Staff members at the Canterbury Rehabilitation and Healthcare Center
in Richmond, Virginia, did everything they could to prevent the spread
of COVID-19. Even before the first case arrived at Canterbury — a
190-bed facility that includes units for long-term care, memory care,
and rehabilitation — visitors were banned and group dining was shut
down.
After the first case of COVID-19 was identified on March 13,
Canterbury’s owner, Marquis Health Services, “brought in a lot of
resources and spent a lot of money,” said Jim Wright, MD, the facility’s
medical director, in a phone interview. Because the company owned
several long-term care facilities, Marquis “also had the advantage of
having PPE [personal protective equipment] at multiple facilities, and
they were able to divert PPE to us.” Marquis also paid staff members at
double the usual rate to boost retention.
As more COVID-19 cases appeared, “we immediately set up part of our
nursing home just for people with COVID-19,” he continued. “We moved
them into isolation rooms and followed CDC guidelines; we closed the
door and had an isolation cart outside that everyone used to change into
gowns and gloves” when they went into a COVID patient’s room. Moving
patients to the ward was difficult because “we had to take residents and
their belongings out of rooms they had lived in for years and move them
down the hallway to a different unit, which was most strenuous in
people power and time.”
In addition, Canterbury assigned specific nurses to work only on the
COVID ward “so they wouldn’t be going from a COVID ward to a COVID-free
ward,” Wright said. “We developed ingress and egress from those wards so
they wouldn’t be in another part of the facility any time during the
day.” The nurses even parked in a separate parking lot, and had separate
showers they could use before they went home. The facility also tried
to test patients and workers, but it had limited access to testing, and
the tests that were available took 11 days to be returned, he said. Cases, Deaths Still Rampant
Even with all of that, with a census of 165 residents, Canterbury had
130 infections and 49 deaths, said Wright. “When we were finally able
to test our entire population, we found that almost half of those tested
were asymptomatic carriers. So we had residents with no symptoms still
shedding the virus, transmitting it, and infecting others.”
COVID-19 has been especially devastating for the dementia patients,
he added, “especially if they’re isolated in their room and they used to
have a common area to visit and see family members. When they can do
that, they’re reminded what time of day it is, and if they see someone
next to them eating, they’re going to eat, so we’ve had quite a bit of
trouble in those people living with dementia” and the facility is
working hard to reestablish eating and hydration patterns. As a result,
reintroducing group dining to dementia patients “is a number one
priority right now,” he said.
Unfortunately, Canterbury’s story has become all too common, said
David Grabowski, PhD, professor of healthcare policy at Harvard Medical
School in Boston. “It’s a similar story in Massachusetts,” he said in a
phone interview, noting that at one nursing home there, “they closed the
facility to visitors, they had no communal dining, they were taking the
temperature of the staff as they came into the building, and yet it
still spread.”
These facilities account for a disproportionate number of COVID-19
deaths, Grabowski noted. “Nursing homes account for about 0.5% of
individuals nationwide … and yet the flawed data we have is that 25% of
the deaths are in nursing homes,” he said. Data from The New York Timessupport
that conclusion, with the paper reporting that “more than 63,000
residents and staff members at those facilities have contracted the
virus, and more than 10,500 have died. That means that nearly a quarter
of the deaths in the pandemic have been linked to long-term care
facilities.”
Grabowski said that percentage is probably an undercount: “I think the true number is closer to 50%,” he noted. Ready-Made Vectors
Nursing homes are ready-made vectors for coronavirus, Wright
explained. “Nursing homes, especially state-supported nursing homes, are
the home for people who generally have had little access to healthcare
because of poverty through their entire lives, and they have reached the
point where they can no longer live in the community because of illness
and disability,” he said.
“So it’s the home for the most frail, the most ill, the most
impoverished members of the community. Add to that the shared quarters
that most publicly funded nursing homes have, and you have the perfect
storm for infectious disease to spread from one person to the next.”
Nursing homes’ high COVID-19 prevalence and mortality rates have
gained the attention of the Trump administration. On March 23, following
a COVID-19 outbreak at a nursing home in Seattle, the Centers for
Medicare & Medicaid Services (CMS) announced it would be having more targeted infection-control inspections of nursing homes.
CMS also took other steps related to nursing homes, including announcing forthcoming transparency rules requiring homes to report COVID-19 cases to patients, families, and the CDC, and doubling Medicare payments for certain COVID-19 tests run on high-throughput equipment.
But CMS’s efforts can only go so far, said Christopher Laxton,
executive director of AMDA, the trade group for nursing home medical
directors. “CMS, I think, has really tried to be helpful by waiving
certain restrictions and allowing telemedicine to come in with greater
frequency and intensity,” Laxton said in a phone interview. However,
“CMS is a regulator and what regulators do is punish entities when
conditions aren’t met.”
Tricia Neuman, executive director of the Program on Medicare Policy
at the Kaiser Family Foundation (KFF), noted that she spoke with one
nursing home medical director “who had been in touch with other nursing
homes who were concerned about coming forward with the problems they’re
facing because they’re worried about being slapped with fines. In the
midst of this crisis, when they’re needing urgent help, they’re
reluctant to put their cards on the table,” she said.
Keeping adequate staffing is a particularly difficult problem for nursing homes, experts said. According to KFF,
38% of workers in long-term care facilities are age 50 or older, and
58% make $30,000 or less annually. “We’re talking about a workforce that
is 80% female, low-income, and disproportionately African American —
people who are working in long-term care facilities under an enormous
amount of stress,” said Neuman. “It’s not easy work, yet we as a nation
rely on these workers to care for our parents and grandparents, and now
in the COVID crisis, under the most strenuous circumstances.”
Treating these workers poorly seems to be part of the culture, said
Canterbury’s Wright. “If you had a living wage paid to staff so that
staffing levels would always be where we want them to be, then it would
have made a difference, but we would have had to have nursing homes in a
country that values elders more and contributes more resources to elder
care,” he said. “We are not in that country; we’re in a country that
devotes about a third of the average resources to its elders compared to
what other developed countries devote.” Reimbursement Issues
The reimbursement system for nursing homes also is a big issue. “The
larger picture is that we’ve always had under-investment in nursing
homes,” said Grabowski, who is a member of the Medicare Payment Advisory
Commission, but who emphasized he was speaking only for himself. “We
have a strange system where we overpay on the Medicare side of nursing
homes — for short-stay, post-hospital patients.”
“On the other side are long-stay residents who are going to be there
for the remainder of their life; their care is paid for by Medicaid,
which typically pays below cost,” he continued. Therefore, the whole
structure is built on “bringing in enough short-stay Medicare patients
to subsidize long-stay Medicaid residents.”
The COVID crisis “shows that that model is broken,” he said. “Right
now, elective surgeries have stopped, and the COVID patients — many
nursing homes are not able to admit them, or they shouldn’t. Put that
together with the idea that the cost structure has gone way up with
infection control and staffing issues, and it’s a really challenging
time. It has shown how fractured this financing model is … It begs
rethinking of how we pay for nursing homes in the U.S. We are so reliant
on Medicaid, and we’re going to need to rethink that going forward.”
In the meantime, what can nursing homes do to stop the spread of
COVID-19? “In the end, it’s shoe-leather epidemiology, with contact
tracing, isolation, and quarantine,” along with more testing, said
Laxton.
He also urged more cooperation between hospitals, nursing homes, and
state and local health officials. “We have seen orders coming from state
governments that say nursing homes have to take hospital discharges,
whether we’re able to care for them or not,” including in some cases
fines for nursing homes that refuse to do so, he said. “That
demonstrates the degree to which people don’t understand nursing homes …
We have to fight these battles on a daily basis.” https://www.medpagetoday.com/infectiousdisease/covid19/86157
The CDC currently recommends all Americans wear cloth masks in public
to curtail transmission of COVID-19 coronavirus, but another form of
personal protective equipment might be a better idea: plastic face
shields.
A JAMA Viewpoint recently published by Eli Perencevich, MD,
of the University of Iowa, and colleagues discussed how limitations to
the supply chain have made obtaining medical masks for the community
difficult, and face shields for the community may be a viable alternative.
“While medical masks have limited durability and little potential for
reprocessing, face shields can be reused indefinitely and are easily
cleaned with soap and water, or common household disinfectants,” they
wrote. “They are comfortable to wear, protect the portals of viral
entry, and reduce the potential for autoinoculation by preventing the
wearer from touching their face.”
And unlike medical masks, face shields do not have to be removed to communicate with others, they said.
Moreover, they noted a simulation study of influenza virus found face
shields reduced viral exposure by 96% when worn within 18 inches of a
cough, and when this study was repeated using the recommended distancing
protocol of 6 feet, inhaled virus was reduced by 92%.
No studies have examined the benefits of face shields on source
control, or their ability to contain a sneeze or cough, when worn by
those who are asymptomatic or symptomatic. But studies on this should be
completed quickly, Perencevich and colleagues suggested.
They added that guidelines from the Infectious Diseases Society of
America, along with the Society for Healthcare Epidemiology of America
(SHEA) and the Pediatric Infectious Diseases Society “included societal use” of personal protective equipment (PPE) such as face shields and masks when discussing how the U.S. can safely ease COVID-19 distancing restrictions.
Judy Guzman-Cottrill, DO, pediatric and infectious diseases liaison
to the SHEA Board of Trustees, who was not involved with the research,
told MedPage Today face shields are “definitely a potential alternative to ‘universal masking’ in the community.”
Face shields are also an important PPE component for healthcare
workers, as “manufacturing of face shields in the U.S. has ramped up
very quickly,” she noted.
“What we still need to clarify is if a face shield alone is adequate
protection for healthcare workers from respiratory viruses while caring
for symptomatic patients, or do healthcare workers need a face shield
plus surgical mask?” said Guzman-Cottrill, of Oregon Health &
Science University. “I don’t think we have enough evidence yet to answer
this question.”
Perencevich and colleagues said randomized trials would likely not be
completed in time to verify the efficacy of face shields, and advised,
“taken as a bundle, the effectiveness of adding face shields as a
community intervention to the currently proposed containment strategies
should be evaluated using existing mathematical models.”
The Capitol’s attending physician sent coronavirus recommendations to
senators and staffers on Friday outlining best practices as the Senate
prepares to return on Monday amid the pandemic.
The six-page list of guidelines from Brian Monahan, the attending
Capitol physician, recommends but does not require the use of face masks
within the Capitol complex. The Architect of the Capitol previously announced
that it was requiring its employees to wear face coverings, but that
did not apply to senators, their staff, Capitol police or reporters.
“Use of a face covering is voluntary unless required by specific
Agency policy, and should be promoted at all times. Use of a face
covering while in the office has the additional advantage of serving as a
source control to minimize virus in the workplace environment and
contributes to the cleaning process efficiency,” Monahan wrote in the
guidance, a copy of which was obtained by The Hill.
He added that “individuals retain the option of not using a face
cover if they can maintain the 6-foot separation guidelines.” But he
noted that the Capitol Police “will not take enforcement actions
regarding face coverings.”
Monahan is requiring all employees to check their temperatures at
home and complete an 11 question self-assessment each day before coming
to the Capitol complex. They will have to report their results to a
designated individual in the office.
“Participation in a health monitoring program is required for all
Congressional employees unless impacted by a collective bargaining
agreement or in those instances where employment is exclusively by
telework or at an isolated/solitary occupancy duty station,” he wrote.
Once in the Capitol complex, Monahan is recommending senators and
their staff minimize the number of individuals in their offices,
avoiding gatherings and modifying office layouts when possible to try to
allow for at least six feet of distance.
That includes allowing staff to telework, which many offices have been doing since late March.
“These guidelines are based on current Centers for Disease Control
and Prevention best practices to minimize risk of coronavirus
transmission in the workplace through use of social distancing measures
and daily screening of employee health prior to reporting for duty,”
Monahan wrote. https://thehill.com/homenews/senate/495738-capitol-physician-recommends-masks-temperature-checks-for-when-senate-returns
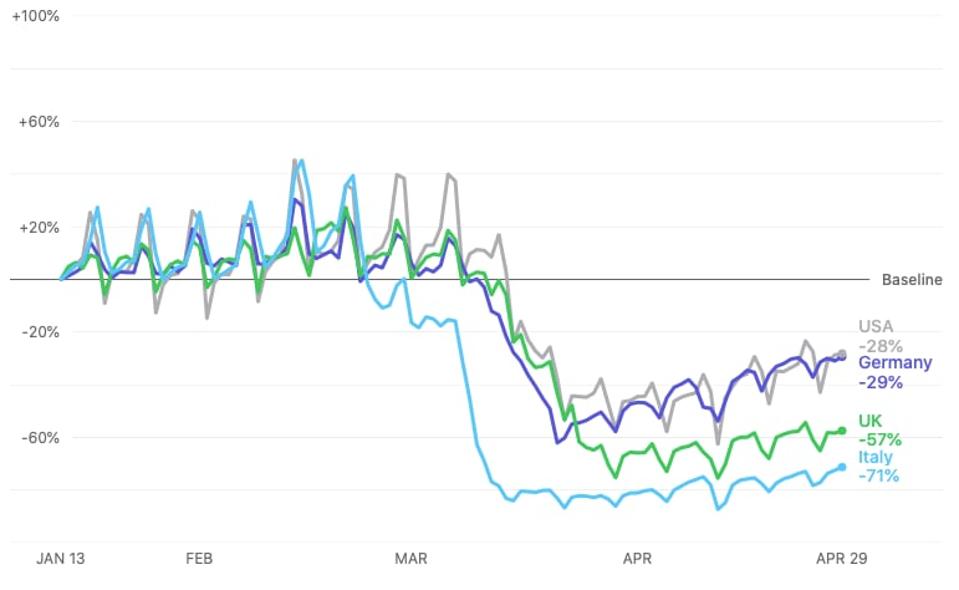
Bye-bye shelter-in-place. Hello re-opening.
Apple’s Mobility Trends report shows that traffic in the US and other countries like Germany has pretty much doubled in the past three weeks. It had been down up to 72%.
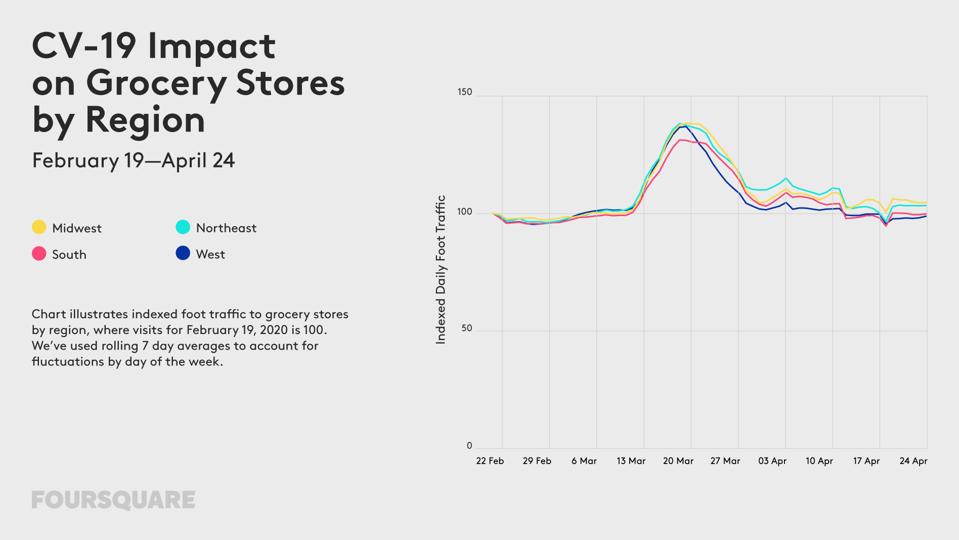
And location data provider Foursquare says that gas and fast food
visits are back to pre-COVID-19 levels in the American Midwest.
Screenshot of Apple’s mapping data showing a resurgence in traffic
John Koetsier
Rural areas are following the same pattern.
“Gas station traffic has returned to pre-COVID-19 levels in the
Midwest, and in rural areas throughout the country,” Foursquare said
yesterday in a blog post. “Foot traffic to quick service restaurants (QSRs) has risen over the past several weeks.”
Whether governments, medical professionals, and scientists want it to
or not, people seem tired of the shutdown and eager to get back to some
semblance of normal life.
Another sign of the impending return to normal?
Grocery store visits are down to normal levels, after being 30-40%
higher than normal in late March as people tried to stock up for a long
shutdown.
Grocery store visits are returning to normal
Foursquare
While the Apple data is measured by people searching Apple Maps for
directions, the Foursquare data is captured by people actually visiting
locations. 13 million Americans have granted the company permission to
capture their data and use it in privacy-safe ways.
While more people are going more places, it hasn’t impacted a number of hard-hit industries just yet.:
Gyms: still down 65-69%
Clothing stores: still down 72%
Furniture stores: still down 56-60%
Movie theaters: still down 75%
Nail salons, on the other hand, are “only” down 38-42%, and hotels in
the Midwest are down just 49%, compared to a 63-70% decline in other
regions.
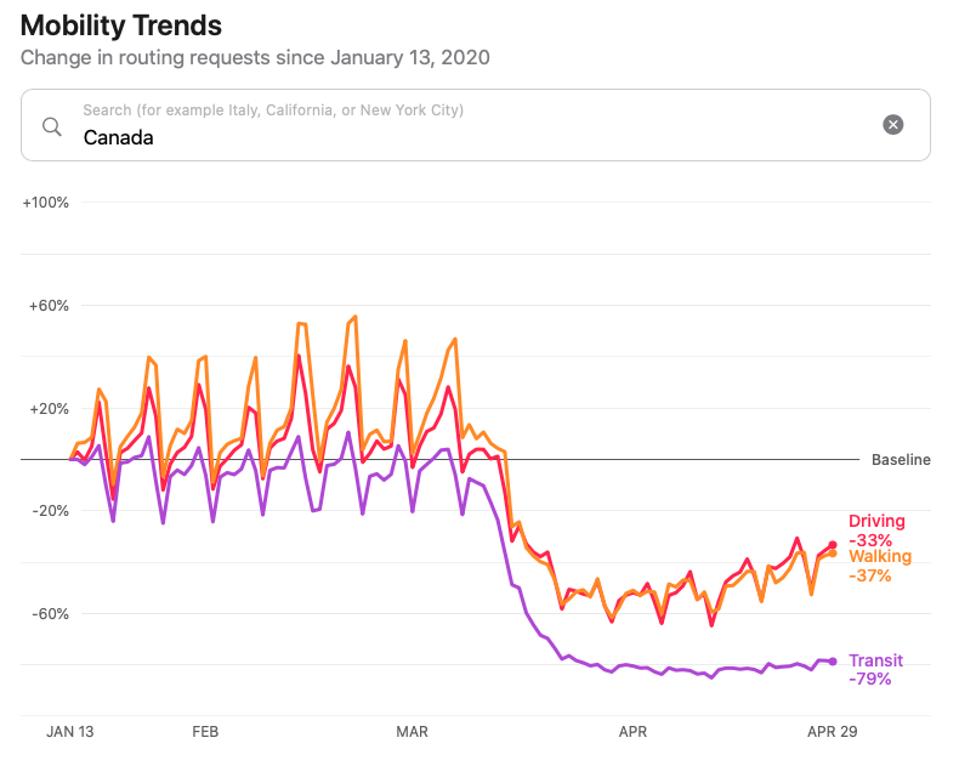
Interestingly, as Apple’s data from Canada shows, while driving and
walking are edging back up to normal levels, people are avoiding
transit, which is still down 79% from pre-Coronavirus levels. Driving by
yourself is safe, apparently, but sitting in a bus or on a train with
hundreds of others is not.
Apple Maps routing directions data for Canada
John Koetsier
“People are feeling the itch to get back to the real world,”
Foursquare says. “As officials begin the process of relaxing some
business restrictions, we’re starting to see upticks in foot traffic to
various places. This is true across regions, regardless of
state-specific policies.”
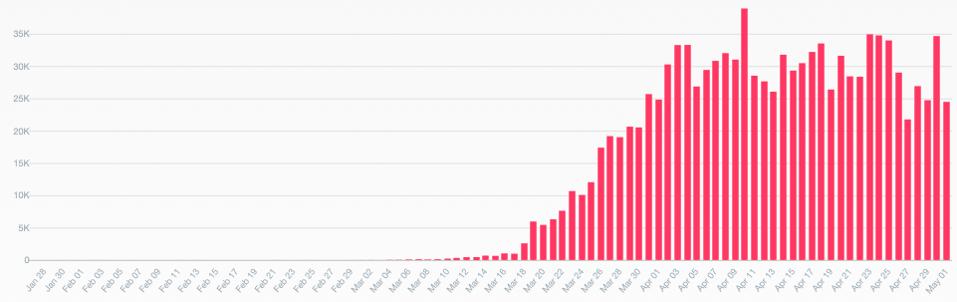
New cases of COVID-19 by day in the US, according to Coronavirus.app.
John Koetsier
COVID-19 cases seem to have started to level off in the US, but there are still 1.1 million total cases,
with 65,034 deaths. There are currently almost 900,000 active cases.
The question is: as states start to open up, and as people start to
decide they’re done with quarantine and shelter-in-place policies, will
that go up?
“It doesn’t look like an annual meeting and it
doesn’t feel like an annual meeting,” Warren Buffett starts
off Berkshire Hathaway (NYSE:BRK.B) (NYSE:BRK.A) annual meeting from an empty arena in Omaha.
As for the coronavirus’s effect on the economy,
the range of possibilities is still “extraordinarily wide,” Buffett
said, but he’s optimistic that the U.S. will overcome it.
“In 2008-2009, our economic train went off the
track due to weaknesses in the system, the banks… this time we have
pulled the train off the tracks and put it on the siding,” Buffett said.
“I remain convinced that nothing basically can
stop America. We have faced tough problems before — the American
miracle, the American magic has always prevailed and it will do so
again.”
He gives a history lesson on how the U.S. has managed to overcome such disruptions as the Civil War and the Depression.
Update at 5:40 PM ET: His conclusion — “Never bet against America. In my view that’s as true today as it was in 1789.”
Still, he said, “We still have a long way to go in creating an even wealthier and more equitable society.”
5:50 PM ET: He emphasizes that
nobody knows what’s going to happen in the markets tomorrow or next
year, so “you can bet on America, but you have to be careful on how you
bet.”
The meat of the annual meeting will likely come during the question session after the meeting’s formal business concludes.
The World Health Organization said Friday it hoped China would invite
it to take part in its investigations into the animal origins of the
novel coronavirus.
“WHO would be keen to work with international partners and at the
invitation of the Chinese government to participate in investigation
around the animal origins,” WHO spokesman Tarik Jasarevic told AFP in an
email.
He said the UN health agency understood there were a number of
investigations under way in China “to better understand the source of
the outbreak”, but added that “WHO is not currently involved in the
studies in China.”
Scientists believe the killer virus jumped from animals to humans, emerging in China late last year, possibly from a market in Wuhan selling exotic animals for meat.
But US President Donald Trump has fuelled speculation and
rumours—generally rejected by experts—that the virus may have emerged in
a top-secret Chinese lab.
WHO has also faced scathing criticism from Trump, who earlier this
month suspended Washington’s funding after accusing the WHO of
downplaying the seriousness of the outbreak and of kowtowing to China.
The UN health agency chief Tedros Adhanom Ghebreyesus did travel with
a team to China in late January, where he met with Chinese President Xi
Jinping to learn more about the response.
This paved the way, Tedros explained earlier this week, for an
international team of scientists to travel there in February to
investigate the situation, including experts from China, Germany, Japan,
the Republic of Korea, Nigeria, the Russian Federation, Singapore and
the United States of America.
But as investigations into the origins of the virus have picked up pace in China, the WHO has not been involved.
The ongoing investigations are believed to be looking at “human cases
with symptom onset in and around Wuhan in late 2019, environmental
sampling from markets and farms in areas where the first human cases
were identified, and detailed records on the source and type of wildlife
species and farmed animals sold in these markets,” Jasarevic said.
He stressed that the results from the virus origin studies were
“essential to preventing further zoonotic introductions of the virus
that causes COVID-19 into the human population.”
“WHO continues to collaborate with animal health and human health
experts, countries and other partners to identify gaps and research
priorities for the control of COVID-19, including the eventual
identification of the source of the virus in China,” he said. https://medicalxpress.com/news/2020-05-china-probe-virus.html
REDHILL BIOPHAR/S ADRRDHL 6.69%,
known primarily as a biopharmaceutical company focused on
gastrointestinal diseases, is joining the race to develop coronavirus
treatments with two pipeline drugs it believes can help treat the
disease that’s triggered a pandemic.
CEO Dror Ben-Asher spoke with Benzinga about opaganib, for which the
company filed an Investigational New Drug Application with the FDA in
April; and RHB-107, on which RedHill is partnering with the National Institute of Allergy and Infectious Diseases in an evaluation for COVID-19. Benzinga: What is current stage of opaganib and RHB-107? What type of results have they shown? Ben-Asher: RedHill has been developing opaganib
primarily for oncology for the past several years and we have tested it
in well over 100 patients. When coronavirus began to spread rapidly, we
decided that opaganib might apply to coronavirus. The drug is
anti-inflammatory, it has antiviral properties and it acts on the same
issues that moderate to severe patients of coronavirus are struggling
with.
Opaganib was first opened as a compassionate use program in Israel,
which means physicians can treat patients in designated hospitals using
opaganib outside clinical studies. Thus far, we have results from
five patients. They are doing very well in terms of overall improvement,
including reduction in inflammation and a decrease in oxygenation
requirement.
Some patients left the hospital while others left the ICU. It’s a small sample size, but we like what we are seeing.
We recently announced that RedHill signed an agreement with the
National Institute of Allergy and Infectious Diseases to
evaluate RHB-107 for coronavirus. It’s a priority project and thus
far RHB-107 has been tested in over 300 patients.
Both Opaganib and RHB-107 are novel molecules that have plenty of
data. We are pursuing both of them in the fight against coronavirus.
There are very few companies out there that have ‘two shots on goal’ for
a coronavirus drug.
Benzinga: Can you give a brief history of RedHill’s relationship with FDA? What other trials has RedHill been involved in? Ben-Asher: RedHill has been meeting with the FDA
numerous times over the last 10 years. We successfully developed and
brought to the market a drug Talicia with FDA approval. Talicia was
designed to treat an infection, Helicobacter pylori. Over 100 million
Americans are infected with Helibobacter pylori, with some parts of the
world population being over 50% infected.
In addition, we are already promoting three products commercially in
the USA with 100 sales representatives in North Carolina. The largest of
the three is Movantik, which we acquired in the beginning of April from
AstraZeneca plcAZN 0.75%.
We have also filed a new application to start a clinical study in the
U.S. for opaganib as a coronavirus drug, and we expect an FDA response
very soon. Benzinga: Can the data from Israel be used in seeking opaganib approval in the U.S.? Ben-Asher: The data in Israel is not considered
clinical study data because it’s compassionate use. Opaganib is used to
help patients in need based on the physician’s discretion. When a
physician has no better alternative, they can choose to treat a patient
with opaganib.
We are pursuing clinical studies in the U.S., and upon approval from
the FDA, we will move forward with a controlled study. If the data is
the same in the controlled study as it is in the compassionate use in
Israel, then we will have a discussion with the FDA for getting it
approved. Benzinga: What would be a timeline for the drug in the U.S.? Ben-Asher: It’s too early to tell, but the magnitude
and urgency of getting the first drug approved for coronavirus is very
significant. Although, the FDA is mandated to ensure that drugs are safe
and effective through the requires clinical studies in a controlled
setting.
The treatment for coronavirus is really short; it’s only a matter of
weeks. The coronavirus does not last long, [and] therefore the studies
are not expected to take long. It’s not expected to be difficult to
recruit patients either, because the need for a new treatment is really
significant. Benzinga: How prepared is the company to scale up production of opaganib if approved in the U.S.? Ben-Asher: RedHill has been working hard
toward boosting production to a large scale. We secured a manufacturer
and we can scale up manufacturing, including getting additional
manufacturers, as soon as the demand for opaganib is needed. https://www.benzinga.com/general/biotech/20/05/15874371/redhills-ceo-on-biopharmas-two-shots-on-goal-for-coronavirus-drug