Florida Governor Ron DeSantis on Monday announced that the Florida Disaster Fund has raised$59.2 million for Hurricane Ian emergency relief, after claiming that the Biden administrationdenied funding assistance.
$25 million came from the state of Florida, while donors provided $35.2 million, DeSantis' office said in a press release. The state funds will be used to acquire building materials, while donations will enable "verified nonprofit organizations to conduct critical temporary repairs on homes damaged by Hurricane Ian," according to the press release, and reported by the Daily Caller.
The disaster funding will also address "unmet needs such as transportation, food assistance, housing aid, clothing, and household goods," according to the release.
"We are providing building materials and supporting nonprofit organizations to provide repairs so impacted residents can move back into their own homes," said DeSantis, adding "Floridians are resilient, and the state stands by them every step of the way as they continue their recovery.
Biden admin denied?
On Monday, DeSantis said that Florida was denied $25 million in emergency funds by the Federal Emergency Management Agency (FEMA).
(Perhaps Florida should change its name to Ukraine?)
Following the FEMA denial, DeSantis said "we’re not going to take no for an answer," adding "we want to cut bureaucracy."
According to the Caller:
FEMA denied the request because of its “limited authority” and “our inability to confirm that authorizing this policy expansion would achieve the intended outcomes for disaster survivors,” the agency said in a letter to Kevin Guthrie, Director of the Florida Division of Emergency Management.
The agency has provided $3.3 billion in federal support to Florida and households for Hurricane Ian relief, according to a Monday press release.
FEMA and the White House both did not immediately respond to requests for comment by the Daily Caller. Gov. DeSantis’ office did not immediately respond to a request for comment as well.
The Florida Disaster Fund - spearheaded by First Lady Casey DeSantis is the state's private fund, which was established to provide financial assistance to communities throughout the state during emergencies.
Many neurodegenerative diseases, or conditions that result from the loss of function or death of brain cells, remain largely untreatable. Most available treatments targetjust one of the multiple processesthat can lead to neurodegeneration, which may not be effective in completely addressing disease symptoms or progress, if at all.
But what if researchers harnessed thebrain's inherent capabilities to cleanse and heal itself? My colleaguesand Iin theLukens Labat the University of Virginia believe that the brain's own immune system may hold the key to neurodegenerativediseasetreatment. In ourresearch, we found a protein that could possibly be leveraged to help the brain'simmune cells, or microglia, stave off Alzheimer's disease.
Challenges in treating neurodegeneration
No available treatments for neurodegenerative diseases stop ongoing neurodegeneration while also helping affected areas in the body heal and recuperate.
In terms of failed treatments, Alzheimer's disease is perhaps the most infamous of neurodegenerative diseases. Affecting more than 1 in 9 U.S. adults 65 and older, Alzheimer's results from brain atrophy with the death of neurons and loss of the connections between them. These casualties contribute to memory and cognitive decline. Billions of dollars have been funneled into researching treatments for Alzheimer's, but nearly every drug tested to date has failed in clinical trials.
Another common neurodegenerative disease in need of improved treatment options is multiple sclerosis. This autoimmune condition is caused by immune cells attacking the protective cover on neurons, known as myelin. Degrading myelin leads to communication difficulties between neurons and their connections with the rest of the body. Current treatments suppress the immune system and can have potentially debilitating side effects. Many of these treatment options fail to address the toxic effects of the myelin debris that accumulate in the nervous system, which can kill cells.
A new frontier in treating neurodegeneration
Microglia are immune cells masquerading as brain cells. In mice, microglia originate in the yolk sac of an embryo and then infiltrate the brain early in development. The origins and migration of microglia in people are still under study.
Microglia play important roles in healthy brain function. Like other immune cells, microglia respond rapidly to pathogens and damage. They help to clear injuries and mend afflicted tissue, and can also take an active role in fighting pathogens. Microglia can also regulate brain inflammation, a normal part of the immune response that can cause swelling and damage if left unchecked.
Microglia also support the health of other brain cells. For instance, they can release molecules that promote resilience, such as the protein BDNF, which is known to be beneficial for neuron survival and function.
But the keystone feature of microglia are their astounding janitorial skills. Of all brain cell types, microglia possess an exquisite ability to clean up gunk in the brain, including the damaged myelin in multiple sclerosis, pieces of dead cells and amyloid beta, a toxic protein that is a hallmark of Alzheimer's. They accomplish this by consuming and breaking down debris in their environment, effectively eating up the garbage surrounding them and their neighboring cells.
Given the many essential roles microglia serve to maintain brain function, these cells may possess the capacity to address multiple arms of neurodegeneration-related dysfunction. Moreover, as lifelong residents of the brain, microglia are already educated in the best practices of brain protection. These factors put microglia in the perfect position for researchers to leverage their inherent abilities to protect against neurodegeneration.
New data in both animal models and human patients points to a previously underappreciated role microglia also play in the development of neurodegenerative disease. Many genetic risk factors for diseases like Alzheimer's and multiple sclerosis are strongly linked to abnormal microglia function. These findings support an accumulating number of animal studies suggesting that disruptions to microglial function may contribute to neurologic disease onset and severity.
This raises the next logical question: How can researchers harness microglia to protect the nervous system against neurodegeneration?
Engaging the magic of microglia
In our lab's recent study, we keyed in on a crucial protein called SYK that microglia use to manipulate their response to neurodegeneration.
Our collaborators found that microglia dial up the activity of SYK when they encounter debris in their environment, such as amyloid beta in Alzheimer's or myelin debris in multiple sclerosis. When we inhibited SYK function in microglia, we found that twice as much amyloid beta accumulated in Alzheimer's mouse models and six times as much myelin debris in multiple sclerosis mouse models.
Blocking SYK function in the microglia of Alzheimer's mouse models also worsened neuronal health, indicated by increasing levels of toxic neuronal proteins and a surge in the number of dying neurons. This correlated with hastened cognitive decline, as the mice failed to learn a spatial memory test. Similarly, impairing SYK in multiple sclerosis mouse models exacerbated motor dysfunction and hindered myelin repair. These findings indicate that microglia use SYK to protect the brain from neurodegeneration.
But how does SYK protect the nervous system against damage and degeneration? We found that microglia use SYK to migrate toward debris in the brain. It also helps microglia remove and destroy this debris by stimulating other proteins involved in cleanup processes. These jobs support the idea that SYK helps microglia protect the brain by charging them to remove toxic materials.
Finally, we wanted to figure out if we could leverage SYK to create "super microglia" that could help clean up debris before it makes neurodegeneration worse. When we gave mice a drug that boosted SYK function, we found that Alzheimer's mouse models had lower levels of plaque accumulation in their brains one week after receiving the drug. This finding points to the potential of increasing microglia activity to treat Alzheimer's disease.
The horizon of microglia treatments
Future studies will be necessary to see whether creating a super microglia cleanup crew to treat neurodegenerative diseases is beneficial in people. But our results suggest that microglia already play a key role in preventing neurodegenerative diseases by helping to remove toxic waste in the nervous system and promoting the healing of damaged areas.
It's possible to have too much of a good thing, though. Excessive inflammation driven by microglia could make neurologic disease worse. We believe that equipping microglia with the proper instructions to carry out their beneficial functions without causing further damage could one day help treat and prevent neurodegenerative disease.
More information: Hannah Ennerfelt et al, SYK coordinates neuroprotective microglial responses in neurodegenerative disease, Cell (2022). DOI: 10.1016/j.cell.2022.09.030
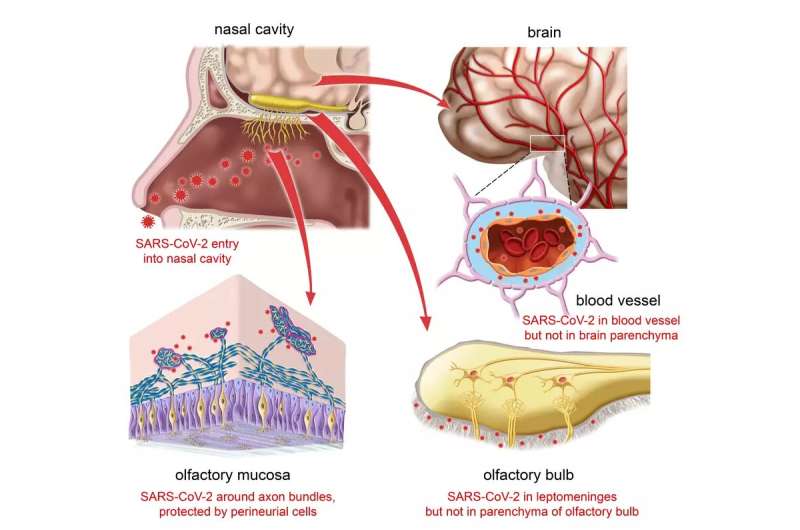
A common symptom of COVID-19 is a partial or complete loss of smell. The virus infects sustentacular cells in the olfactory epithelium and is thought to impair thereby the activity of the sensory neurons in this epithelium.
Scientists at the Max Planck Research Unit for Neurogenetics in Frankfurt in collaboration with physicians and scientists at the University Hospitals Leuven (Leuven, Belgium) and hospitals in Bruges and Brussels, Belgium, have now examined tissue samples of nasal mucosa andbrainof patients who died from or with a SARS-CoV-2 infection, including the delta, omicron BA.1 or BA.2 variants.
In a total of more than a hundred COVID-19 patients, the scientists failed to find evidence for viral invasion of the brain. A poorly characterized type of fibroblasts in the olfactory mucosa appears to act as one of several anatomical barriers that shield the brain from the virus at vulnerable interfaces.
Anosmia occurs often after infection with SARS-CoV-2, ranging from a temporary impairment to a persistent, possibly permanent, loss of smell. The nasal mucosa represents one of the main entry sites of the virus. Early in the pandemic, the suspicion arose that the virus might infect cells of the olfactory epithelium, hitchhike on the olfactory nerve, and then infect or invade the brain via the nearby olfactory bulb, which is located only a few millimeters from the nasal cavity.
But this suspicion has not been confirmed. In November 2021, scientists at the Max Planck Research Unit for Neurogenetics in Frankfurt, together with physicians and scientists in Leuven and Bruges, Belgium, reported that SARS-CoV-2 infects the sustentacular cells (supporting cells) of the olfactory epithelium, but not the sensory neurons. The researchers were unable to detect the virus in the olfactory bulb.
The physicians had developed a bedside surgical procedure to collect tissue samples from deceased patients. With this new procedure, they were able to harvest, within an hour or two after the time of death, tissue samples of respiratory mucosa, olfactory mucosa, and the frontal lobe of the brain, as well as whole olfactory bulbs, in a cohort of 70 COVID-19 patients. This unusually short postmortem interval makes the tissue samples highly suitable for molecular and histological studies.
SARS-CoV-2 infects the respiratory epithelium, but not the brain. Credit: P. Meeze and M. Khan
All brain samples were negative
Now the team has examined tissue samples obtained from a second cohort of 45 COVID-19 patients who had died within two weeks after diagnosis and were infected with the delta, omicron BA.1 or BA.2 variants. They also analyzed tissue samples of the frontal lobe of the brain of most COVID-19 patients from the first cohort, who were infected with non-variants of concern or the alpha variant.
"We examined microscopically the olfactory bulbs and the frontal lobe samples for viral nucleic acid and protein. All samples were negative: no neurons were infected. Moreover, by trying to culture SARS-CoV-2 from cerebrospinal fluid samples, we could not find evidence that SARS-CoV-2 had invaded the brain," says Peter Mombaerts of the Max Planck Research Unit for Neurogenetics.
Adds Laura Van Gerven, ENT surgeon at the University Hospitals Leuven, Belgium, "SARS-CoV-2 would have the greatest chance of displaying its hypothetical neurotropic or neuroinvasive capacity in these highly vulnerable patients, with a colossal failure of the host defense and the gravest outcome of all."
The so-called perineurial fibroblasts of the olfactory nerve—thin, elongated cells whose function is not known—apparently act as a protective anatomical barrier. They wrap around the olfactory nerve bundles in one or more densely packed layers.
"We do not know how these cells prevent the virus from invading the olfactory nerve bundles. But they seem instrumental in preventing SARS-CoV-2—and possibly some of the many other pathogens that infect the nasal mucosa—from invading the brain," Mombaerts explains.
The paper is published in the journal Neuron. The new results do not support the suspicion that SARS-CoV-2 infects brain cells and invades the brain. The findings have implications for the mechanisms of long COVID.
More information: Mona Khan et al, Anatomical barriers against SARS-CoV-2 neuroinvasion at vulnerable interfaces visualized in deceased COVID-19 patients, Neuron (2022). DOI: 10.1016/j.neuron.2022.11.007
A drug in development for obstructive sleep apnea (OSA) has shown promising results, after researchers from Flinders University tested the treatment in people for the first time.
Designed to prevent the narrowing or collapse of the upper airways during sleep, a key factor in OSA, the treatment could prove to be a potential alternative for certain people with OSA tocontinuous positive airway pressure(CPAP) machines, which can only be tolerated by about half of all OSA sufferers.
"While further rigorous clinical evaluation and testing is required, this is a great first step and should offer some hope to the many people worldwide who suffer from sleep apnea," says study senior author Professor Danny Eckeart, Director of Flinders' sleep lab FHMRI: Sleep Health.
"OSA is one of the most common sleep-related breathing disorders, with an estimated one billion sufferers, and when untreated is associated with major health and safety consequences. While CPAP machines are effective, tolerance remains a major issue for many and other treatments such as dental splints and upper airway surgery don't always work. This is why we need new treatment options for OSA.
"At the moment, there are no approved drug treatments for OSA. However, with advances in our understanding of the different reasons people get OSA, the potential for effective new medications is growing stronger each year."
Published in the journal Chest, the study tested the drug on 12 people with OSA using either nasal drops, a nasal spray or via direct application using an endoscope, versus a placebo.
Monitoring for sleep and airway activity across several sessions, the team found consistent and sustained improvements in the patients' airways staying open throughout sleep, compared to the placebo treatment, regardless of the delivery method used.
"Although a small study, our findings represent the first detailed investigation of this new treatment in people with OSA, with promising results," says study lead author Dr. Amal Osman from FHMRI: Sleep Health.
"The drug we tested is designed to target specific receptors that are expressed on the surface of the upper airways, triggering them more easily to activate the surrounding muscles to keep the airway open during sleep. While there's still a long way to go in terms of clinical testing and development, our study shows targeting these receptors may be a promising avenue for future treatments."
More information: Amal M. Osman et al, Topical K+ channel blockage improves pharyngeal collapsibility: A translational, placebo-controlled trial, Chest (2022). DOI: 10.1016/j.chest.2022.11.024
Former NFL players may have shorter health spans—defined as absence of age-related disease—compared with men in the general population, according to a new study. Credit: Rachel Grashow, Harvard T.H. Chan School of Public Health
Former professional football players—particularly linemen—are more likely than nonplayers with similar demographic characteristics to develop diseases typically associated with advanced age when significantly younger, according to new research published Dec. 8 in the British Journal of Sports Medicine.
These former elite athletes also tend to experience age-related conditions—hypertension and diabetes, among others—earlier, compared with the general population. Looking across all conditions, these athletes' health spans were reduced by nearly a decade.
Notably, the effects persisted even after the researchers accounted for body mass index and race, two powerful risk factors for the diseases studied.
The research—based on a survey of nearly 3,000 former National Football League players, representing the largest study cohort of former professional football players to date—was conducted by investigators at the Harvard T. H. Chan School of Public Health and Harvard Medical School as part of the ongoing Football Players Health Studyat Harvard University, a research program that encompasses a constellation of studies designed to evaluate various aspects of players' health across their life span.
The findings, the research team said, warrant further study to define the biochemical, cellular, and physiologic mechanisms behind this premature aging phenomenon.
"Our analysis raises important biological and physiological questions about underlying causes but, just as importantly, the results should serve as an alarm bell telling clinicians who care for these individuals to pay close attention even to their relatively younger former athlete patients," said study senior investigator Rachel Grashow, director of epidemiological research initiatives for the Football Players Health Study.
"Such heightened vigilance can lead to earlier diagnoses and timelier intervention to prevent or dramatically slow the pace of age-related illness,"
This level of attention is important because chronic conditions such as diabetes or hypertension, for example, could be easily overlooked due to a former player's status as an elite athlete, Grashow added.
Although previous studies had shown that former professional football players live as long or longer than males in the general population, athletes themselves reported to their physicians that they often feel older than their chronologic age. In addition, sports medicine physicians who treat players have reported that these athletes often experience an earlier onset of age-related chronic conditions such as dementia, arthritis, hypertension, and diabetes.
Intrigued by these conflicting reports, Grashow and colleagues surveyed 2,864 Black and white former professional football players between the ages of 25 and 59 to determine whether a health care provider had ever told them that they had dementia/Alzheimer's disease, arthritis, hypertension, or diabetes. In addition, the researchers used survey data to measure participants' health spans, or how long these athletes lived without developing any of these four conditions.
The researchers compared these results to data from men aged 25 to 59 in the general population derived from two large, nationwide studies: the National Health and Nutrition Examination Survey and the National Health Interview Survey, which collectively hold information on tens of thousands of individuals.
Not surprisingly, the analysis showed that all four conditions increased with age in both the former football players and in the general population. However, the prevalence of these conditions, or the proportion of individuals who had them, differed significantly between the two groups.
In each decade of life, the former athletes were more likely to report that they'd been diagnosed with dementia/Alzheimer's disease and arthritis. For hypertension and diabetes, only the younger players, those aged 25 to 29, reported significantly higher numbers of diagnoses compared with the general population.
Importantly, the health span for each former NFL player age group most closely resembled American men a decade older. For example, 66 percent of the former players in the 30 to 39 age group reported an intact health span, compared with 62 percent of men in the general population ages 40 to 49.
Searching for game-related aspects that might be important for this premature emergence of aging diseases, the researchers separated data from the former football players group into linemen and non-linemen. This analysis showed that linemen, who experience more contact during games than non-linemen, had notably shorter health spans across all decades of life. This subgroup tended to develop age-related diseases sooner than their non-linemen peers.
"We wanted to know: Are professional football players being robbed of their middle age? Our findings suggest that football prematurely weathers them and puts them on an alternate aging trajectory, increasing the prevalence of a variety of diseases of old age," Grashow said. "We need to look not just at the length of life but the quality of life. Professional football players might live as long as men in the general population, but those years could be filled with disability and infirmity."
Metabolic conditions such as hypertension and diabetes could have dangerous long-term effects on heart health and cognition that could be mitigated with early diagnosis and treatment, said study senior author Aaron Baggish, director of in-person assessment studies at the Football Players Health Study and former director of Massachusetts General Hospital's Cardiovascular Performance Program, which provides comprehensive cardiac care to athletes.
"The duration of one's life is very important, but so too is the quality of one's life," added Baggish, who is currently professor of medicine at the University of Lausanne in Switzerland. "This study was conducted to probe the latter and now provides an important perspective on how early-life participation in the great game of football may accelerate the onset of certain common forms of chronic disease."
Grashow noted that future studies will focus on the biological mechanisms that give rise to premature aging among former professional football players, as well as interventions that can help these athletes live healthier lives as they age.
More information: Rachel Grashow et al, Healthspan and chronic disease burden among young adult and middle-aged male former American-style professional football players, British Journal of Sports Medicine (2022). DOI: 10.1136/bjsports-2022-106021
Usually, the scariest part of childhood vaccination, for both kids and parents, is the needles. In rare cases, however, vaccines can have unexpectedly negative effects, and the secret lies in our genes.
In a study published recently in theJournal of Clinical Immunology, researchers from Tokyo Medical and Dental University (TMDU) have revealed three previously unknown variants that can cause a severe reaction to a normal childhood vaccine.
In countries where tuberculosis is common, children often receive the bacillus Calmette-Guérin (BCG) vaccine to protect them from getting infected. Some cases, however, show an unexpectedly negative reaction to the BCG vaccine, due to a condition known as Mendelian susceptibility to mycobacterial disease (MSMD). The BCG vaccine in children with MSMD can cause swollen lymph nodes, inflamed bone tissue, and abscesses.
"Adverse reactions to the BCG vaccine are known to be associated with inherited variants in genes involved in the immune response," says lead author of the study, Rintaro Ono. "Thus, when we encountered four pediatric patients who exhibited signs of mycobacterial disease after BCG vaccination, we analyzed their genome to determine what mutations were responsible for this reaction."
To do this, the research team collected blood samples from the children and their immediate relatives and sequenced their genomic DNA to identify variants in genes related to immunity. They then tested the effects of the identified variants in the lab to determine the functional consequences of the variants.
"The results were somewhat unexpected," explains Hirokazu Kanegane, senior author. "While the variants that we found were in a gene called STAT1, which is often mutated in patients with MSMD, three out of the four variants that we identified have never been seen before."
Functional analysis of these three new variants demonstrated that they resulted in loss of function of the STAT1 protein, which made it unable to activate an appropriate immune response to the vaccine. Importantly, the variants show dominant negative, which means that the products of these mutated genes prevent the products of the wild-type gene (also known as natural form) from carrying out their normal activities—all in the same cell.
These findings suggest that heterozygous dominant negative variants in STAT1 may be a common cause of MSMD in Japanese patients. Given that the initial symptoms of MSMD (such as fever) are common in children, but can be severe or prolonged in patients with MSMD, it is important to monitor these patients closely after BCG vaccination. Careful follow-up and evaluation for STAT1 variants, such as those identified in this study, may enable these patients to be diagnosed and treated earlier.
More information: Rintaro Ono et al, Novel STAT1 Variants in Japanese Patients with Isolated Mendelian Susceptibility to Mycobacterial Diseases, Journal of Clinical Immunology (2022). DOI: 10.1007/s10875-022-01396-1
Investigators from the Smidt Heart Institute at Cedars-Sinai have found that even subtle forms of liver disease directly impact heart health. The findings, recently published in the journalFrontiers in Cardiovascular Medicine, help further clarify the relationship between liver disease and heart disease beyond their shared risk factors.
In the retrospective study, investigators compared patients' FIB-4 scores—a marker forliver fibrosisthat can indicate risk of developing severe liver disease—withheart abnormalitiesvisible through cardiac MRI scans. They found that elevated FIB-4 scores were associated with abnormalities in heart function and vascular dimension.
Alan Kwan, MD, a cardiologist and cardiac imaging researcher in the Smidt Heart Institute as well as lead and corresponding author of the study, said it had been known that nonalcoholic fatty liver disease was associated with cardiovascular death, but the relationship was poorly understood and possibly obscured by risk factors the two have in common, such as diabetes.
Previous similar studies had been limited in scope, looking only at how cirrhosis and nonalcoholic fatty liver disease affect the heart.
Earlier this year, the American Heart Association (AHA) released a statement that nonalcoholic fatty liver disease—an increasingly common liver condition that affects more than one in four adult Americans—is a risk factor for atherosclerotic cardiovascular disease.
And surprisingly, heart disease—not progression of liver disease—is the leading cause of death in people with nonalcoholic fatty liver disease, according to the AHA.
"If 25% of the population has this potential risk factor for cardiac disease, we knew we needed to understand it more fully," Kwan said. "So, our overall aim with this study was to examine the connections between the heart and the liver—a newer area of study, but one that made sense to explore further. The liver processes cholesterol and produces factors involved in blood clotting and inflammation—all of which can affect the heart—so we wanted to take a closer look at these associations."
To conduct the study, investigators reviewed electronic medical records from the past 11 years of 1,668 patients who had low, moderate or high FIB-4 scores within one year of having a cardiac MRI, adjusting for standard cardiovascular risk factors. They found that nearly 86% of patients had at least one heart abnormality.
Cardiac MRI provides a unique view of the heart, using detailed imaging that can identify subtle changes in heart structure, function, blood vessel size and structure, heart muscle composition, and more.
"The abnormalities we saw were vascular changes—enlargement of the blood vessels coming out of heart as well as an increase in how much blood was moving," Kwan said.
"Typically, when physicians examine the heart, we aren't thinking about the liver, and vice versa. We tend to be very specialized in our own organ categories. But this study's findings indicate that we can and should screen for liver conditions when looking at heart conditions—we can't view the heart and the liver as completely separate organs functioning on their own islands."
The next step in the research, Kwan said, is to further explore the impact that liver disease can have on heart health.
"Also, other questions come to light," he said, "such as, when treating people with nonalcoholic fatty liver disease, could medications to treat this also help the heart? Or, when you see your cardiologist or primary care physician and risk factors such as high cholesterol, blood pressure, diabetes and family history are discussed, should nonalcoholic fatty liver disease also be a standard risk factor to consider?"
Susan Cheng, MD, MPH, director of the Institute for Research on Healthy Aging in the Department of Cardiology at the Smidt Heart Institute and senior and co-corresponding author of the study, agreed that there are multiple reasons to continue research in this area.
"If we can understand the basic science of how the liver affects the heart, we can likely better understand other heart and organ interactions," said Cheng, who also holds the Erika J. Glazer Chair in Women's Cardiovascular Health and Population Science. "This could also shed light on directions for potential future targeted therapies to prevent cardiovascular disease in patients with liver disease."
Other Cedars-Sinai investigators who worked on this study include Nancy Sun, MPS; Matthew Driver, MPH; Patrick Botting, MSPH; Jesse Navarrette, MPA; David Ouyang, MD; Mazen Noureddin, MD; Debiao Li, Ph.D.; Joseph Ebinger, MD; and Daniel Berman, MD.
More information: Alan C. Kwan et al, Cardiovascular and hepatic disease associations by magnetic resonance imaging: A retrospective cohort study, Frontiers in Cardiovascular Medicine (2022). DOI: 10.3389/fcvm.2022.1009474