Upgrades to Overweight
Saturday, September 29, 2018
Cantor Fitzgerald Starts Vertex (VRTX) at Overweight
Cantor Fitzgerald analyst Alethia Young initiates coverage on Vertex (NASDAQ: VRTX) with a Overweight rating and a price target of $217.00.
New Apple Watch: The Worst Heart Device Ever?
If a company develops a new drug and proves its worth in large-scale clinical trials, physicians typically want to examine the evidence for themselves. If the sponsor claims that a new product saves lives, prescribers and patients need to feel comfortable that the claims are valid. Understandably, organizations that are interested in public health are reluctant to endorse most new drugs, partially because of fears that they will be accused of being influenced by industry money. As a result, it generally takes years for a truly life-saving drug to be supported and adopted by the clinical community.
Given this history of caution, the launch of the new Apple Watch Series 4 a week ago raised many an eyebrow.
In case you did not know, the Apple Watch Series 4 includes an FDA-approved heart monitor functionthat is capable of monitoring the electrocardiogram of the person who wears it.
Everyone expected that Apple would make every effort to tout the merits of this new device. Unsurprisingly, news outlets promulgated the Apple announcement with great excitement.
And Dr. Ivor Benjamin, the president of the American Heart Association, spoke favorably about its impact in person at a heavily promoted media event. He referred to the heart app as “game-changing.” Wow!
The American Heart Association never does this. Typically, even when the evidence supporting a new drug or device is overwhelming, the AHA remains silent. The AHA receives considerable funds from the pharmaceutical and device industry, and naturally, it does not want the public to think that its statements are influenced by these financial involvements.
So what was different this time?
Perhaps, the Apple Watch Series 4 actually does save lives. That would justify all of the hype.
However, according to Health News Review, the data supporting the use of the device was based on only 588 people, about half of whom had permanent or persistent atrial fibrillation. Reportedly, the device accurately identified the patient’s underlying rhythm more than 98% of the time. However, the performance of the notification function of the app (which sends an alert to the wearer) was not so stellar.
Is this data summary accurate? I do not know. Typically, the evidence that supports a new drug or device is published in the peer-reviewed medical literature. But as far as I know, the evidence supporting the device has not been subject to peer-review by any journal.
However, even if the data are accurate, it is important to understand that the device has not been approved by the FDA for any defined use. Typically, the FDA approves drugs and devices based on data from studies performed in populations who will use them. The people who will use the Apple Watch represent the general population. But the utility of the Apple Watch has not been evaluated in the general population.
In people who are likely to use the heart monitor function, the prevalence of atrial fibrillation is very low and the rhythm is likely to present as brief and highly infrequent bursts rather than a chronic arrhythmia. The rate of false positives and false negatives is highly dependent on the prevalence of the disorder in the population being evaluated. And accurately detecting a long-standing arrhythmia is not the same as accurately detecting “bursts.”
If the prevalence of atrial fibrillation in those wearing the Watch is less than 1% and if the accuracy of the device varies with the duration of the arrhythmia bursts, the number of false positive alerts is likely to be very high compared with the number of true positive alerts. Dr. Venk Murthy of the University of Michigan has made this very important point very eloquently in the Health News Review article.
So how accurate or useful is the Apple Watch in detecting short infrequent bursts of asymptomatic atrial fibrillation in patients with no known heart disease in whom the prevalence of the arrhythmia is extremely low? We simply do not know.
What does this mean? Two things.
First, the device is likely to alert many truly healthy people, causing enormous and unnecessary anxiety. Most will be motivated to see medical attention, potentially putting horrific pressures on our healthcare system. Even a low false positive error rate is problematic in a low-prevalence population, leading to meaningful squandering of healthcare resources.
Second, the device might detect atrial fibrillation in a few people who did not previously know that they had the arrhythmia. But what benefits does this knowledge provide? What does the presence of these asymptomatic bursts mean? Do they have clinical importance? Should they be treated? No one knows.
Even if the Apple Watch were perfect in its detection of atrial fibrillation in the general population, it is not clear how this information might be helpful. As Health News Review reported, screening of the general population for atrial fibrillation is not recommended. And anticoagulation (or interventions to treat the rhythm disturbance) in the very few patients with newly detected bursts of atrial fibrillation carries risks without known benefits.
As expected, there have been anecdotal reports of a handful of people who became aware of a cardiac diagnosis because they used the Apple Watch. But these stories do not describe “life-saving” events. And they are certainly not being balanced by untold reports of false alarms and unnecessary physician visits and treatments.
Dr. Benjamin may be right. The Apple Watch may be a game-changer — but not in a good way. If the device causes anxiety, yields minimal benefits, and subjects people to unnecessary risks, its utilization will place unwelcome burden on our healthcare system and cause harm to our patients.
Yet, apparently, Apple COO Jeff Williams has dubbed the Watch the “ultimate guardian for your health.” Really?
I do not know if Apple was quoted correctly or in the appropriate context. But Dr. Venk Murthy has responded very admirably: “We’d never accept such broad statements from a pharmaceutical ad, and we shouldn’t accept it from marketing for a device.”
Dr. Murthy is absolutely right. I strongly disagree with the statement attributed to Mr. Williams, and I am really uncomfortable with the public position taken by Dr. Benjamin.
In the current political climate, we relish the opportunity of being skeptical of drugs. It is acceptable (and quite fashionable) to launch missiles at drug manufacturers. All too often, we are right to do so.
Isn’t it time that we held devices to the same standards of truth and evidence?
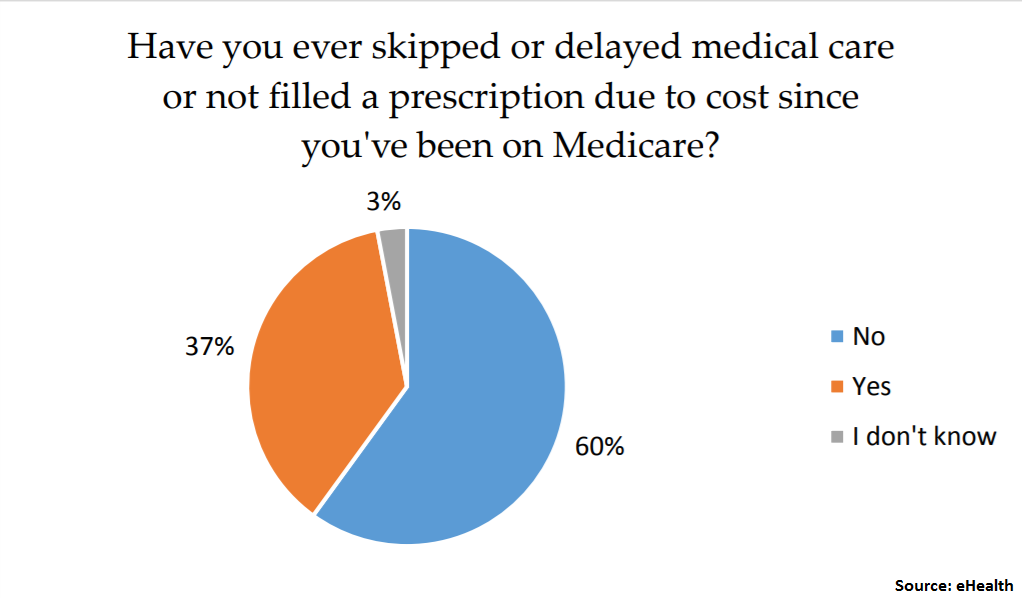
Nearly 4 in 10 people on Medicare skip their doctor’s visits
Medicare can help defray retirees’ health-care costs, but it’s no panacea. Some beneficiaries in the program are delaying medical attention due to the expense.
Nearly 4 out of 10 Medicare enrollees have admitted to skipping or delaying medical care, or failing to fill a prescription, in order to save money, according to a recent survey from eHealth.com.
In August, the private online health insurance exchange did an email poll of 1,020 individuals who were 65 and over, and had purchased a Medicare insurance product through the company.
“When it comes to understanding Medicare plan options and choosing one, it’s pretty complex and overwhelming,” said Andrew Shea, vice president of Medicare products at eHealth.com.
“Deductibles can sometimes be surprising to people with Medicare plans, and they don’t fully understand how the deductible works and the concept of having to float a decent amount of money before the coverage really kicks in,” he said.
Here are some of the expenses that are driving beneficiaries’ decision to avoid the doctor.
Paying for prescriptions
Of the participants who said they skipped the pharmacy due to the cost of drugs, 45 percent said that both the brand name and the generic medication were too costly.
Indeed, one of the costliest generics is atorvastatin — a widely used drug that treats high cholesterol, according to GoodRx.com, a site that provides discounts on prescription drugs.
The cash price for a monthly supply of the medication costs around $121, GoodRx.com found. Medicare Part D, which covers prescription drugs, can help lower this cost significantly.
Deductibles and more
Costs related to Medicare premiums only tell part of the story.
You probably know that, this year, individual filers with up to $85,000 ($170,000 for married and filing jointly) in modified adjusted gross income in 2016 can expect to pay $134 per month for Medicare Part B.
Those with higher incomes will pay more. See below.
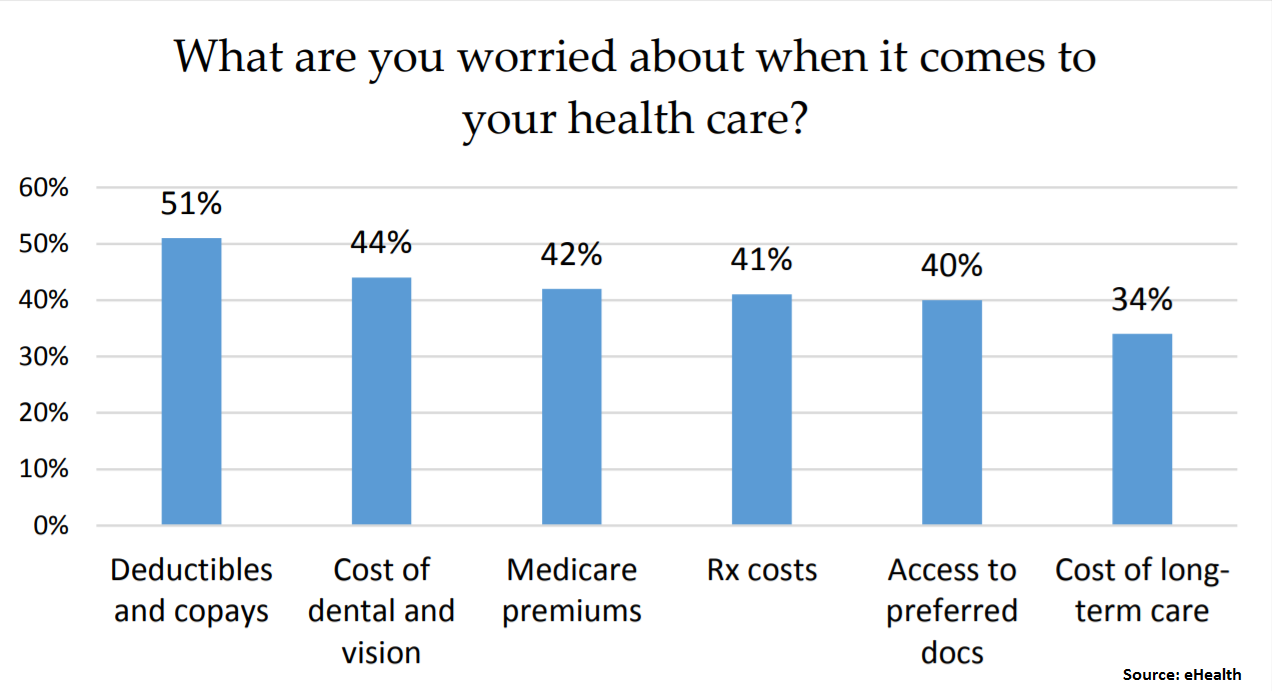
Deductibles and copays are keeping beneficiaries up at night. About half of the participants in eHealth.com’s study said they were worried about these costs.
Individuals enrolled in Medicare Part A, which covers hospital stays and skilled nursing, face a deductible of $1,340 per benefit period when they’re admitted to the hospital.
Beneficiaries of Medicare Part B, which covers doctor’s visits and other outpatient services, are subject to an $183 annual deductible in 2018. Once you’ve paid that amount, you’re responsible for 20 percent of the Medicare-approved amount for services.
Eyes and ears
One popular misconception among Medicare beneficiaries is that they’ll be covered for everything once they’ve enrolled in the health-care program.
That’s not so. Your dentures, routine vision exams and eyeglasses, as well as hearing aids, generally aren’t covered under original Medicare.
In all, 44 percent of the participants in eHealth’s study said that they were worried about the cost of dental and vision services.
Some Medicare Advantage plans may offer hearing and eye benefits. Beneficiaries should examine the depth of that coverage if they get it, said Shea.
Enrollees can also purchase standalone dental, vision and hearing insurance coverage, which averages between $35 and $45 a month at eHealth, he said.
What you should know
Don’t phone in your Medicare enrollment this fall. Here are a few recommendations to follow, according to Shea.
• Don’t assume last year’s plan is still right for you. Premiums go up, and the terms of your coverage can change. Review your plan during open enrollment.
• Check your mail. Around September, enrollees in Medicare Advantage plans receive an annual notice of change document that will provide a walkthrough of coverage updates. Take the time to read it, and call your insurer to clarify anything hard to understand.
• Talk to your doctor. If you’re skipping medical treatment due to cost, explain your situation to your physician. He or she may be able to point you toward less expensive treatment options, as well as community resources to help you deal with the expense.
Avoiding medical attention now can lead to mounting problems — and bills — down the road.
“One of the worst things is to be penny-wise and pound-foolish, ending up in the hospital with a $5,000 out-of-pocket bill,” said Shea.
Tim Berners-Lee’s new plan to upend the World Wide Web
Last week, Tim Berners-Lee, inventor of the World Wide Web, asked me to come and see a project he has been working on almost as long as the web itself. It’s a crisp autumn day in Boston, where Berners-Lee works out of an office above a boxing gym. After politely offering me a cup of coffee, he leads us into a sparse conference room. At one end of a long table is a battered laptop covered with stickers. Here, on this computer, he is working on a plan to radically alter how all of us live and work on the web.
“The intent is world domination,” Berners-Lee says with a wry smile. The British-born scientist is known for his dry sense of humor. But in this case, he is not joking.
This week, Berners-Lee will launch Inrupt, a startup that he has been building, in stealth mode, for the past nine months. Backed by Glasswing Ventures, its mission is to turbocharge a broader movement afoot, among developers around the world, to decentralize the web and take back power from the forces that have profited from centralizing it. In other words, it’s game on for Facebook, Google, Amazon. For years now, Berners-Lee and other internet activists have been dreaming of a digital utopia where individuals control their own data and the internet remains free and open. But for Berners-Lee, the time for dreaming is over.
“We have to do it now,” he says, displaying an intensity and urgency that is uncharacteristic for this soft-spoken academic. “It’s a historical moment.” Ever since revelations emerged that Facebook had allowed people’s data to be misused by political operatives, Berners-Lee has felt an imperative to get this digital idyll into the real world. In a post published this weekend, Berners-Lee explains that he is taking a sabbatical from MIT to work full time on Inrupt. The company will be the first major commercial venture built off of Solid, a decentralized web platform he and others at MIT have spent years building.
A NETSCAPE FOR TODAY’S INTERNET
If all goes as planned, Inrupt will be to Solid what Netscape once was for many first-time users of the web: an easy way in. And like with Netscape, Berners-Lee hopes Inrupt will be just the first of many companies to emerge from Solid.
“I have been imagining this for a very long time,” says Berners-Lee. He opens up his laptop and starts tapping at his keyboard. Watching the inventor of the web work at his computer feels like what it might have been like to watch Beethoven compose a symphony: It’s riveting but hard to fully grasp. “We are in the Solid world now,” he says, his eyes lit up with excitement. He pushes the laptop toward me so I too can see.
On his screen, there is a simple-looking web page with tabs across the top: Tim’s to-do list, his calendar, chats, address book. He built this app–one of the first on Solid–for his personal use. It is simple, spare. In fact, it’s so plain that, at first glance, it’s hard to see its significance. But to Berners-Lee, this is where the revolution begins. The app, using Solid’s decentralized technology, allows Berners-Lee to access all of his data seamlessly–his calendar, his music library, videos, chat, research. It’s like a mashup of Google Drive, Microsoft Outlook, Slack, Spotify, and WhatsApp.
The difference here is that, on Solid, all the information is under his control. Every bit of data he creates or adds on Solid exists within a Solid pod–which is an acronym for personal online data store. These pods are what give Solid users control over their applications and information on the web. Anyone using the platform will get a Solid identity and Solid pod. This is how people, Berners-Lee says, will take back the power of the web from corporations.
For example, one idea Berners-Lee is currently working on is a way to create a decentralized version of Alexa, Amazon’s increasingly ubiquitous digital assistant. He calls it Charlie. Unlike with Alexa, on Charlie people would own all their data. That means they could trust Charlie with, for example, health records, children’s school events, or financial records. That is the kind of machine Berners-Lee hopes will spring up all over Solid to flip the power dynamics of the web from corporation to individuals.
A NEW REVOLUTION FOR DEVELOPERS?
Berners-Lee believes Solid will resonate with the global community of developers, hackers, and internet activists who bristle over corporate and government control of the web. “Developers have always had a certain amount of revolutionary spirit,” he observes. Circumventing government spies or corporate overlords may be the initial lure of Solid, but the bigger draw will be something even more appealing to hackers: freedom. In the centralized web, data is kept in silos–controlled by the companies that build them, like Facebook and Google. In the decentralized web, there are no silos.
Starting this week, developers around the world will be able to start building their own decentralized apps with tools through the Inrupt site. Berners-Lee will spend this fall crisscrossing the globe, giving tutorials and presentations to developers about Solid and Inrupt. (There will be a Solid tutorial at our Fast Company Innovation Festival on October 23.)
“What’s great about having a startup versus a research group is things get done,” he says. These days, instead of heading into his lab at MIT, Berners-Lee comes to the Inrupt offices, which are currently based out of Janeiro Digital, a company he has contracted to help work on Inrupt. For now, the company consists of Berners-Lee; his partner John Bruce, who built Resilient, a security platform bought by IBM; a handful of on-staff developers contracted to work on the project; and a community of volunteer coders.
Later this fall, Berners-Lee plans to start looking for more venture funding and grow his team. The aim, for now, is not to make billions of dollars. The man who gave the web away for free has never been motivated by money. Still, his plans could impact billion-dollar business models that profit off of control over data. It’s not likely that the big powers of the web will give up control without a fight.
When asked about this, Berners-Lee says flatly: “We are not talking to Facebook and Google about whether or not to introduce a complete change where all their business models are completely upended overnight. We are not asking their permission.”
Top Five Trending Kidney Care Topics from DaVita Medical Insights
DaVita Kidney Care, a division of DaVita Inc. (NYSE: DVA), a leading provider in kidney care services, today shared its “top five” list from the DaVita Medical Insights podcast and blog. Both are forums to discuss trending news and issues in kidney care and were created by physicians, for physicians.
The top five stories include:
- The Self-Regulating Bioartificial Kidney – Bryan Becker, M.D., discusses The Kidney Project, an initiative officially launched in 2015 by nephrologists William Fissell, M.D. and David Humes, M.D. “to create a small, surgically-implanted and free-standing bioartificial kidney,” which would help settle organ supply barriers.
- Effectively Managing Kidney Patients’ Transitions of Care – Ananda Harrison interviews Dr. Becker on the importance of managing care when a patient moves within or between health care settings, across states of health and between clinicians, and the physician’s role in this process.
- Why Physicians Choose Nephrology – Physician leaders for DaVita recount why they chose to become nephrologists in honor of National Doctors Day.
- Electronic Health Records: Past, Current and Future Landscape – Electronic health records (EHRs) first started to appear in the 1970s, yet physicians have been slow to adopt the technology because of cost and workflow disruption. Listen to Adam Weinstein, M.D., cover the evolution of EHRs, what the future potentially holds for this technology and where its full functionality may ultimately settle.
- Study: The Impact of Missed Dialysis Treatments on Clinical Outcomes – A study conducted by DaVita Clinical Research aimed to identify the prevalence of in-center hemodialysis absenteeism and its effects on clinical outcomes. Steve M. Brunelli, M.D., MSCE reviews the key takeaways, including how missed treatments impact hospitalization and mortality among dialysis patients.
Cidara initiates Phase 3 trial to evaluate efficacy, safety of antifungal
Cidara Therapeutics, Inc., a biotechnology company developing novel anti-infectives including immunotherapies, today announced that the first trial site has been activated for ReSTORE, a Phase 3 clinical trial evaluating the efficacy and safety of the company`s lead antifungal, rezafungin, to treat candidemia and invasive candidiasis. Rezafungin is a novel echinocandin antifungal being developed as a once-weekly, high-exposure therapy for the treatment and prevention of serious invasive fungal infections.
“Given the compelling data from our Phase 2 program, we are very pleased to initiate our global Phase 3 program of rezafungin,” said Jeffrey Stein, Ph.D., president and chief executive officer of Cidara. “Difficult-to-treat, invasive Candida infections are associated with a high mortality and affect the most vulnerable patients. Rezafungin has the potential to be the first new antifungal approved for this indication in over a decade and, given how the drug works, it has the potential to improve outcomes for patients and allow them to leave the hospital earlier, resulting in reduced healthcare costs.”
ReSTORE is a global, randomized, double-blind, controlled Phase 3 pivotal clinical trial evaluating the efficacy and safety of once-weekly intravenous dosing of rezafungin compared to once-daily dosing of caspofungin in patients with candidemia and/or invasive candidiasis. The trial design will be similar to the company`s Phase 2 STRIVE study, which met its primary safety and efficacy objectives. The ReSTORE trial is designed to evaluate one rezafungin dosing regimen of 400 milligrams (mg) for the first week followed by 200 mg of rezafungin once weekly for up to four weeks in total. This treatment arm will be compared to caspofungin in a 1:1 randomization.
The primary efficacy endpoint of ReSTORE, which will be used for a U.S. Food and Drug Administration (FDA) New Drug Application submission, is all-cause mortality at day 30. The primary efficacy endpoint for the European Medicines Agency (EMA) is expected to be global response at day 14.
“I am very enthusiastic about the initiation of this important trial of rezafungin as a once-weekly echinocandin which may offer a new solution for patients and physicians to treat serious invasive Candida infections,” said Cornelius J. Clancy, M.D., Associate Professor of Medicine and Director of the Mycology Research Unit and XDR Pathogen Lab at the University of Pittsburgh. “There is an urgent and growing need for new therapeutic approaches for these infections, which typically afflict highly vulnerable patients, including those who are critically ill and have compromised immune systems. Rezafungin has the potential to overcome the significant limitations associated with current standards of care such as sub-optimal dosing, increasing resistance, drug-drug interactions and toxicities, all of which complicate therapy in patients who are already ill.”
The ReSTORE trial will enroll approximately 184 modified intent-to-treat, or mITT, patients and is expected to generate topline data in 2020. This global trial is anticipated to be conducted at approximately 100 clinical trial centers across the United States, Europe, Asia and Australia.
Subscribe to:
Posts (Atom)