A work of art created by artificial intelligence without any human input cannot be copyrighted under U.S. law, a U.S. court in Washington, D.C., has ruled.
Only works with human authors can receive copyrights, U.S. District Judge Beryl Howell said on Friday, affirming the Copyright Office's rejection of an application filed by computer scientist Stephen Thaler on behalf of his DABUS system.
The Friday decision follows losses for Thaler on bids for U.S. patents covering inventions he said were created by DABUS, short for Device for the Autonomous Bootstrapping of Unified Sentience.
Thaler has also applied for DABUS-generated patents in other countries including the United Kingdom, South Africa, Australia and Saudi Arabia with limited success.
Thaler's attorney, Ryan Abbott, on Monday said that he and his client strongly disagree with the decision and will appeal. The Copyright Office in a statement on Monday said it "believes the court reached the correct result."
The fast-growing field of generative AI has raised novel intellectual property issues. The Copyright Office has also rejected an artist's bid for copyrights on images generated through the AI system Midjourney despite the artist's argument that the system was part of their creative process.
Several pending lawsuits have also been filed over the use of copyrighted works to train generative AI without permission.
"We are approaching new frontiers in copyright as artists put AI in their toolbox," which will raise "challenging questions" for copyright law, Howell wrote on Friday.
"This case, however, is not nearly so complex," Howell said.
Thaler applied in 2018 for a copyright covering "A Recent Entrance to Paradise," a piece of visual art he said was created by his AI system without any human input. The office rejected the application last year and said creative works must have human authors to be copyrightable.
Thaler challenged the decision in federal court, arguing that human authorship is not a concrete legal requirement and allowing AI copyrights would be in line with copyright's purpose as outlined in the U.S. constitution to "promote the progress of science and useful arts."
Howell agreed with the Copyright Office and said human authorship is a "bedrock requirement of copyright" based on "centuries of settled understanding."
Tonix Pharmaceuticals CEO Dr Seth Lederman joined Steve Darling from Proactive to announce the company has initiated a Phase 1 clinical study involving TNX-1500 in healthy volunteers, focusing on single ascending dose escalation.
The primary objectives of this study are to assess the safety, tolerability, pharmacokinetics, and pharmacodynamics of intravenous TNX-1500. TNX-1500 is a pharmaceutical product under development for the prevention of kidney transplant rejection, as well as other potential indications related to transplantation and autoimmune disorders.
Lederman highlighted that recent animal studies have shown promising results, indicating that TNX-1500 has the potential to prevent organ rejection and maintain graft function, either as a standalone treatment or when combined with other drugs.
The Phase 1 study will involve the evaluation of eligible participants over a 120-day period after dosing, with a target enrollment of 36 participants. The initiation of this Phase 1 study is a crucial step towards supporting the dosing regimen for an upcoming Phase 2 trial involving kidney transplant recipients.
Tonix Pharmaceuticals is optimistic about TNX-1500's potential to improve long-term graft survival with reduced toxicity compared to current immunosuppressive treatments.
Additionally, the company believes that TNX-1500 could address various indications, including autoimmune diseases beyond transplantation.
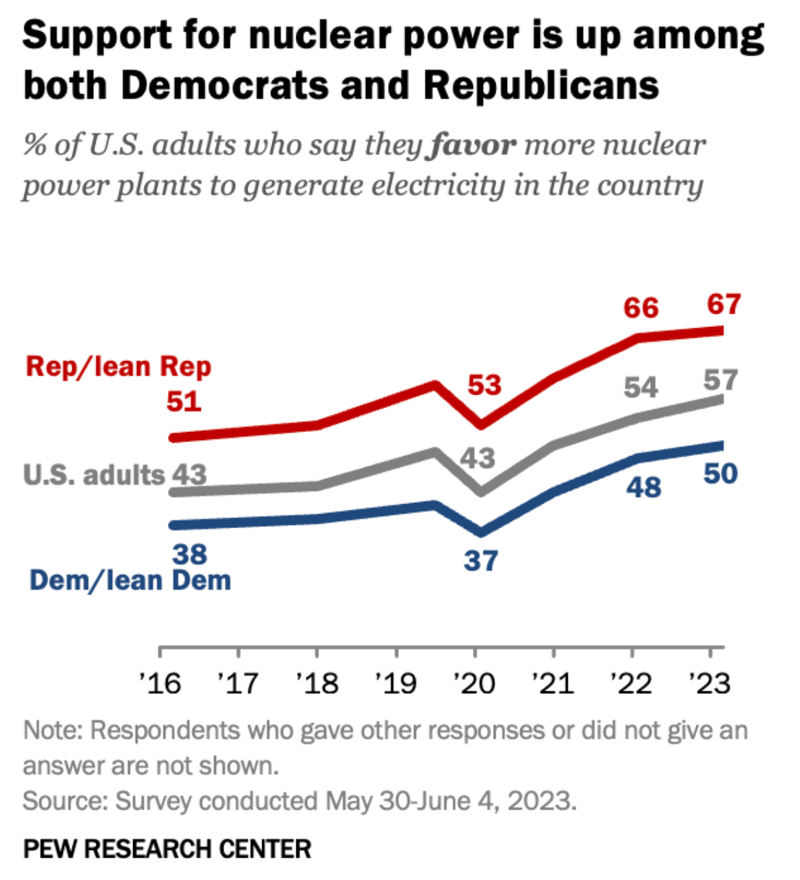
Several months after Elon Musk shared his thoughts on X (previously Twitter), advocating for greater use of nuclear power in response to a Times Magazine article featuring J. Robert Oppenheimer's grandson's views on nuclear's role in a net zero-carbon economy, a Pew Research Center survey noted a rise in the number of Americans supporting nuclear power.
About 57% of Americans (a majority) say they now favor nuclear power generation plants nationwide, up 14 percentage points since 2020, according to Pew. This dramatic rise in just a few short years as demand for electricity with the 'electrify everything' push, including in transportation, soars.
Every 4 years, an interprofessional panel of experts from the American Geriatrics Society provides updated guidelines on safe prescribing of medications in older adults, known as theBeers Criteria. A 2023 update was released in May 2023 after panel review of more 1,500 clinical trials and research studies published since the last update.
Anticoagulants
Notable changes to the 2023 guidelines include updated recommendations for anticoagulation. Warfarin should be avoided as initial therapy for venous thromboembolism or nonvalvular atrial fibrillation unless there are contraindications to direct oral anticoagulants (DOACs) or other substantial barriers to use.
Rivaroxaban should also be avoided, and dabigatran used with caution in favor of apixaban, which is felt to have a better safety profile in older adults. Rivaroxaban may be considered if once daily dosing is deemed to be more clinically appropriate. Financial barriers regarding drug coverage and formulary options were acknowledged as a significant barrier to equitable access to preferred direct oral anticoagulants in older adults.
Diabetes medication
Regarding diabetes management, short-acting sulfonylureas should be avoided in addition to long-acting sulfonylureas, because of the increased risk of hypoglycemia, and cardiovascular and all-cause mortality in older adults. Sodium-glucose cotransporter 2 inhibitors as an entire class are recommended to be used with caution, as older adults are at higher risk of euglycemic ketoacidosis and urogenital infections, particularly in women in the first month of initiating treatment.
Like DOACs, the panel acknowledged that financial considerations may lead to limited options for oral diabetic treatment. In circumstances where a sulfonylurea is used, short-acting forms are preferred over long acting to reduce the risk of prolonged hypoglycemia.
Aspirin for primary prevention
Alongside the U.S. Preventive Services Task Force guideline update in 2022 regarding aspirin for primary prevention of cardiovascular disease and stroke, the Beer's Criteria recommend against initiation of aspirin for primary prevention in older adults. Ticagrelor and prasugrel should be used with caution because of the increased risk of major bleeding in older adults over the age of 75, compared with clopidogrel. If prasugrel is used, a lower dose of 5 mg is recommended, in line with guidelines by the American College of Cardiology and American Heart Association.
Pain medication
For pain management, the Beer's Criteria updated recommendations to avoid NSAIDs, particularly when used in combination with steroids or anticoagulants. The panel highlights that even short-term use of NSAIDs is high risk when used in combination with steroids or anticoagulants. If no other alternatives are possible, patients should be placed on a proton pump inhibitor or misoprostol while taking NSAIDs.
Baclofen should be avoided in older adults with renal insufficiency (estimated glomerular filtration rate < 60 mL/min per 1.73 m2) because of the increased risk of encephalopathy, and when used, should be given at the lowest effective dose with close monitoring for mental status changes.
Androgen and estrogen replacement therapy
For androgen replacement therapy, the panel notes that testosterone supplementation should be avoided because of cardiovascular risks unless there is confirmed hypogonadism. The panel revised their recommendation on the basis of emerging data that a history of prostate cancer is not an absolute contraindication for exogenous testosterone. A risk versus benefit discussion about exogenous testosterone should be had with a medical oncologist or urologist in those with a history of prostate cancer.
Regarding estrogen, systemic formulations should not be initiated in women over the age of 60 because of increased risk of cardiovascular events, venous thromboembolism, and dementia. In women with a history of breast cancer, vaginal estrogens are generally felt to be safe to use at low doses, such as less than 25 mcg twice weekly.
An insurance industry lobbying campaign persuaded federal officials to allow insurers to charge physicians fees for the privilege of being paid electronically, even though it can cost more to mail paper checks, according to anew investigationby the nonprofit news organization ProPublica.
The Affordable Care Act requires that health plans give providers the option of being paid electronically to improve efficiency and save money. In 2017, the Centers for Medicare & Medicaid Services (CMS) issued guidance that prohibited insurers and their payment processing vendors from "engaging in unfair business practices that do not support an efficient healthcare system," according to a recent Medical Group Management Association (MGMA)position paper.
But that guidance, which appeared to forbid requiring fees to receive payments online, disappeared from the CMS site 6 months later.
According to ProPublica's reporting, the change was the result of a quiet insurance industry lobbying campaign led by Matthew Albright, a former CMS employee who left government service to work for Zelis, a payment processing company co-owned by private equity giant Bain Capital.
The details of the lobbying effort were discovered by Alex Shteynshlyuger, a New York urologist, who through public records requests received the email correspondence between Albright and CMS and shared that material with ProPublica.
Albright had been able to influence CMS policy to protect what ProPublica called a "crucial revenue stream" for payment processors. The fee notice was removed just 3 days after Albright requested the change, ProPublica found.
When CMS resisted further changes, including eliminating guidance forbidding insurers and payment processors from charging excess fees for online payments, Albright brought in a law firm. The threat of a lawsuit by deep-pocketed Zelis was enough to bring CMS in line, ProPublica reported. Today, these fees can cost larger medical practices more than $1 million a year, according to the MGMA report.
"[I]t took less than a decade for a new industry of middlemen, owned by private equity funds and giant conglomerates like UnitedHealth Group, to cash in," writes Cezary Podkul, the author of the ProPublica report.
It might seem that avoiding the fees would be as simple as requesting to be paid by check. However, a 2021 poll by the MGMA found that 57% of doctors were being charged these fees when they hadn't agreed to them. According to the ProPublica report, physicians who have requested to be paid by check often find themselves being bounced back to electronic fund transfer (EFT) payments, where they are again charged fees.
In October 2021, more than 90 physician organizations, including the American Medical Association and the MGMA, signed a letter calling on the Biden administration to reinstate guidance to protect physicians' right to receive EFT payments without paying fees. The letter describes the practice as "outrageous" and analogous to "an employee being required to enroll in a program that would deduct a percentage of each paycheck to receive direct deposit payments from an employer."
So far, however, the situation remains unchanged. The language on the CMS site has changed, though. In 2022, the guidelines were adjusted to clarify that EFT fees are allowed.
The US Supreme Courteffectively prohibited university admissions officers from giving preferential treatment to applicants based on their race this summer.
Many medical-school leaders decried the high court’s ruling, claiming the ban will lead to less diversity within their student bodies, a less diverse crop of physicians and worse outcomes for minority patients.
But it’s not clear diversity within the physician workforce improves patient outcomes — which ought to be the primary objective of medical education.
In fact, there’s evidence affirmative-action policies can harm patients as well as aspiring doctors themselves.
It’s an article of faith among affirmative action’s defenders that a more diverse physician workforce benefits patients.
In her dissent from the majority’s ruling, Justice Sonia Sotomayor wrote that affirmative action helps increase “the number of students from underrepresented backgrounds” who become doctors, which in turn “improves ‘healthcare access and health outcomes in medically underserved communities.’”
The Association of American Medical Colleges echoed Sotomayor, saying it was “deeply disappointed” in the majority’s ruling, which “demonstrates a lack of understanding of the critical benefits of racial and ethnic diversity.”
Many medical-school leaders decried the high court’s ruling, claiming the ban will lead to less diversity within their student bodies, a less diverse crop of physicians and worse outcomes for minority patients.Joe Carrotta / NYU Langone Health
“This decision will hasten the deaths of Black people in this country and we already die prematurely,” Advancing Health Equity founder and physician Uché Blackstock blasted.
They’re referring in part to a handful of studies showing black Americans post better health outcomes when treated by black doctors.
But researcher Ian Kingsbury recently examined those studies’ methodologies and concluded that “systematic reviews” have “found ‘no relationship’ or ‘mixed results’ between race/ethnicity and quality of communication and ‘inconclusive’ evidence for patient outcomes.”
Admissions officers’ obsessive focus on race often causes them to ignore applicants’ academic and clinical aptitude — with dire consequences for the applicants themselves and ultimately the patients they treat.
Justice Sonia Sotomayor said affirmative action helps “the number of students from underrepresented backgrounds” who become doctors as it “improves ‘healthcare access and health outcomes in medically underserved communities.’”AP
Affirmative-action policies seek to give underrepresented groups a leg up in the admissions process.
By design, that means admitting applicants who likely would have been rejected based on their test scores and grade-point averages alone.
From 2013 to 2016, 56% of black applicants and 31% of Hispanic applicants with below-average Medical College Admission Test scores and undergraduate GPAs were admitted to medical school, compared with just 8% of white applicants and 6% of Asian applicants with similar scores and GPAs.
It has been exhaustively documented that undergraduate “GPAs and MCAT total scores are strong predictors of academic performance in medical school through graduation,” as one study from the Association of American Medical Colleges itself put it.
The Association of American Medical Colleges echoed Sotomayor, saying it was “deeply disappointed” in the majority’s ruling, which “demonstrates a lack of understanding of the critical benefits of racial and ethnic diversity.”AP
In other words, affirmative action might help underqualified applicants get into med school.
But it won’t necessarily keep them there.
Black medical school students drop out, citing academic problems, at a rate 10 times higher than white students.
It’s cruel — not compassionate — to admit students who aren’t qualified for the intellectual rigors of medical school.
It sets them up for failure, saddles them with debt they could have avoided and wastes resources that could have gone towards training qualified applicants who will actually practice medicine.
Worst of all, admitting underqualified students ultimately hurts patients.
“MCAT scores are predictive of student performance” on both Step 1 and Step 2 of the US Medical Licensing Examination, concluded one 2016 study.
Those licensing exams, in turn, are indicative of students’ skill at treating patients during their clinical rotations.
“USMLE scores have a positive linear association with clinical performance as a medical student,” noted a 2019 study, “even after correcting for gender, institution, and test-taking ability.”
The relationship holds after students graduate, complete residencies and become practicing physicians.
A 2014 study of US-licensed doctors who trained overseas found that “after adjustment for severity of illness, physician characteristics, and hospital characteristics, performance on Step 2” had “a statistically significant inverse relationship with mortality. Each additional point on the examination was associated with a 0.2% decrease in mortality.”
The purpose of medical school is not to maximize diversity.
It’s to transform America’s best and brightest students into the most competent physicians possible, no matter their race, gender or any other demographic consideration.
Doctors hold people’s lives in their hands.
It should not matter what color those hands are.
Sally C. Pipes is president, CEO and Thomas W. Smith fellow in health-care policy at the Pacific Research Institute and founder and chairman of the Benjamin Rush Institute. Her latest book is “False Premise, False Promise: The Disastrous Reality of Medicare for All.”