by Paul D. Thacker
Senior officials inside the NIH are working to shut down a Tony Fauci initiative launched in 2020 called the Centers for Research in Emerging Infectious Diseases or “CREID.” Meanwhile, attorneys inside the Justice Department have launched initial inquiries into one of the CREID grants awarded to Scripps Research Institute researcher Kristian Andersen, who is now in the process of fleeing the United States for a position being created for him at the University of Oslo.
NIH Director Jay Bhattacharya did not respond to repeated requests for comment, but an NIH spokesperson confirmed the agency is shutting down the CREID grants. “Though the grants have been properly terminated, money will be released to the grantees to assure safe shutdown of these programs in terms of biosafety and security,” said an NIH spokesperson, adding that pandemic preparedness remains important but the dangers of health comorbidities in infectious disease outbreaks was further underlined during COVID. “Strengthening overall health through proactive disease prevention offers a more resilient foundation for responding to future health threats—beyond reliance on vaccines or treatments for yet-unknown pathogens.”
Tony Fauci announced the formation of CREIDs in 2020, awarding 11 grants worth around $17 million, with $82 million in expected funding in succeeding years. NIH did not explain how much of the $82 million slated for CREID had already been spent. Two CREID grantees have been the focus of intense scrutiny since Fauci’s announcement: Peter Daszak of the nonprofit EcoHealth Alliance and Kristian Andersen of Scripps.
Daszak was later discovered to have undisclosed ties to the Wuhan Institute of Virology (WIV), having provided an NIH subaward to WIV researcher Shi Zhengli. At the close of the Biden Administration, the Department of Health and Human Services (HHS) finally debarred EcoHealth Alliance and Peter Daszak from receiving federal funds, in part because “in response to NIH’s multiple safety-related requests” EcoHealth Alliance had not provided WIV records.
Andersen also faced close inspection for his CREID grant. Some months before Fauci gave final sign off on Andersen’s CREID award, Andersen and other researchers published a paper in Nature Medicine titled, “Proximal Origin” that dismissed the possibility of a Wuhan lab accident. Andersen’s paper was widely hailed by scientists as proof, at the time, that discussions of a COVID lab accident was a conspiracy.
Nature Medicine’s editor-in-chief, Joao Monteiro, tweeted that the “Proximal Origin” paper “put conspiracy theories” about the pandemic’s possible lab origin to rest.
Andersen echoed Monteiro’s statement days later, associating “conspiracy theorists” worried about a possible lab accident with people who doubt the Moon landing.
The paper would go on to become one of the most heavily cited scientific papers in 2020. However, emails made public through freedom of information act requests and by congressional investigators later found that the papers’ authors had run it past funders—Collins and Fauci at the NIH, as well as with Jeremy Farrar, then at the Wellcome Trust and now with the World Health Organization.
Congressional Republicans later charged that Fauci had helped orchestrate the paper, while House Democrats pointed the finger at Jeremey Farrar, publishing a report that concluded Farrar helped “organize and facilitate” and “led the drafting process of the paper.”
The group BioSafety Now has demanded Nature Medicine retract the “Proximal Origin” paper, calling it a “a product of scientific misconduct.” Two weeks ago, The DisInformation Chronicle reported that the Justice Department began an initial inquiry into the paper, sending Nature Medicine a list of questions that included, “How do you handle allegations that authors of works in your journals may have misled their readers?” The existence of the Justice Department letter to Nature Medicine had not been previously reported.
Justice Department officials opened the inquiry as they suspect the paper may have been a quid pro quo, published by the authors to dismiss the possibility of a lab accident in exchange for the Fauci CREID grant. Andersen addressed these bribery allegations two years ago during a congressional hearing.
“There is no connection between the grant and the conclusions we reached about the origin of the pandemic,” Andersen wrote in sworn testimony to Congress in July 2023. “We applied for this grant in June 2019, and it was scored and reviewed by independent experts in November 2019.”
The Intercept later reported that Andersen “knew that was false.” NIH records show the Fauci CREID grant to Andersen wasn’t finalized until May 21, 2020, two months after Andersen published “Proximal Origin” in March 2020.
Misleading intelligence agencies
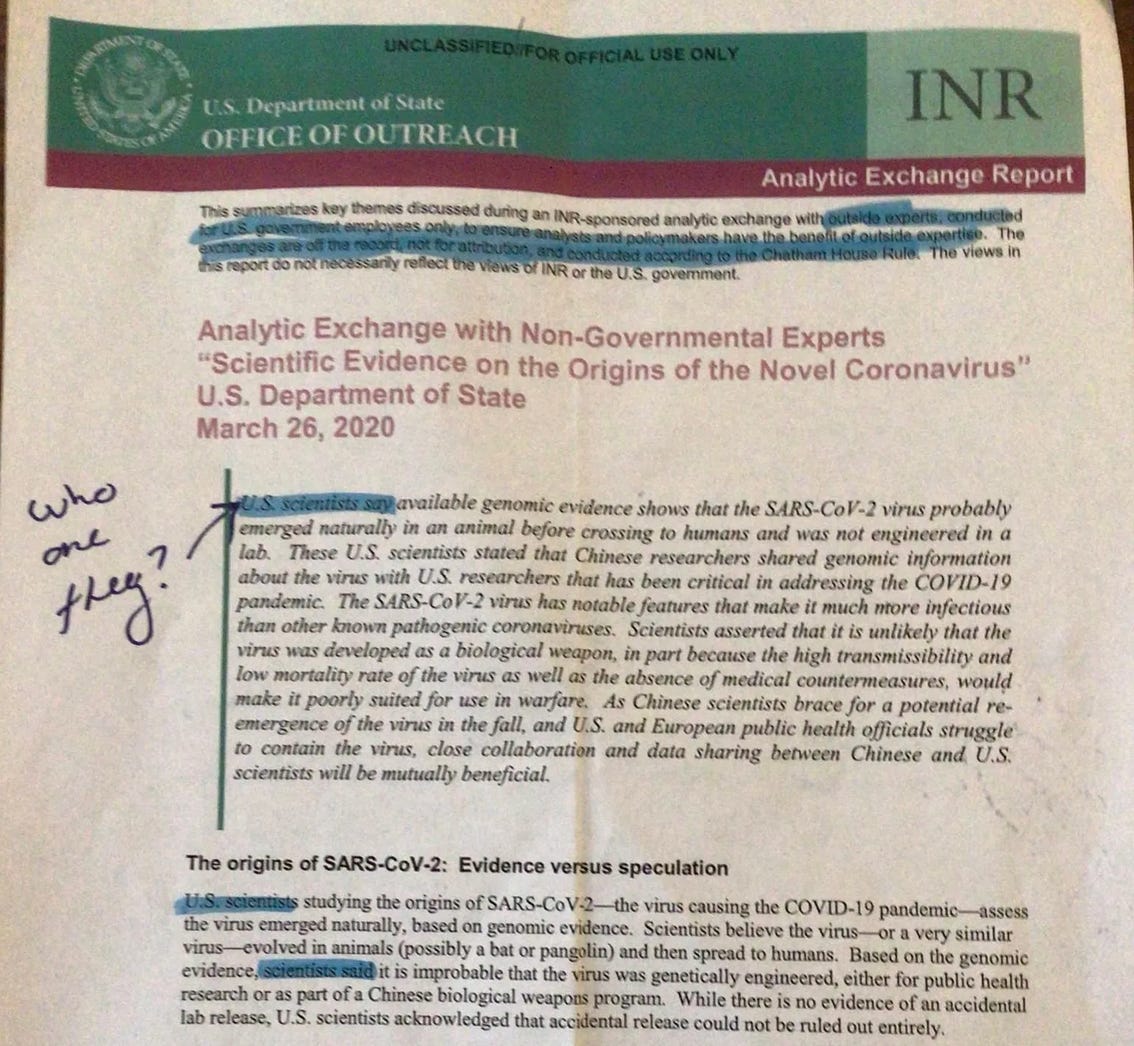
Justice Department officials are also likely to examine Andersen’s possible role in misleading US intelligence agencies. A week after Nature Medicine published “Proximal Origin,” the State Department’s Bureau of Intelligence and Research (INR) published an intelligence report that circulated inside security agencies. First reported by The DisInformation Chronicle, the INR report is marked “UNCLASSIFIED/FOR OFFICIAL USE ONLY.”
The INR report documents a briefing that non-government scientists gave to State Department officials, downplaying the possibility of a Chinese lab accident and citing the “Proximal Origin” paper. The names of the scientists who briefed State remained unknown until a couple years ago, when emails found that one of the scientists was Kristian Andersen, who is apparently a citizen of Denmark, not the US.
“Did we have a foreign national parading into the intel agencies and convincing senior officials to not look into a matter?” said a State Department official who is not cleared to speak to the media. “That’s a counter intelligence matter. We need a professional law enforcement investigation.”
Andersen’s involvement came to light in a late 2020 email sent by State Department official David Feith in which Feith wrote that Andersen had briefed State for their March 2020 INR report. “In fact, I'm told that in a briefing organized by INR earlier this year, [Andersen] said that several features that had initially raised questions in his mind were subsequently put to rest by more detailed analysis,” Feith explained by email. “Notably, it was that subsequent follow-on analysis, referred to by Anderson in the INR discussion….”
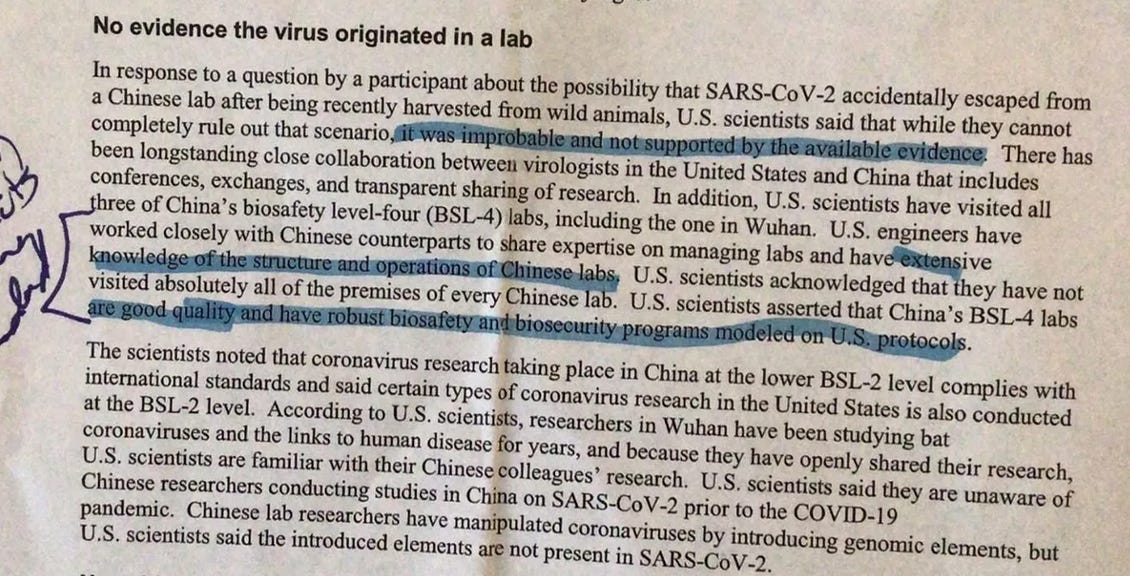
Based on the briefing by Andersen and colleagues, State’s INR report concluded there was no evidence the virus originated in a lab. “U.S. scientists said that while they cannot completely rule out that scenario, it was improbable and not supported by available evidence.”
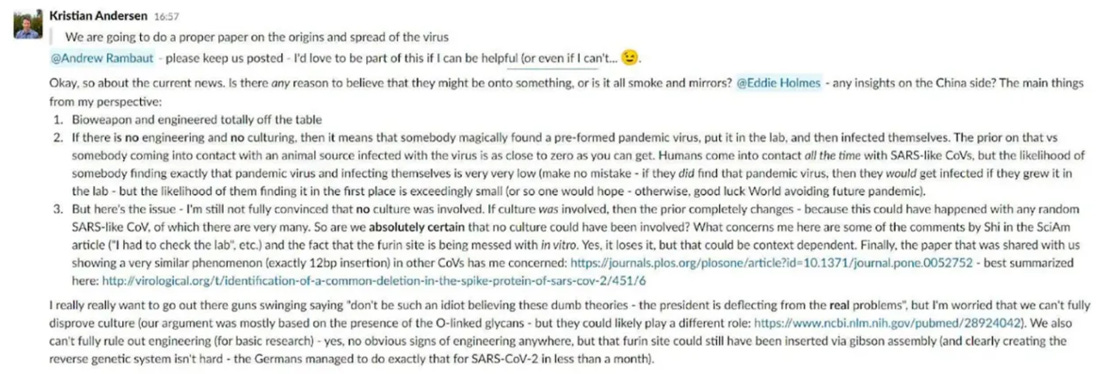
But on April 16, 2020, a month after briefing the State Department, Andersen sent a Slack message to his “Proximal Origin” co-authors. This message contradicts what scientists told the State Department.
“I’m still not fully convinced that no culture was involved,” Andersen wrote his co-authors, a month after briefing State that a lab accident was not supported by evidence. “We also can't fully rule out engineering (for basic research).” Andersen added that a critical part of the virus called the furin cleavage site “still could have been inserted” into the virus.
Researcher Andreas Martin Lisewski with Germany’s Constructor University published a recent study supporting Andersen’s suspicion that a furin cleavage site was inserted into the COVID virus called SARS-CoV-2. After analyzing the sequence, Lisewski concluded the SARS-CoV-2 furin cleavage site came from a laboratory-constructed MERS virus. Although legacy media have ignored these findings, virologist Christian Drosten of Charité University in Berlin presented these conclusions that the SARS-CoV-2 virus was not natural at a World Health Organization meeting last February.
“I don’t see how this not a criminal misleading and counterintelligence matter,” said the State Department official. “This is way beyond the threshold needed for a grand jury.”
During a sworn congressional deposition, Andersen testified that he also briefed the CIA and FBI, although the nature and timing of those discussions is unclear.
As the noose continues to tighten on Andersen, he has been looking to move outside the United States and has apparently found a new home at the University of Oslo. The move would be a precipitous fall in status for Andersen, as Scripps Research Institute has been ranked as one of the most influential scientific programs in the world.
Andersen did not respond to questions and repeated requests for comment sent to his Scripps email.
Finding refuge
“I have heard from several sources that there is an ongoing effort from a group of scientists at the University of Oslo to recruit Andersen, and that this might be finalized in the near future,” said Sigrid Bratlie, a molecular biologist and senior advisor at Norway’s Langsikt Policy Centre.
The campaign to find a position for Andersen at the University of Oslo apparently began last October when professors Anne Spurkland, Rein Aasland, and Nils Christian Stenseth invited Andersen to give a lecture on the Oslo campus. Nelseth has long trumpeted Andersen’s research. In 2021, he published a paper with WIV scientist Shi Zhengli that dismissed the possibility of a Wuhan lab accident, citing Andersen’s “Proximal Origin” paper.
Covering the “facts and the fiction” of the COVID pandemic, Andersen claimed during the October lecture that critiques of his research were mere political attacks that had been spread by conspiracy theorists, naming two Oslo researchers sitting in the audience: Sigrid Bratlie and Gunnveig Grødeland, a professor at the University of Oslo.
Andersen’s Oslo talk was sponsored by the Norwegian Society for Immunology which later released an apology. “Kristian Andersen’s lecture concluded by asserting that, based on his findings, SARS-CoV-2 necessarily originated from an animal at the Wuhan wet market,” the statement reads. “In retrospect, unfortunately, it seems the purpose of his lecture was just as much about stopping the free debate in Norway on this topic.”
Undeterred, Stenseth, Spurkland and Aasland then helped nominate Andersen for membership in the Norwegian Academy of Science and Letters. Two months ago, the Academy accepted Andersen’s nomination.
The exact position being created for Andersen at the University of Oslo is unclear. Stenseth, Spurkland, and Aasland did not respond to questions and repeated requests for comment sent by email. University of Oslo officials also contacted by email did not reply.
Andersen’s arrival in Oslo is likely to be greeted with some trepidation. Last week, Bratlie published a book to positive reviews in Norway titled, “The Wuhan Mystery – the hunt for the origins of the covid pandemic.” Bratlie’s book argues that the pandemic likely started from a lab accident in Wuhan, evidence that was then covered up by international scientists to protect reputations, jobs, and funding. This cover-up, she argues, impedes society’s ability to prepare for future pandemics.
Bratlie said that scientists have legitimate worries about the current climate for research in Trump’s America, but these concerns should be balanced with the need to protect democratic principles and academic integrity.
“I would be absolutely devastated on behalf of Norwegian academia if this recruitment happens,” Bratlie said of the University of Oslo’s bid to bring Andersen to her country. “If Andersen has contributed to a cover-up of the origins of the pandemic, potentially extending to criminal acts, he should be held accountable and not be given amnesty or academic shield in Norway.”
https://disinformationchronicle.substack.com/p/nih-dissolving-pricey-infectious