by Alan Cassels
To fully grasp the spectacle of modern disease mongering, let’s riff on the latest and pudgiest kid on the block: fatness. Here’s a handy image to help grasp pharma’s marketing message: visualize a big, obese pro wrestler, but mean and scary looking, because corporate America is trying to sell you the idea that being overweight is mean and scary.
But one caveat: the image in your head can’t be a real wrestler, but a fake one dressed up in a Sumo costume, so the person looks like a children’s cartoon version of someone sick and unhealthy. You might find this marketing ploy confusing, but being oversized is a disease that wins oversized attention from drug manufacturers who’ve found that the gargantuan size of the injectable weight loss drug market is big, malleable, and easily manipulated.
It wins my attention because it is so utterly mockable, where the jokes come unprompted once you realize these weight loss “breakthrough drugs” are just diabetes medicines repurposed to net billions in Big Pharma profits.

Drug makers rarely cure disease, but they show a profound level of professional expertise in selling sickness. Selling you the science that excess fat is definitively lethal and a precursor to heart disease, cancer, diabetes and early death required insightful market analysis, human psychology research, and refining the art of physician schmoozing. Old-fashioned fat-shaming can only sell a limited number of scripts.
Modern fat-mongering deploys a pharma-fuelled fear machine with industry-sponsored guidelines, gullible media, complicit psychologists, as well as promoters, pimps and pushers in all medical specialties including endocrinologists, cardiologists, and even dermatologists (because everyone wants to look "healthier").
Think Top Gun. Yup, everyone’s getting into the cockpit to fly that hypersonic fear machine into the danger zone!

Obedient journalists have always been pharma’s best marketers. In the past, a drug pitch sometimes caused a gag reflex. Now corporate messages wash down like a shot of Jack Daniels before they start typing.
Case in point: Canada’s national newspaper, the Globe and Mail has hopped on the fat-mongering gravy train, hosting a half-day session on the obesity “epidemic.” Of course, the only epidemic these days is legacy media’s gluttony around headlines with the term “epidemic.”
But I digress.
Norvo Nordisk got the Globe and Mail’s André Picard, the guy some consider Canada’s most highly decorated health reporter, to pimp WeGovy. But let’s face it, Novo is rolling in so much excess money, they can buy whomever they like.
One such guy that has already sold his soul to fat-lowering drug makers is Picard’s co-panelist Dr. Arya Sharma. Based on public disclosures, Sharma has reported receiving payments from companies including Novo Nordisk (makers of Ozempic, Wegovy, and Saxenda), Eli Lilly, Boehringer Ingelheim, Currax, Johnson & Johnson, Allurion, Aidhere, Medscape, MDBriefcase, Oviva, and Xenobiosciences. I’m sure he’d say he’s “independent” yet when a “Thought Leader” like Arya Sharma pockets honoraria from a laundry list of pharma companies pushing weight-loss drugs it’s tough to swallow the “independent” claim without giggling.
It's also the kind of pharma relationship Mr. Picard would have criticized in the past.
Speaking of the past, and “independence” I remember 30 years ago when André actually wrote copy that criticized the pharmaceutical industry’s marketing tactics. But now our eminence grise is being paid for an afternoon pretending he’s moderating a “scientific” discussion.
Oh, how the mighty have fallen, not to mention getting plumper on the golden goose. At the bottom of the webpage for the Globe and Mail’s Novo Nordisk marketing event, Novo Nordisk runs a final ad, followed by a Globe and Mail ad that asks readers to “support quality, independent journalism.”
Who is marketing whom?

Drug companies are not just selling weight loss anymore; they’re selling salvation. Novo’s Wegovy is a GLP-1 inhibitor, other brands include Ozempic and Mounjaro. Drug companies along with friendly reporters like Andre Picard promote these drugs for shedding pounds as well as supposed “downstream health benefits” like reducing heart attacks. The science behind these claims might not be solid, but economics drive real profits that cannot be disputed making Novo and Eli Lilly mind boggingly rich.
Novo Nordisk is headquartered in a Copenhagen suburb and its market capitalization of $570 billion currently exceeds the entire Danish GDP.
The Globe and Mail/Novo Nordisk event reports that “in 2022, approximately 30 per cent of adults in Canada were living with obesity.” I have to apologize for the awkward wokeness of the Canadian language. We no longer have hypertensives, diabetics or obese people, we have people “living” with hypertension, diabetes and obesity. The Globe maintains that “access to care is hampered by stigma and a long-held view that obesity is a lifestyle choice versus a chronic illness.” Bingo!
The crappy food that corporations sell causes a chronic disease that other corporations now cure! Medicine can save us while the markets rejoice.
Picard and his corporate friends will discuss “leverage” or how “Canada can leverage its private sector and implement programs and policies to help prevent and treat obesity for a healthier nation.” Since Novo is funding this adventure, the leverage is clear: Novo will leverage the Canadian government to drive patients onto the Novo teat, hoping that WeGovy is their path to salvation.
So, let’s stop eating this nonsense for a second and consider a few reasons why we all need to fast from all the fat-mongering:
1. Repeat after me: Being Overweight Is Not a Disease. Period.
What happened to the days when we accepted that people come in different shapes and sizes? Definitions of diversity and inclusion don’t include big fat people, because THOSE people need reminding that their diversity is pathological and they need to do the right thing and consider high tech injectable weaponry.
The reality is that weight indices are a terrible predictor of health. We learned this over the last 40 years with the grossly inappropriate use of the term “Body-Mass Index” or BMI, a fiction which is still being used to push the idea that one can formulate health based on height and weight, and then use that number to beat everyone senseless.
A 2012 JAMA study showing metabolic health discrepancies (e.g., 50% of overweight and 30% of obese individuals being metabolically healthy) across BMI categories is good proof that the BMI, as a way to diagnose or classify “healthiness” is a dud. Let’s be frank: there are also very thin and fit-looking people who drop dead of heart attacks or cancer.
This research was followed in 2016 by a study in Nature showed that 30% of people classified as obese by BMI had normal body fat percentages when measured by DEXA scans. Additionally, many overweight people also happen to have good cardiovascular systems, perfect cholesterol and blood pressure, who then live long and healthy lives.

Real Sumo Wrestlers are very big dudes, such as the legendary Japanese heavyweight Yamamotoyama (pictured here) who weighed in at 584 pounds and yet, by all accounts, was a pretty healthy guy despite a BMI that was clearly off the charts. Seems like it wasn’t his weight that made him stop Sumo wrestling. (he was caught match fixing—oopsie—and asked to quit). This guy was the real deal, not some bozo running around in an inflatable Sumo suit allegedly having fun pretending to be fat.
2. Diet and Exercise Work, But Where’s the Profit in That? Patented phama solutions on the other hand…
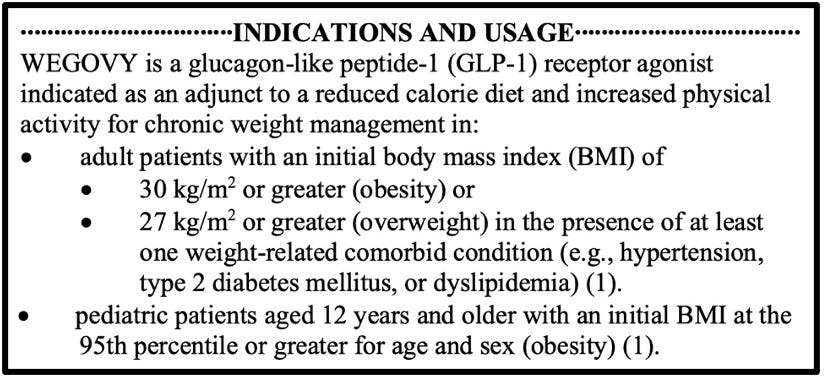
The age-old solution—eating better and moving more—works. It always has. But there’s no billion-dollar ad campaign for broccoli and brisk walks, so instead, lets pump the sexy narrative that obesity is an untreatable disease requiring expensive injections. The irony? These drugs work only if you also change your diet and lifestyle, (see Wegovy’s FDA-Approved product indications, in the box). No one really talks about the fine print, old-fashioned discipline which is always a barrier to the gut-busting weight-loss drug market.
The brief history of weight loss drugs, by the way, is a tragicomedy of human vanity, corporate greed, and the FDA’s uncanny ability to approve weight loss disasters every time corporations ask. With zero exceptions.
A quick whirlwind tour of weight loss drugs demonstrates how ungodly stupid humans are in failing to learn from recent medical history. Fen-phen, a combo of fenfluramine and phentermine, hit the U.S. market as a weight-loss drug in the early 1990s. American Home Products (later Wyeth) pushed fenfluramine hard, and by 1996, millions were popping it.
But reports later linked fen-phen to heart valve damage and pulmonary hypertension, and in September, 1997, the FDA yanked fenfluramine and its cousin dexfenfluramine (Redux) off the market. Phentermine stayed legal, but the fen-phen craze was toast.
Meridia (sibutramine) came on the U.S. market in November 1997, approved by the FDA as a prescription weight-loss drug. It promised modest results—about 5-10% body weight loss—and was aimed at obese patients with BMI over 30, or those at 27 with risks like diabetes. By 2010, research showed a 16% increased risk of heart attacks and strokes in patients with pre-existing heart issues. Meridia got the axe in October 2010 when Abbott voluntarily pulled it under FDA pressure.
Then came a really shitty situation brought to us in 1999 by Roche—a drug for those who like their weight-loss horror with a side of public humiliation. Xenical was a wonder pill that was great at blocking fat absorption but had an inconvenient side effect of making you accidentally shit your pants. Roche’s drug gifted the world with a brand new medical term “anal leakage,” putting into public parlance the thought that perfectly healthy adults wearing diapers was natural. The FDA added a liver warning in 2010 but didn’t pull it. Now, it’s sold as Xenical (prescription) and Alli (over-the-counter since 2007, lower dose).
Lastly, let’s not forget the loveable gastric banding, launched as a weight-loss strategy in the late 1970s. Adjustable versions emerged in the 80’s, but the real game-changer came in 1993 with laparoscopic adjustable gastric banding (LAGB). The FDA greenlit it in the U.S. in 2001, and it peaked around 2008. Then the problems came: It appeared that poorly fitted or slipping bands caused mayhem—stomach necrosis (tissue death) and sepsis from blood poisoning. Studies found reoperation rates at 15-60%, with patients needing fixes for slippage, erosion, or plain failure to lose weight. Fast forward to now, the Lap-Band, once a star, became a cautionary tale; removal surgeries now outpace installations. A 2020 article in Temple Health tracks the declining popularity and the long-term complication rates, including the 35-40% removal rate after 10 years.
3. GLP1 Adverse Effects Are Likely Underestimated. Aren’t they always?
GLP-1 drugs are the golden goose of weight loss, but they come with a price. And I don’t just mean financial—though at over $1,000 a month, that’s no joke. We’re talking nausea, diarrhea, gastroparesis (that’s when your stomach stops working), and muscle loss so extreme that some people look like they’ve aged 20 years in six months. Rats tested on GLP-1 were found to have thyroid tumors, but we’re different than rats aren’t we?
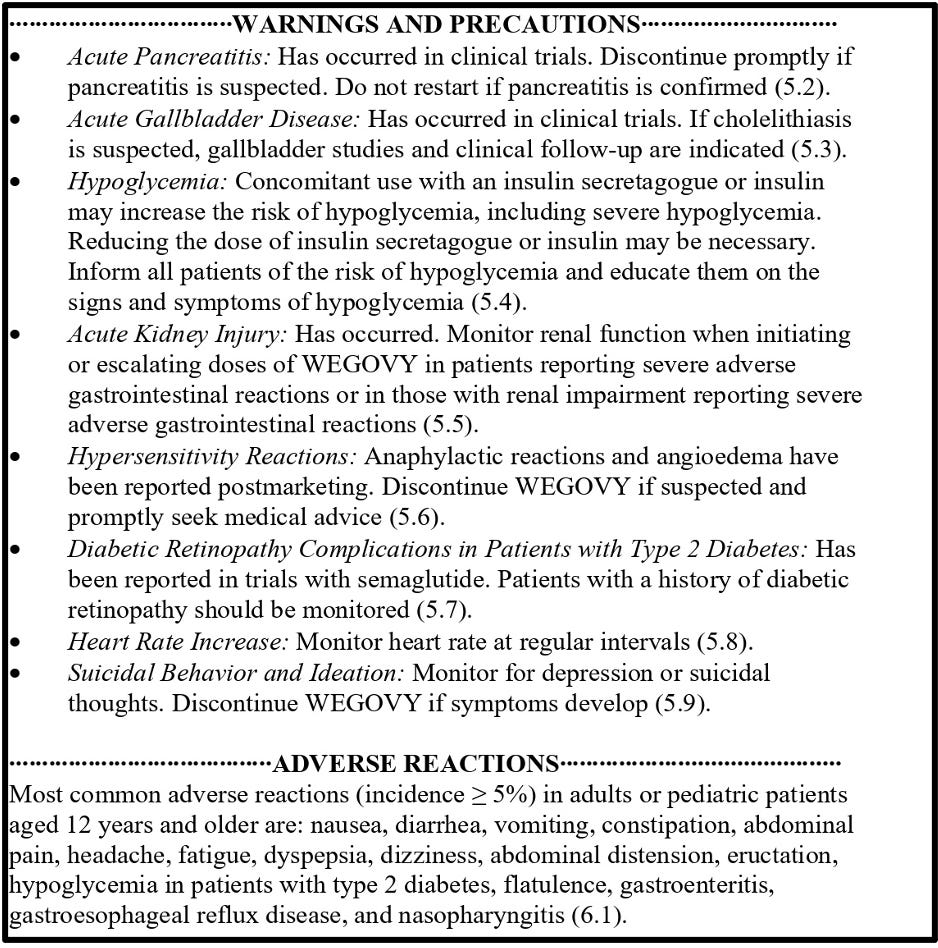
(see Below: from FDA-Approved label for Novo’s Wegovy)
Oh, and when you stop taking them? The weight comes back, often with added pounds. Sounds like a great plan for lifelong dependence, doesn’t it?
These drugs “work” because they can help you lose weight if you never stop taking the drug and don’t die from side effects. Reading from the label, you’ll find those the side effects include pancreatitis, muscle loss, paralytic gut issues and nausea so severe it makes food repulsive. Nothing screams health like vomiting up your dinner.
Remember the last big drug scandal we’re still living through? Big Pharma reconfigured good old “pain” and turned pain patients into lifelong opioid customers to make billions until the lawsuits caught up with them. Now, we’re seeing a similar kind of thing developing.
According to the news site Law360, “The number of lawsuits against GLP-1 manufacturers is growing, with over fifty stomach paralysis lawsuits filed in federal court by early 2024 with many more expected.” What’s coming down the road? Mass tort litigation, and it’s going to be BIG given the millions of people taking these drugs and some percentage of whom are being injured. My insiders in the legal world tell me the GLP-1 makers are secretly setting aside mountains of cash to cover future legal bills when they start getting sued for all the usual stuff criminal drug companies do: bribing doctors, lying to regulators, and planting propaganda with reporters like the Globe and Mail’s Andre Picard.
And the lobbying to make these drugs available for teens and even children is in full sway. The key point is that they’re aiming to hook people young, keep them on the drugs forever, and rake in the profits. Because nothing shouts ethical medicine like getting a 14-year-old hooked on an injectable weight-loss drug they’ll need for the rest of their lives.
4. Health Is More Than One Number
Corporate health has forced numbers on generations of people, figures which do nothing but play sheer havoc, leaving people obsessed about their cholesterol, blood pressure or blood sugar numbers. Of these, the BMI is one number that doctors use as a lazy shorthand for health.
Actual health is about so much more: nutrition, strength, endurance, mental well-being. But why encourage people to improve their eating and metabolic fitness when a magic shot can bring down BMI? It’s the same playbook as cholesterol drugs, anti-diabetes meds, and blood pressure pills: redefine health’s numbers in a way that guarantees more prescriptions.
The Bottom Line
Corporate health such as this Globe/Novo obesity event deserves even more mocking than I can muster. Clearly it isn’t about health—it’s about profit for The Globe and Novo Nordisk.
It’s also about convincing the public that normal human variation is a medical problem requiring pharmaceutical intervention, replacing personal agency with a monthly prescription. This is a story you’ll never find written by Andre Picard in the Globe and Mail.
The next time you hear someone say, “You should take Wegovy for your health,” ask them this: Since when did Big Pharma become the guardian of our well-being? For good measure, then remind them that the best prescription for lifelong health still comes down to common sense—which these days seems pretty uncommon.
https://disinformationchronicle.substack.com/p/corporate-health-wears-an-inflatable



