expected savings under the program, the score estimated reduced utilization for some medications of more than 25 percent. This disruption to access has no medical justification.
Price negotiations will also have a chilling effect on drug research – and thereby diminish the number of new medicines available to patients in the years and decades to come. One recent study from Vital Transformation estimates that over the next decade, the IRA's drug price negotiations will result in 139 fewer medicines being developed.
With no basis in medical science, the IRA also favors research into medicines administered in a doctor's office over the pills, patches, and capsules people can pick up at a pharmacy and take at home. Many of the most promising cancer treatments fall into the latter category of "small-molecule" drugs – a clear policy contradiction to President Biden's "Cancer Moonshot" goal to reduce cancer deaths by half in the next 25 years.
The IRA's incentive structure is already steering research dollars away from areas of greatest unmet medical need and preferred routes of administration. And due to the price-popularity nexus in selecting drugs for price negotiations, the IRA actually discourages development of treatments that would benefit Medicare patients in large numbers.
Research into rare diseases will also suffer. The IRA's drug selection provisions disincentivize research that would allow approved rare-disease treatments to be used to treat additional disease states.
Judging the success of the IRA's drug-pricing program requires looking not just at prices, but also at its impact on access to treatments and the far-reaching shifts in research and development decision-making and investment it induces.
This ‘holiday’ announcement is cause not for celebration, but for concern.
Kenneth E. Thorpe is chair of the Department of Health Policy and Management at the Rollins School of Public Health, Emory University. He is also chairman of the Partnership to Fight Chronic Disease.
In this series, “Promise or Peril: Alarming COVID-19 mRNA Vaccine Issues,” we explore how the introduction of mRNA technology lacked an adequate regulatory framework, setting the stage for serious adverse events and other concerns related to inadequate safety testing of lipid nanoparticles, spike protein, and residual DNA- and lipid-related impurities, as well as truncated/modified mRNA species.
Previously: In Part 1, we introduced how the U.S. Food and Drug Administration (FDA) relaxed the rules for mRNA vaccines compared to mRNA therapies and discussed the available data regarding LNP distribution throughout the body based on animal testing, the fact that human testing was not done, and the lack of mRNA or spike protein biodistribution data. In Parts 2 and 3, we explored how the LNPs are constructed and how they behave in the body and affect health.
Now we turn to another problem—the cargo contained in the LNP capsules: the mRNA and its encoded spike protein. We introduce the inflammatory response to the spike protein and one of its subunit proteins and how they may contribute to serious adverse events such as myocarditis and blood clotting.
Rochelle Walensky, former director of the U.S. Centers for Disease Control and Prevention (CDC), stated on “Good Morning America” in June 2021 that myocarditis cases are “really quite rare … minor, self-limited, they generally resolve with rest and standard medications.” However, this assertion was made based on a preliminary review of 300 cases and before conducting long-term follow-up.
A study published on Aug. 1 followed 40 adolescents in Hong Kong for up to a year. Follow-up testing performed in 26 patients with initial abnormal findings revealed that 58 percent of those with vaccine-associated myocarditis had persistent heart muscle scarring. The authors concluded: “There exists a potential long-term effect on exercise capacity and cardiac functional reserve during stress.”
This series demonstrates how exposure to the spike protein results in downstream cardiovascular issues. Given that vaccination causes the body to produce more spike protein, it is clear that additional research was needed to understand the health impacts of vaccination prior to licensure.
Summary of Key Facts
The SARS-CoV-2 spike protein and its S1 subunit have known impacts on the cardiovascular system, such as an increased risk of blood clotting.
The vaccine-induced spike protein and its S1 subunit have been found in the blood following vaccination.
In lab studies, the spike protein activates white blood cells and may trigger an inflammatory response or clotting.
Free spike protein was found in the blood of adolescents and young adults with post-mRNA vaccine myocarditis but not in healthy control subjects without myocarditis.
The S1 subunit can interact with ACE2, platelets, and fibrin and may be what leads to an inflammatory response driving serious adverse events, including clots, myocarditis, and neurological problems.
As discussed in Part 3, lipid nanoparticles (LNPs) act as adjuvants, stimulating the immune system. This innate immune response peaks within six hours of vaccination and returns to baseline by about day nine, temporally corresponding to the onset of myocarditis, which typically occurs within the first seven days following mRNA COVID-19 vaccination.
Studies have not been done to evaluate how vaccination affects those who have already been infected with SARS-CoV-2.
The spike protein was implicated in small vessel microclots during COVID-19 illness; thus, postvaccination cardiovascular effects should have been anticipated.
The first deadline for FDA-mandated post-authorization safety studies has passed, yet to the best of our knowledge, the full report has not been made available to the public.
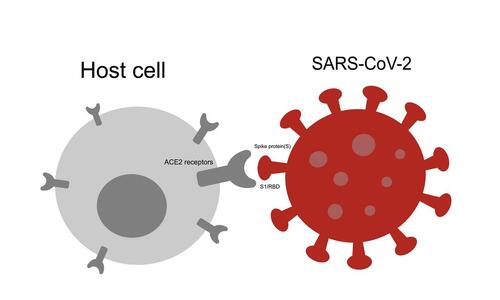
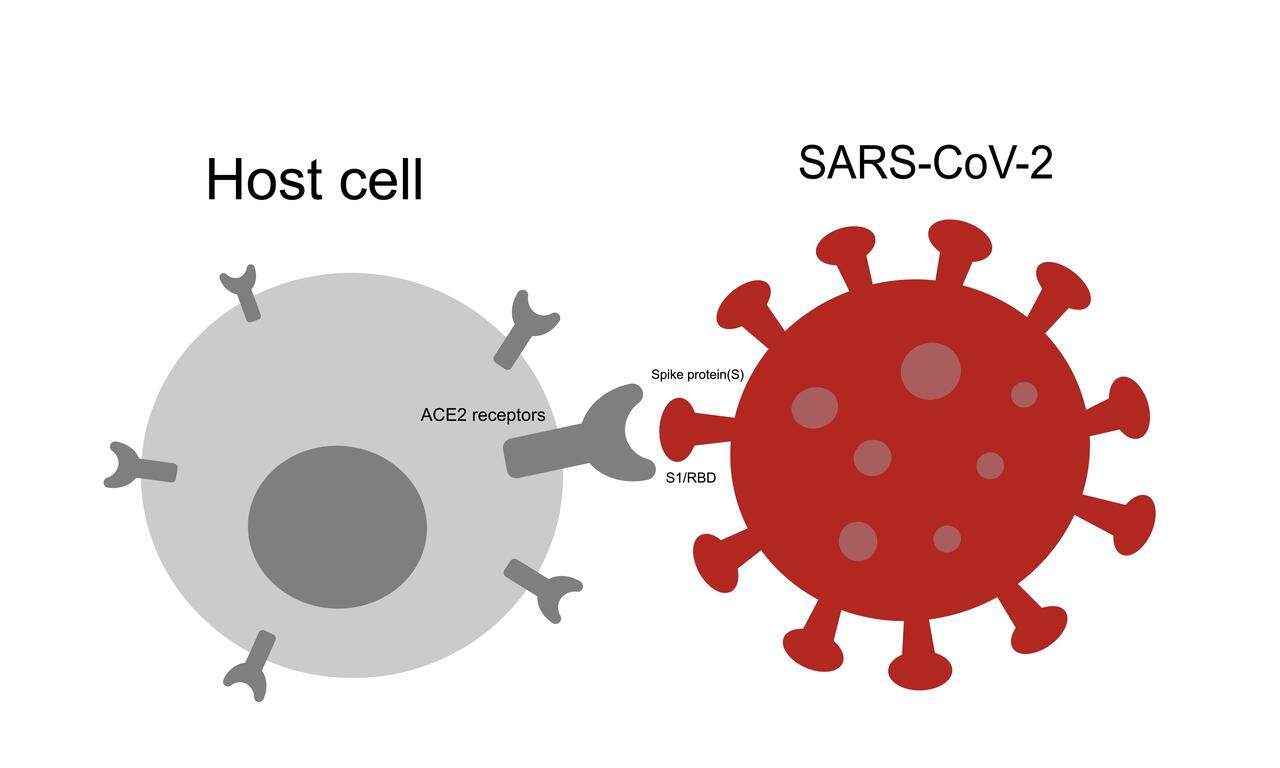
The spike protein protrudes from the SARS-CoV-2 virus like a crown of sticky handles. The job of the spike protein is to grab onto the ACE2 receptor so the virus can enter the cell. The ACE2 receptor is found in many human cells in the lungs, kidneys, gut, heart, and the lining of the blood vessels.
Spike protein is comprised of two parts: the S1 and S2 subunits. The S1 subunit protein sits at the tip of the spike protein and is responsible for attaching to the ACE2 receptor. Once bound to the receptor, the spike protein changes shape to allow the virus to enter. Having accessed the inside of the cell, the SARS-CoV-2 virus uses the cell’s own protein manufacturing process to make new viral proteins.
Effective vaccines select recognizable antigens that induce a robust immune response. The spike protein was chosen for the mRNA COVID-19 vaccine because it is responsible for attaching to cells and gaining entry. However, research suggests that the spike protein and its S1 subunit may also be responsible for cardiovascular complications following both infection and vaccination.
The S2 subunit may also interfere with tumor suppression, potentially explaining why COVID-19 can be more severe for cancer patients.
(Jaitham/Shutterstock)
Research shows that the spike protein is found in the blood following COVID-19 infection and vaccination. The spike protein modifies blood clotting and can stimulate an overactive immune response. A better understanding of these findings and the specific roles the spike protein and its S1 subunit play will help us determine who is most at risk for severe disease or vaccine adverse events.
Cardiovascular Effects of Spike Protein Following Infection
Although the studies are small, the spike protein has been found in the blood and clots of severely ill COVID-19 patients. The clinical evidence suggests a fingerprint of the spike protein’s cardiovascular effects.
In a study of 41 patients published in Frontiers in Immunology, 30.4 percent of the 23 hospitalized were found to have significant levels of spike protein in their circulation. None of the remaining 18 uninfected or mildly ill individuals had circulating spike protein.
A small case-control study detected the spike protein in clots retrieved from COVID-19 patients with acute ischemic stroke and myocardial infarction.
Another study detected the S1 subunit in the plasma of 64 percent of COVID-19-positive patients, and S1 levels were significantly associated with disease severity. The nucleocapsid (N) protein, a marker for COVID-19 infection, was also detected. The authors speculated that the presence of S1 and N in plasma suggests that virus fragments enter the bloodstream, potentially due to tissue damage.
The exact chain of events is not fully understood. Still, laboratory, clinical, and biopsy findings offer converging evidence suggesting a role for the spike protein and its S1 subunit in blood clotting and heart injury.
Blood Clots Associated With Spike S1 Subunit
In laboratory experiments like those performed in the Frontiers in Immunology study, the spike protein S1 subunit causes a chain reaction that sets up the right conditions for clots to form. In this chain reaction, the S1 protein binds to the ACE2 receptor on the cells lining the blood vessels. Binding to ACE2 then activates immune cells.
This domino effect can also stimulate platelet binding, increasing clotting risk. Platelets are essential clotting agents that stop blood loss following injury by clumping together. The authors further noted that in vitro, “our group recently documented that exposing sera from severe COVID-19 patients to endothelial cells induced platelet aggregation.”
In other words, the S1 subunit is of interest because, in vitro (in a test tube), it appears to cause changes to clotting mechanisms. If the S1 subunit can affect clotting agents like fibrin, complement 3, and prothrombin, this may be a mechanism through which SARS-CoV-2 can cause cardiovascular complications. Clotting causes changes in blood flow, potentially leading to thrombosis, stroke, and heart attack.
Atypical Blood Clots
Providing blood thinners to decrease the risk of clot formation did not appear to reduce the clotting risk in COVID-19 inpatients or outpatients. This may be because the clots formed after exposure to the S1 subunit may not be typical blood clots. Three findings suggest that the S1 subunit is important to clotting risk.
1. Clots Resist Normal Breakdown
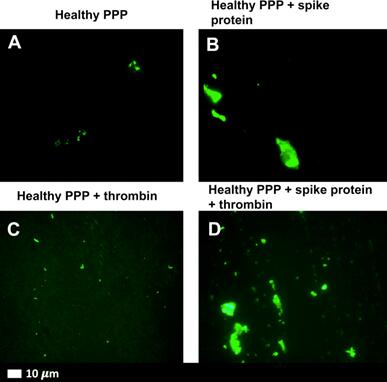
First, when the S1 subunit was added to healthy blood in the lab, it created dense, fibrous clot deposits. These fibrous “amyloid” clots formed even when blood taken from healthy people was exposed to the S1 subunit.
The S1 subunit appears to be associated with clotting resistant to fibrinolysis—the normal breakdown of clots necessary to restore blood flow after injury. These amyloid clots are shown in Figure 1 below.
Amyloid clots occur when a protein is damaged and begins to fold abnormally on itself. When these abnormal amyloid proteins accumulate in the body, they can interfere with normal function.
Figure 1. Amyloid Clots Formed in Response to Spike Protein S1
Figure 1. Amyloid clots formed in response to spike protein S1. (National Center for Biotechnology Information)
2. S1 Subunit Can Induce Amyloid Substances
Second, these dense clots may be caused by certain protein segments on the S1 subunit. The spike protein has seven protein segments (peptides) that can induce fibrous (amyloid) substances. While the fully intact spike protein (S1 and S2 subunits attached to form the full spike) did not form this amyloid, the S1 subunit did. This finding is interesting because it suggests that the subunits of the spike protein may have unique effects on cells.
3. Spike Blocks Other Clot-Inhibiting Proteins
Third, spike protein can outcompete other proteins, which prevent clots from forming. In another laboratory experiment designed to understand how this process plays out, scientists found that the spike protein blocks proteins important to breaking down clots.
In summary, the in vitro (laboratory-based) research suggests that the spike protein subunit S1 can induce clot formation and impair clot dissolution. While we do not know precisely how this translates to processes in the body, Epoch Times’ Jan Jekielek explored clotting and the role of spike protein with pathologist Dr. Ryan Cole on June 3 and Dr. Paul Marik on May 23. In the interview, Dr. Cole explained that the spike protein persists in the body longer, inflames tissues wherever it lands, and acts as an irritant or toxin in the body.
Spike Protein Found in COVID-19-Vaccinated Myocarditis Patients
Studies of COVID-19-vaccinated patients diagnosed with myocarditis found spike protein in the patients’ blood and heart muscles but not in those without myocarditis.
It is unclear why the spike protein was circulating freely or unbound by antibodies. The adolescents who developed myocarditis had similar immune markers to those who did not develop myocarditis. In other words, the group with myocarditis did not appear to have any immune problems.
Rather, these adolescents may have had an overactive natural immune response. Strong natural (“innate”) immunity helps the body fight off disease without any prior exposure. However, the first responders (inflammatory cytokines) can sometimes be exuberant. If the innate immune response overreacts, it may trigger myocarditis.
Found in Heart Muscle
The spike protein coded by mRNA has also been found in heart muscle cells. An endomyocardial (heart muscle) biopsy study was conducted among 15 patients with myocarditis following vaccination. No other viral infection could be found that might have caused the myocarditis.
The investigators found SARS-CoV-2 spike protein in nine of the 15 patients. Immune cells (CD4+ T) were also detected in the biopsy samples. These observations suggest an inflammatory reaction to the spike protein.
The authors concluded: “Although a causal relationship between vaccination and the occurrence of myocardial inflammation cannot be established based on the findings, the cardiac detection of spike protein, the CD4+ T-cell-dominated inflammation, and the close temporal relationship argue for a vaccine-triggered autoimmune reaction.”
A 2022 modeling study also suggests that the spike protein can cause an autoimmune response by mimicking human molecules, causing antibodies to bind to “self” proteins.
Spike S1 Detected in the Blood of Vaccinated Adults
Another study found that 11 of 13 adults vaccinated with Moderna’s mRNA-1273 had the S1 subunit in their blood as early as one day after vaccination.
Plasma was collected from 13 participants at various times during the first month after each dose. The antigens S1 and spike were measured to estimate the amount of mRNA translation into protein products.
After the first 100-microgram dose, S1 antigen was detected in the plasma of 11 participants. In contrast, the spike antigen was detected in three of 13 participants. The S1 antigen peak was detected on average five days after vaccination. Again, the timing of this peak for S1 seems to add to the clues suggesting an autoimmune response in the week after vaccination.
mRNA Detected in the Blood and Lymph Nodes After Vaccination
Vaccine mRNA, which encodes the spike protein and its S1 subunit, also persists in the blood and lymph nodes. Following vaccination, spike-encoded mRNA has been found in the blood for 15 days and in lymph nodes for up to 60 days. Spike-laden exosomes have been found circulating in the blood for up to four months. This finding is important because it refutes the CDC’s claim that the mRNA is so fragile that it dissolves quickly at the injection site (see Figure 2a in Part 1).
The lymph nodes continue creating better-fitting antibodies after any viral infection. This is a critical way that our bodies prepare for new variants naturally. However, persistently high levels of vaccine-induced mRNA and spike protein may not be helpful when the immune system is asked to respond to future variants. In other words, if the immune system is tasked with continuing to pump out antibodies to a previous variant, it may be less nimble when asked to create a high-quality antibody for a new variant.
Given what we know about the harmful effects of the SARS-CoV-2 virus, we should not have assumed that the vaccine-encoded spike protein would be harmless.
And, given what we know about clotting issues following COVID-19 infection, future studies should test whether the S1 subunit produced in response to vaccination can also cause clotting issues via the same pathway. These studies should include both lab experiments and human observations.
In addition, we do not know the relative amounts of free spike protein in circulation following infection versus vaccination.
In the case of the COVID-19 vaccines, the active ingredient was not studied prior to authorization. The manufacturers used mRNA that encodes for a substitute protein (luciferase) to test the safety and biodistribution of the mRNA vaccines.
Pfizer submitted animal biodistribution data to regulatory agencies using the surrogate RNA encoding for luciferase, as discussed in Part 1 of this series.
However, these studies were inadequate in describing how mRNA, the spike protein, its S1 subunit, and the LNP carrier would affect the human body.
In this article, we described laboratory findings showing clotting associated with the S1 subunit. Studies like these reinforce why thorough preclinical studies are so crucial. The studies conducted by pharmaceutical companies were not sufficient to address these questions.
We had very little information about how people would respond to vaccination depending on age, sex, immune status, overall health, or history of prior SARS-CoV-2 infection. The original clinical trials did not enroll enough people who had already recovered from COVID-19; they were not designed to provide an understanding of how prior infection would affect a person’s response to vaccination.
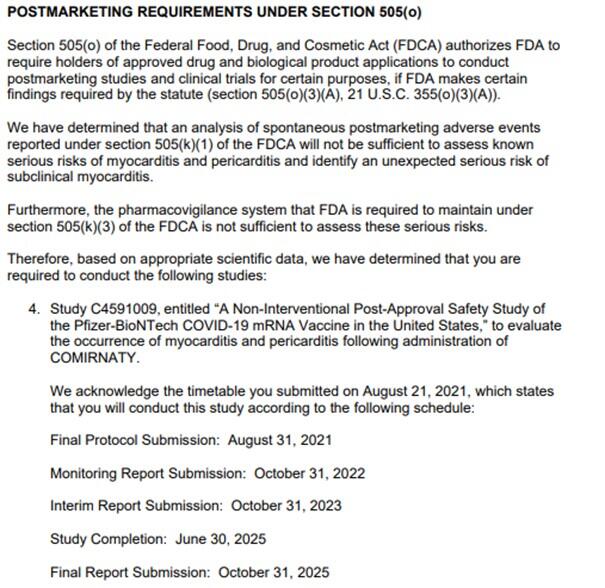
Required Pfizer Post-Authorization Safety Study Unavailable to Public
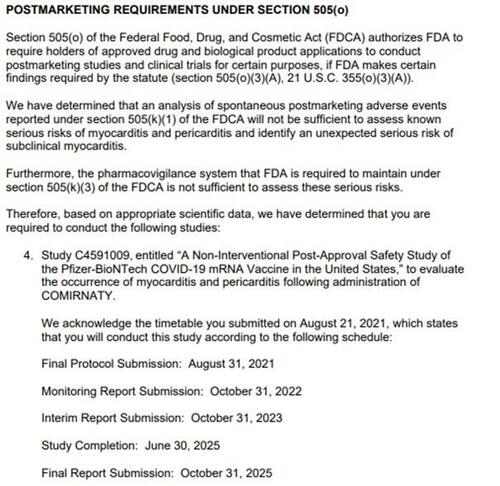
Pre-authorization studies were clearly inadequate. Post-authorization, the FDA has only acknowledged that passive surveillance is insufficient to establish safety. The agency responded to adverse event reports by requiring Pfizer to conduct additional studies, with the first monitoring report due October 2022.
“We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
“Furthermore, the pharmacovigilance system that the FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks. Therefore, based on appropriate scientific data, we have determined that you are required to conduct the following studies. …”
Has the FDA received the monitoring report from Pfizer, which was due by Oct. 31, 2022? The next report, the interim report, will be due in October.
Figure 2. FDA Postmarketing Safety Study Requirements
FDA BLA Approval Letter, Aug. 23, 2021. (U.S. Food and Drug Administration)
Next: In Part 5, we will discuss the mRNA manufacturing issues affecting contamination with double-stranded DNA and the potential for genome integration.




{kind=link}
{kind=link}
{kind=link}