Medtronic (NYSE:MDT) announces positive
results from a U.S. pivotal study evaluating its MiniMed 780G Advanced
Hybrid Closed Loop insulin pump in adolescent and adult diabetics. The
results were virtually presented at the Scientific Sessions of the ADA.
The device, CE Mark’d
this week, features a default target of 100 mg/dL (with an option of
120 mg/dL), programmable insulin action time from two to eight hours and
automatic corrections every five minutes.
Average A1C levels of 7.0% with overall time in
range (70-180 mg/dL) of 75% and overall time below range (less than 70
mg/dL) of 1.8%.
Autocorrection contributed 22% of all bolus insulin.
Participants in SmartGuard (closed loop) 95% of the time.
At the default setting, mean sensor glucose was 144 mg/dL overall and 148 mg/dL overall.
No severe hypoglycemia or diabetic ketoacidosis occurred.
Time in range at the default setting was 76% overall at the 2-3 hour active insulin time (AIT) and 79% at the 2 hour AIT.
The data will support a U.S. marketing application.
Related tickers: Abbott (NYSE:ABT), Tandem Diabetes Care (NASDAQ:TNDM), Insulet (NASDAQ:PODD)
Following up on their initial announcement in March, Roche (OTCQX:RHHBY) unit Genentech and U.S. commercialization partner AbbVie (NYSE:ABBV) announce positive results from a Phase 3 clinical trial, VIALE-A,
evaluating Venclexta (venetoclax) and chemo agent azacitidine in
previously untreated acute myeloid leukemia (AML) patients ineligible
for intensive chemo.
The study met both primary endpoints,
demonstrating statistically significant improvements in overall survival
(OS) (sole U.S. efficacy endpoint) and the proportion of patients
achieving complete remission (CR) and CR with incomplete blood count
recovery (CRi) compared to azacitidine + placebo.
Specifically, OS in the Venclexta + azacitidine
(V+a) arm was 14.7 months compared to 9.6 months in the azacitidine
alone arm (p<0.001). 64% of patients receiving V+a achieved CR + CRi
versus 28.3% of patients in the azacitidine group (p<0.001).
The companies are co-commercializing Venclexta in the U.S. while AbbVie has sole rights ex-U.S.
Cybercriminals could trace your device or access sensitive personal
data through contact-tracing apps built for the coronavirus pandemic, a
new report says. In a report released Thursday,
cybersecurity firm Check Point noted that U.S. developers are working
on contact tracing apps that measure Bluetooth signal strength to detect
the distance between device users. The basic idea is, if two devices
are close enough, within 6 feet, an infected user could potentially
transmit the virus. If somebody is infected, other app users would be
notified and could self-quarantine and get tested.
GPS can also be used to determine location. This approach allows
health authorities to analyze the geography of the infection spread and
take preventative measures. MIT’s SafePaths app, for example, uses GPS technology.
Checkpoint researchers laid out a number of concerns about the apps, including issues with the following:
Bluetooth: If not implemented correctly, hackers can trace a
person’s device by matching devices and the “identification packets”
they send out.
GPS: If GPS is used, it can give away sensitive information,
revealing where users are traveling and their location during previous
days or weeks.
Personal data: Apps store contact logs, encryption keys and other
sensitive data on devices. This data could be vulnerable if not
encrypted and stored in the application “sandbox.”
There is also a danger that identity could be exposed if phone
number, name or other identifying data is associated with a tracing app.
“The jury is still out on how safe contact tracing apps are. After
initial review, we have some serious concerns,” Jonathan Shimonovich,
Manager of Mobile Research at Check Point, said in a statement.
“Contact tracing apps must maintain a delicate balance between
privacy and security, since poor implementation of security standards
may put users’ data at risk,” he added.
Google and Apple made news in April when they announced
a framework based on Bluetooth for registration of contact events. Each
device generates keys to send to nearby devices and the devices store
the contact IDs locally.
According to the framework, if a user decides to report a positive
diagnosis of COVID-19 to their app, they will be added to the positive
diagnosis list – managed by a public health authority – so that other
users who came into range of the infected person’s Bluetooth “beacons”
can be alerted.
Check Point has offered some pointers on how you can protect yourself from exposing your data:
Install apps from reputable stores only such as the App Store and
Google Play Store. Those stores only allow authorized government
agencies to publish such apps.
Use mobile security: install mobile security software to scan applications and protect the device against malware.
US property and casualty insurers have cast the coronavirus pandemic as an unprecedented event whose massive cost to small businesses they are neither able nor required to cover.
The industry has warned it could cost them $255 billion to $431
billion a month if they are required, as some states are proposing, to
compensate firms for income lost and expenses owed due to virus-led
shutdowns, an amount it says would make insurers insolvent.
The estimate, made by the American Property Casualty Insurance
Association, a trade group, was recently used by the industry to
successfully lobby against state and city lawmakers’ efforts to
legislate to make the sector pay.
Insurers say business interruption policies only apply when actual
physical property damage prevents a business from operating and any
attempt to apply cover beyond that, for a pandemic, are
unconstitutional.
The stance has discouraged some policyholders from filing claims and prompted others to take legal action.
A Reuters examination of APCIA’s estimate, however, suggests the possible bill may not be so onerous.
The APCIA estimate is an industry worst-case scenario based on all
small firms with business interruption coverage being able to claim. It
also assumes that 60 percent to 90 percent of businesses with fewer than
100 employees will be affected by COVID-19.
Only about 40 percent of small firms have business interruption
coverage, according to the Insurance Information Institute, and most of
the policies explicitly exclude pandemics, according to Tyler Leverty
and Lawrence Powell, professors who specialize in insurance at the
University of Wisconsin and the University of Alabama, respectively.
Powell has estimated that insurers could be on the hook for a maximum
of $120 billion a month in claims on the basis that half of small firms
have business interruption insurance.
Leverty said that if the estimate counted only businesses without
explicit exclusions for pandemics, “it would be in the millions per
month.”
The APCIA said it stood by its numbers, which it said reflect the
unique and widespread impact of the virus. It declined to comment on
Powell’s analysis.
“Yes, these are eye-popping figures,” APCIA Chief Executive David
Sampson told Reuters, referring to the association’s estimate. “This
pandemic is unprecedented in its scale, reach, and economic impact.”
New Jersey’s business interruption bill, a model for others, is
stalled while Roy Freiman, the lawmaker who introduced it, waits for an
alternative plan from the industry.
“I said, ‘Look, we don’t want insolvency, but surely there is some
place between 100 percent denial and insolvency that you can operate
within,’” Freiman told Reuters.
The city council in Washington, DC, shelved a similar plan in early
May after “pretty intense” lobbying, Council Member Charles Allen, a
supporter, told Reuters. APCIA’s cost estimate was cited in council
discussions along with an association white paper describing the plan as
unconstitutional.
Chairman Phil Mendelson, who introduced the plan, withdrew it after
members voiced fears of a lengthy court fight and insurer insolvency.
“Obviously, our concerns were heard,” Sampson told Reuters at the time.
Trade groups say the industry’s stance has deterred many claims.
“Businesses are being told if you file they will probably deny you,”
Andrew Wrigie, executive director of the New York City Hospitality
Alliance, which represents 2,500 bars and restaurants in New York City, told Reuters.
“We’re telling them to seek counsel and be on record filing claims.”
That’s not an option for George Sizemore, owner of Bit of England Darts & Games Shoppe in Virginia Beach.
Sizemore’s insurance agent told him it would be pointless to claim
for the $40,000 in revenue he said he lost while his store was shut
because his policy does not cover pandemics.
“The only way I could file a claim would be to have a lawyer,” said Sizemore. “I just don’t have the money.”
There are currently dozens of lawsuits in US courts seeking compensation on behalf of small businesses for lost earnings due to the pandemic.
Legal experts said that while many policies exclude pandemics, some
do not and there is precedent for courts requiring insurers to pay for
physical loss without physical damage, such as when pollution or
asbestos make property uninhabitable.
“It’s not anywhere near as clear-cut as the industry says,” said John
Ellison, a partner at Reed Smith who has represented policyholders for
three decades. https://nypost.com/2020/06/12/small-businesses-dont-qualify-for-covid-19-claims-insurers/
Abstract Background: While several trials are ongoing for
treatment of COVID-19, scientific research on chemoprophylaxis is still
lacking even though it has potential to delay the pandemic allowing us
time to complete research on vaccines. Methods: We have conducted a
cohort study amongst Health Care Workers (HCW) exposed to COVID-19
patients, at a tertiary care center in India where there was an abrupt
cluster outbreak within on duty personnel. HCWs who had voluntarily
taken hydroxychloroquine (HCQ) prior to exposure were considered one
cohort while those who had not were considered to be another. All
participants with a verifiable contact history were tested for COVID-19
by rtPCR. The two cohorts were comparable in terms of age, gender,
comorbidities and exposure. The primary outcome was incidence rates of
rtPCR positive COVID-19 infection amongst HCQ users and non – users.
Results: 106 healthcare workers were examined in this cohort study of
whom 54 were HCQ users and rest were not. The comparative analysis of
incidence of infection between the two groups demonstrated that
voluntary HCQ usage was associated with lesser likelihood of developing
SARS-CoV-2 infection, compared to those who were not on it, X2=14.59,
p<0.001. None of the HCQ users noted any serious adverse effects.
Conclusions: This study demonstrated that voluntary HCQ consumption as
pre-exposure prophylaxis by HCWs is associated with a statistically
significant reduction in risk of SARS-CoV-2. These promising findings
therefore highlight the need to examine this association in greater
detail among a larger sample using Randomised Controlled Trials (RCT).
Migraine headaches are notoriously difficult to treat with pain
medications, which perform no better than placebo in studies. Now, a new paper in the journal Headache finds
that 83% of patients who completed a short course of cognitive
behavioral therapy (CBT) had fewer headaches. The researchers believe
that changes in a key brain area for pain management explains how CBT
helps with migraines. But what’s most interesting about these findings
is the way it challenges the way we classify these headaches in the
first place.
Migraines hurt. Badly. Patients often describe the throbbing
headaches as so painful, all they can do is lie down in a dark room. The
mainstay of treatment for migraines has long been medication, but
medications for acute migraines often don’t work. It gets even harder
when people have frequent or chronic migraines, where preventative
medicines are thought to work only about 20% of the time.
When medications don’t work, doctors prescribe other methods like
biofeedback training, acupuncture or stress reduction therapy. But
because migraine is considered a medical problem, these treatments are
second line.
Therapy for migraine headaches
That’s why this new study is so important. Most of the 18 adolescents
in the study with frequent migraine headaches saw a reduction in their
migraines. Unlike many studies which run special protocols that no one
can access outside the lab, this one used an easily available remedy.
Cognitive behavioral therapy is the one of most widely taught and
available types of psychotherapy in the U.S. today.
To sort out how the therapy might have helped, researchers ran MRIs
on the study participants both before and after their time in CBT. The
adolescents had 15 + or – 7.4 headaches a month before enrolling in the
study. They then participated in 8 weekly sessions of CBT. After the
eight weeks, their headache frequency decreased to 10 + or – 7.4 a
month.
The technical details: the MRIs were a particular type called
structural and resting-state blood-oxygen-level dependent contrast
scans. They also used arterial spin labeling to look at brain activation
during the resting state and compared the left and right amygdala to
assess connectivity. They also looked at voxels, or 3D pixels, across
the whole brain over time.
Therapy activated the brain’s pain control areas
After CBT, the scans showed greater brain activations in the frontal
regions associated with cognitive regulation of pain. So these were the
areas in the frontal cortex where we can consciously think about our
pain and cope with it. The MRIs also found increased connectivity
between the amygdala and frontal regions after CBT. So the amygdala,
which is the stress and raw emotion center of our brain, was talking
more with the frontal area where we can think through our pain.
In other words, cognitive behavioral therapy helped the part of our
brains that freaks out about pain listen to calming thoughts from the
brains’ higher levels.
That’s pretty cool. When medical problems are treated more
effectively by talk therapy than by medication, it raises questions
about the nature of the problem in the first place. It would be easy to
wonder if migraine headaches are really an emotional or psychosomatic
problem; an “all in our heads” sort of thing. It’s an old idea, passed
down from ancient Greek ideas that formed a foundation in western
culture: that the mind and body are separate. It leads us to ask
questions like, “Is this a medical problem or this is a psychological
problem?”
Mind and body are a single biological system
Studies like this highlight the growing understanding that there is
no separation between our minds and our bodies. Neither is there a
meaningful separation between our thoughts, emotions or our physical
symptoms.
We exist as one biological system with different access points.
That idea can be challenging at first. But once we wrap our minds
around it, humans make more sense. If we are a single interconnected and
unified system with lots of inputs and outputs, recent findings in
medical science stop seeming so weird.
Here’s one example: it’s a mind-bender to consider the role of the
gut microbiome. The “guest” bacteria living in our gut impact a host of
“separate” systems in our bodies. Evidence suggests that the population
makeup of gut bacteria determines whether we have inflammation that
leads to heart disease. AND those bacteria also impact our serotonin
levels, making us happy or depressed.
How can the bacteria in our gut be the reason we are depressed? We
have cherished the idea that depression is in the realm of mind and that
it’s something we can control. Yet recent science suggests that
organisms who live inside us are a big part of it. That only makes sense
if we think of our bodies and minds as a single system.
Going to talk to a therapist because you have migraines may be giving
you a lot more than just coping skills. It may be actually rewiring
your brain. https://www.forbes.com/sites/alisonescalante/2020/06/12/83-of-patients-had-fewer-migraine-headaches-after-doing-therapy/#63a50f96251f
Human medical trials have begun on severely ill COVID-19 patients using low-doses of radiation. The first results on a very small group
were published this week in a non-peer-reviewed journal that exists to
get critical results out quickly to the scientific and medical
community.
The results were quite extraordinary.
Researchers at Emory University Hospital, led by Dr. Mohammad Khan, Associate Professor of Radiation Oncology, treated five COVID-19 patients
with severe pneumonia who were requiring supplemental oxygen and whose
health was visibly deteriorating. Their median age was 90 with a range
from 64 to 94, four were female, four were African-American, and one was
Caucasian.
These patients were given a single low-dose of radiation (1.5 Gy) to both lungs, delivered by a front and back beam configuration. Patients were in an out of the Radiotherapy Department in 10 to 15 minutes.
Within 24 hours, four of the patients showed rapid improvement in
oxygenation and mental status (more awake, alert and talkative) and were
being discharged from the hospital 12 days later. Blood tests and
repeated imaging of the lungs confirmed that the radiation was safe and
effective, and did not cause adverse effects – no acute skin, pulmonary,
gastrointestinal or genitourinary toxicities. The gray (Gy) is a dose unit of ionizing radiation defined as the absorption of one joule of radiation energy per kilogram of matter. The Gy replaces the older unit of the rad, and 1 Gy = 100 Rad.
Potential role of low-dose radiation to combat the cytokine storm in severe pneumonia associated … [+]
George Wilson
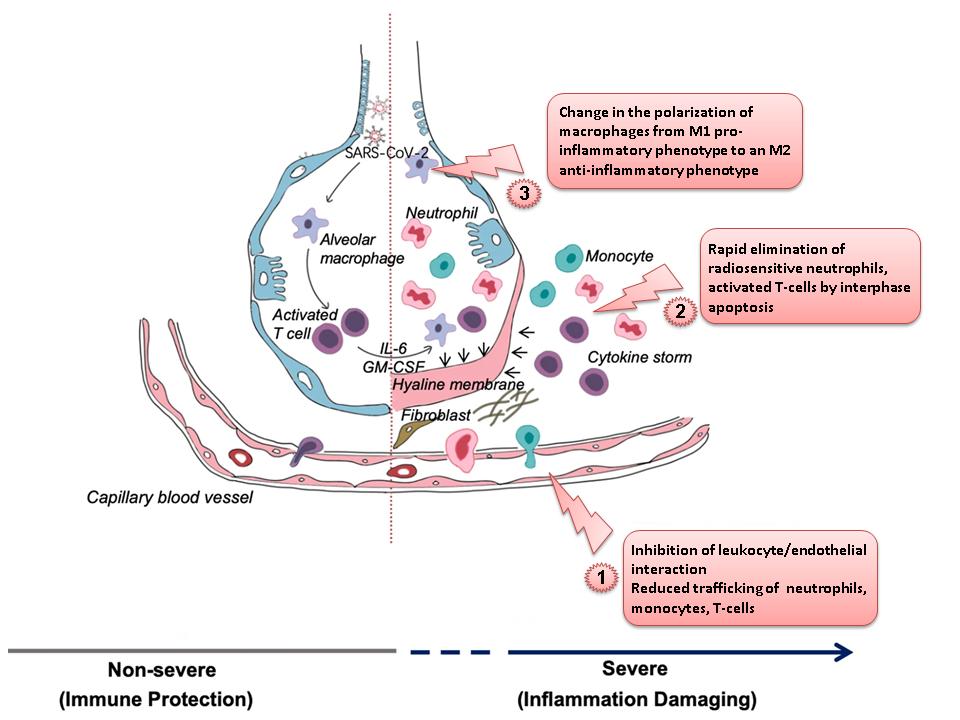
These studies indicated possible mechanisms by which low doses of
radiation mitigates inflammation and facilitates healing, one being the polarization of macrophages to an anti-inflammatory or M2 phenotype.
The M1 type tends to overstimulate the immune system which can lead to a
cytokine storm, while the M2 type tends to suppress the overreaction of
the immune system.
We kind of knew this would work because we did the same thing 70 to
80 years ago. Dr. E. J. Calabrese at the University of Massachusetts School of Public Health & Health Sciences and Dr. Gaurav Dhawan at the University of Massachusetts reviewedhow X-ray therapy was used during the first half of the 20th century to successfully treat pneumonia, especially viral pneumonia like that caused by this coronavirus.
As Welsh puts it, for COVID-19 patients who progress to severe
disease where there is no established treatment and death is a
significant possibility, low-dose radiation would appear to be a
relatively safe strategy that could be widely implemented, once evidence
of efficacy is produced. This can be readily achieved with small,
pragmatic and expeditious clinical trials, with an extremely rapid
clinical signal of benefit.
As the other human radiation trials move forward, it will be exciting
to see the results because we need an easy, quick and safe treatment
for the most dangerous virus of our time. https://www.forbes.com/sites/jamesconca/2020/06/12/1st-human-trial-successfully-treated-covid-19-using-low-doses-of-radiation/#195f75f0dc69