Shares of MercadoLibre Inc. are heading for their biggest two-day slump since November on concern that Amazon.com Inc.’s latest move in Brazil will ramp up competition in the e-commerce segment.
The stock extended Tuesday’s selloff, dropping as much as 5.8% on Wednesday to as low as $2222.52, its weakest intra-day level since May 7. That followed a 6.6% decline the prior session.
Value wars between Amazon and Walmart to attract cash-strapped consumers are heating up late in the year.Amazon announced on Wednesday morning the launch of a new private-label line called "Amazon Grocery," which spans more than 1,000 products and is largely priced under $5. The timing couldn't be better, as our attention has shifted to a storm brewing in the low-income consumer world.
Amazon Grocery will be a direct competitor to Walmart, Aldi, and other value grocery chains, offering affordable private-label goods amid ongoing value wars (read report). The new line will feature dairy, fresh produce, meat, snacks, and pantry staples priced under $5, an easy hook for low-income consumers. Another selling point: more than 1,000 items can be delivered straight to consumers' doors, saving them the time and hassle of driving to the supermarket and pushing a cart down the aisles.
"The extensive selection includes everything from milk and olive oil to fresh produce, meat and seafood, with most products priced under $5, offering exceptional value to customers," Amazon wrote in a press release.
"With Amazon Grocery, we're simplifying how customers discover and shop our extensive private label food selection while maintaining the quality and value our customers expect and deserve," Jason Buechel, Vice President of Amazon Worldwide Grocery Stores and Chief Executive Officer at Whole Foods Market, wrote in a press release.
Buechel noted, "During a time when consumers are particularly price-conscious, Amazon Grocery delivers more than 1,000 quality grocery items across all categories that don't compromise on quality or taste – from fresh food items to crave-worthy snacks and pantry essentials – all at low, competitive prices that help customers stretch their grocery budgets further."
Amazon has long operated a large online grocery business, selling household basics, paper products, and cleaning supplies. In recent years, it has doubled down on physical retail through Whole Foods Market, Amazon Fresh supermarkets, and convenience stores.
This week, Goldman's consumer sector specialist, Scott Feiler, and financials sector specialist, Christian DeGrasse, both noted that low-income trades are under pressure, pointing to Tricolor and CarMax as potential drivers that have set off alarm bells among investors.
America’s largest anti-hunger program, SNAP, is preparing for a significant update. USDA’s updated SNAP stocking rules aim to replace the “one rice, one bean, one chicken” baseline with a seven-variety standard that reads like a nutrient-density checklist, promising richer choices for the 42 million Americans who rely on the benefit. Yet the question lingers: will the science of dietary diversity survive the politics of convenience-store economics?
SNAP, the Supplemental Nutritional Assistance Program, serves approximately 42 million people in 22 million households, accounting for about 12.5% of our total population. New policy is being directed at the SNAP work requirement [1] and the products available for purchase by SNAP recipients. The USDA has just released updated rules for retailer SNAP eligibility, outlining the required items and their minimum quantities. While ambitious on paper, questions remain about whether these changes will be implemented, let alone how effectively they will be enforced.
The thrust of the rulemaking is to both increase the breadth of nutritional foods available and make it easier to enforce these stocking requirements. There are approximately 250,000 establishments that accept SNAP benefits. The majority, 80% of food stamp redemptions, come from supermarkets and “superstores,” such as Walmart and Target. While convenience stores represent the largest number of outlets, accounting for 44% of the quarter million, they make up only 5% of redemptions. So, the impact of these new rules will be muted at best. Still, how a store qualifies for SNAP participation reveals why variety standards matter.
The Road Paved With Good Intentions
To qualify as a SNAP retailer, a food store must either demonstrate that at least 50% of its sales come from staple foods or show that it carries a required breadth of staple items. Specialty shops, such as butchers or bakeries, usually qualify under the first rule, while most supermarkets and general food stores qualify under the second.
SNAP divides staple foods into four core categories—the building blocks of balanced meals:
Protein: meat, poultry, or fish, whether fresh, frozen, or canned.
Dairy: milk, yogurt, cheese, and related products.
Grains: bread, rice, pasta, cereals, and flours.
Fruits and vegetables: fresh, frozen, or canned produce.
SNAP stocking standards aim to ensure that families can purchase the basic building blocks needed to prepare real meals at home. They emphasize raw staples, grains, flours, beans, peas, and lentils, rather than relying on processed, multi-ingredient products. Under the current regulations, those choices are fairly limited
Only “3 × 4” is required: Stores need only three varieties in each of four staple groups, with perishables required in just two groups. That adds up to as few as 12 items in total.
“Ingredient loophole:USDA’s current “variety” test is ingredient, not product-based, so anything that shares the same main ingredient—no matter the cut, color, flavor, or brand—gets lumped into the same variety bucket. Three cans of pinto beans can satisfy the entire “bean” requirement, or several packs of chicken nuggets can meet the protein quota—leaving little diversity.
Accessory-food loophole: Snack items, such as jerky sticks or protein bars, count toward the quota even though they’re not staples or ingredients, encouraging small stores to stock easy, high-margin snacks instead of fresh or minimally processed staples, thereby squeezing out healthier choices.
Few Perishables: Fresh items are only required in two categories, so retailers often stock shelf-stable produce and dairy but avoid fresh proteins or whole-grain breads. Shoppers often see a limited selection of fresh meats, yogurts, and whole-grain breads—foods that spoil more quickly but are essential for a well-rounded, healthy diet.
In practice, this system often leaves SNAP shoppers in low-income areas, who are primarily served by convenience stores, with a bare-bones pantry instead of genuine choice.
The proposed rules significantly raise the bar—expanding the minimum from 12 items to 28 and tightening definitions to ensure true variety
“3 × 4” becomes “7 × 4”: every SNAP retailer would have to stock seven distinct varieties in each staple group—protein, dairy, grains, and produce. The shelf of white bread, corn flakes, and oatmeal would give way to a variety of options, including rice, quinoa, oats, corn tortillas, pasta, and more.
Removes the ingredient loophole by splitting big buckets into sub-groups. Beans are now categorized by type (dry, canned, or mixed), so a bag of black beans and a can of chickpeas represent different varieties. Protein options expand beyond just chicken.
Closes the accessory-food loophole:Snack bars, most jerky sticks, and cheese/fruit spreads are formally re-labeled “accessory foods,”things we tend to snack on, sweeten with, or use to complement a meal rather than form its foundation, so they no longer count toward staple quotas. A store that previously met its protein target with beef, turkey, and pork jerky must replace them with more traditional staples, such as canned tuna, eggs, or raw nuts, thereby broadening the healthy protein options on the shelf.
More fresh items: Perishables must appear in at least three categories, not just two—so stores must add fresh proteins or grains alongside produce and dairy.
In USDA’s own survey of small retailers, only 52 % stocked enough dairy and 63 % enough protein to meet the future seven-variety standard—evidence that many stores are already thin on these categories today.
SNAP rules are being refined to strike a balance between nutrition and choice. The USDA is proposing updates to SNAP’s variety framework to expand the definition of distinct staple foods in the protein, dairy, and grain categories. The goal is to provide households using SNAP with greater access to diverse, nutritious building blocks for home cooking, while reducing unnecessary complexity for retailers.
Protein has long been the trickiest category for small-format stores to meet. The proposed framework categorizes proteins into seven groupings, now including nuts, legumes, and plant-based proteins—broadening affordable, fiber-rich options.
Dairy’s new categories reflect what most families actually buy, rather than by the mammal (cow, goat, or sheep) producing the dairy product. The focus is on everyday choices, such as milk, yogurt, and cheese, with room for plant-based substitutes.
Grains now focus on raw grains and flour as core staples, recognizing their role as versatile ingredients for cooking and baking. All forms of bread (bagels, tortillas, loaves) count as one variety, as do breakfast cereals and foods.
Fruits and Vegetables are already diverse, but pre-cut produce now counts as staples, while deli-prepared salads do not.
A Nutritional Aside
Nothing is being taken away—people can still buy snack bars, jerky, or fruit spreads with SNAP benefits. The change simply tightens how stores qualify as SNAP retailers. These changes aim to make SNAP stores look less like “just enough” pantries and more like real sources of variety for home cooking.
The proposal doesn’t ban ultra-processed foods (UPFs). What it does is tighten the criteria for which items “count” when retailers prove they stock enough staple foods. Because many UPFs are now classified as accessory foods (so they no longer help a store pass the test), while the quota for minimally processed staples jumps from 12 to 28, shelf space is nudged away from UPFs and toward beans, raw grains, fresh meat, milk, and produce. Shoppers can still buy soda or candy with SNAP, but stores get no regulatory credit for carrying them.
Paving the Road
The idea of stricter retailer requirements is not new. What is little mentioned is that these expanded retailer requirements were part of the 2014 Agricultural Act, or Farm Bill. The USDA spent two years developing regulations to clarify what constitutes a variety. Moments before they were to take effect, now three years since the 2014 enabling legislation, Congress did a “do-over,” barring the USDA from enforcing the new provision and requiring a rewrite to the variety definitions. In 2019, USDA tried again, but its compromise drew criticism from both nutrition advocates and industry. The rules were never finalized, and today’s proposal—nearly a decade later—represents another attempt to balance competing pressures from Congress, advocates, and food retailers.
The long stall comes down to a mix of politics, practicality, and pushback. Congress, worried about the burden on small stores, repeatedly blocked enforcement through budget riders. USDA’s 2019 attempt at compromise alienated advocates by weakening nutrition standards while failing to provide clear regulatory text. At the same time, industry groups pushed for flexibility to avoid stocking requirements they saw as costly or unrealistic. The result has been nearly a decade of gridlock—caught between the Farm Bill’s intent to improve access to healthy staples and the political and logistical realities of regulating diverse food retailers.
If history is any guide, regulation alone won’t turn a corner bodega into a bastion of fresh produce. Without enforcement muscle, incentives for small retailers, and parallel investments in nutrition education, Congress’s decade-old mandate risks another loop through the policy grinder. The new rule is a necessary nudge toward healthier plates. Still, its real power will depend on whether lawmakers fund compliance, watchdogs demand transparency, and communities insist that access to good food is more than a line item. MAHA warriors will once again face the question of whether the words used to woo their votes will become acts and deeds or remain smoke and mirrors.
[1] As Pew Charities reports, “most Americans ages 16 to 59 who aren’t disabled must register with their state SNAP agency or employment office; meet any work, job search, or job training requirements set by their state; accept a suitable job if one is offered to them; and work at least 30 hours a week. Failure to comply with those rules can disqualify people from getting SNAP benefits.”
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.
Last night, Congress failed to pass a seven-week continuing resolution, triggering a federal government shutdown. Senate Democrats refused to support the “clean” CR, insisting on $1.5 trillion in additional spending, including massive subsidies to health insurers, as a condition for keeping the government open.
As I discussed last week, the Democrats’ plan would repeal all the health policy provisions in the One Big Beautiful Bill, including policies that (1) restrict subsidies to U.S. citizens and certain legal immigrants, (2) require work for able-bodied adults on Medicaid, and (3) reduce Medicaid’s money-laundering schemes that result in corporate welfare. Their core demand is to continue a Biden COVID-era policy of $40 billion in additional annual federal payments directly to health insurers selling Obamacare plans above and beyond the original Obamacare subsidies that flow straight to insurers. This is despite overwhelming evidence that much of this spending is lost to fraud and does not translate into any health care received by more than one-third of enrollees.
In today’s newsletter, I discuss two prominent op-eds on why Biden’s COVID credits should expire. I then highlight a new Paragon policy brief that shows there are far more enrollees who do not use any health care compared to the number of people who would supposedly lose coverage when the COVID credits expire. I conclude with an editorial in The Wall Street Journal showing significant attrition in employer-based health coverage over the past few years—attrition driven by the COVID credits.
Ge Bai: Let Covid Credits Expire
In a new Wall Street Journal op-ed, Johns Hopkins professor and Paragon advisor Ge Bai argues that Biden’s COVID credits must expire:
Letting the subsidies go away merely restores the original ObamaCare premium-support structure. That preserves access to subsidies for low-income populations, who already comprise 93% of the 24 million who get health insurance through the ObamaCare exchanges.
As I have written in a recent policy brief, the government would subsidize more than 80 percent of the premium for the average enrollee after the COVID credits expire.
In her op-ed, Ge explains that “since 2021, Congress has been bribing higher-income Americans to purchase expensive ObamaCare plans by hiding the plans’ true price tags using taxpayer dollars.” This is because the COVID credits raised the cap on subsidies that existed at four times the federal poverty level.
Ge documents Obamacare’s problems: soaring premiums, deductibles over $5,000, and one in five medical claims denied. In essence, these plans are so unappealing that massive subsidies are needed to get people to enroll. Those subsidies now exceed $130 billion annually. Policymakers should avoid wasting additional funds by propping up this inefficient structure with ever-larger subsidies. Instead, as Ge suggests, they should begin by asking the more fundamental question: why are Obamacare plans so unaffordable in the first place? Here’s Ge’s answer:
The inflationary provisions of the Affordable Care Act—such as the medical loss ratio, mandated “essential” benefits, community rating and premium subsidies—have inhibited insurers from offering affordable and flexible options. The law’s regulatory burdens on providers have also fueled consolidation and driven up service prices.
More from Ge, including a mention of fraud, which I discuss below:
By luring people to these expensive plans and making them dependent on subsidies, lawmakers not only wasted taxpayer dollars and invited fraud but also effectively killed the market for affordable alternatives. Continuing this scheme would be fiscally reckless and irresponsible to consumers. Covid-era subsidies should be allowed to die a natural death.
Ge then discusses how the COVID credits make health coverage worse for Americans:
By masking the true price of ObamaCare plans, Covid-era premium subsidies have distorted insurance markets and trapped people in plans they don’t want. As Americans start to understand how expensive these plans really are, they will begin demanding genuine insurance that covers only major events at affordable premiums. Innovative options—such as direct primary and specialty care, association plans, health-share ministries, and crowd-sharing arrangements—will emerge organically.
Burlison: Let Covid Credits Expire
Congressman Eric Burlison of Missouri had a Washington Examiner op-ed on why the COVID credits should expire. According to Rep. Burlison:
42% of Obamacare enrollees are on fully subsidized plans as of 2024. Another 28% pay a premium of $50 or less. When Biden’s subsidies expire, the average enrollee (someone earning 200 percent of the federal poverty level) will only have to pay $32 a week for a plan — about the cost of a median DoorDash order. Someone earning 100% of the poverty level would only have to pay $3.45 — the cost for a cup of coffee.
Even without Biden’s COVID subsidies, taxpayers will still cover 80% of the typical enrollee’s premium —up from 68% in 2014. That’s because Obamacare subsidies cap what enrollees pay, fully insulating them from rising healthcare costs and shifting costs directly onto taxpayers.
If Republicans cave to the Left’s demands, it will be entirely clear that generous taxpayer-funded pandemic healthcare subsidies will be here to stay; almost four million Americans will lose their employer coverage, crowded out by artificially low government-backed premiums.
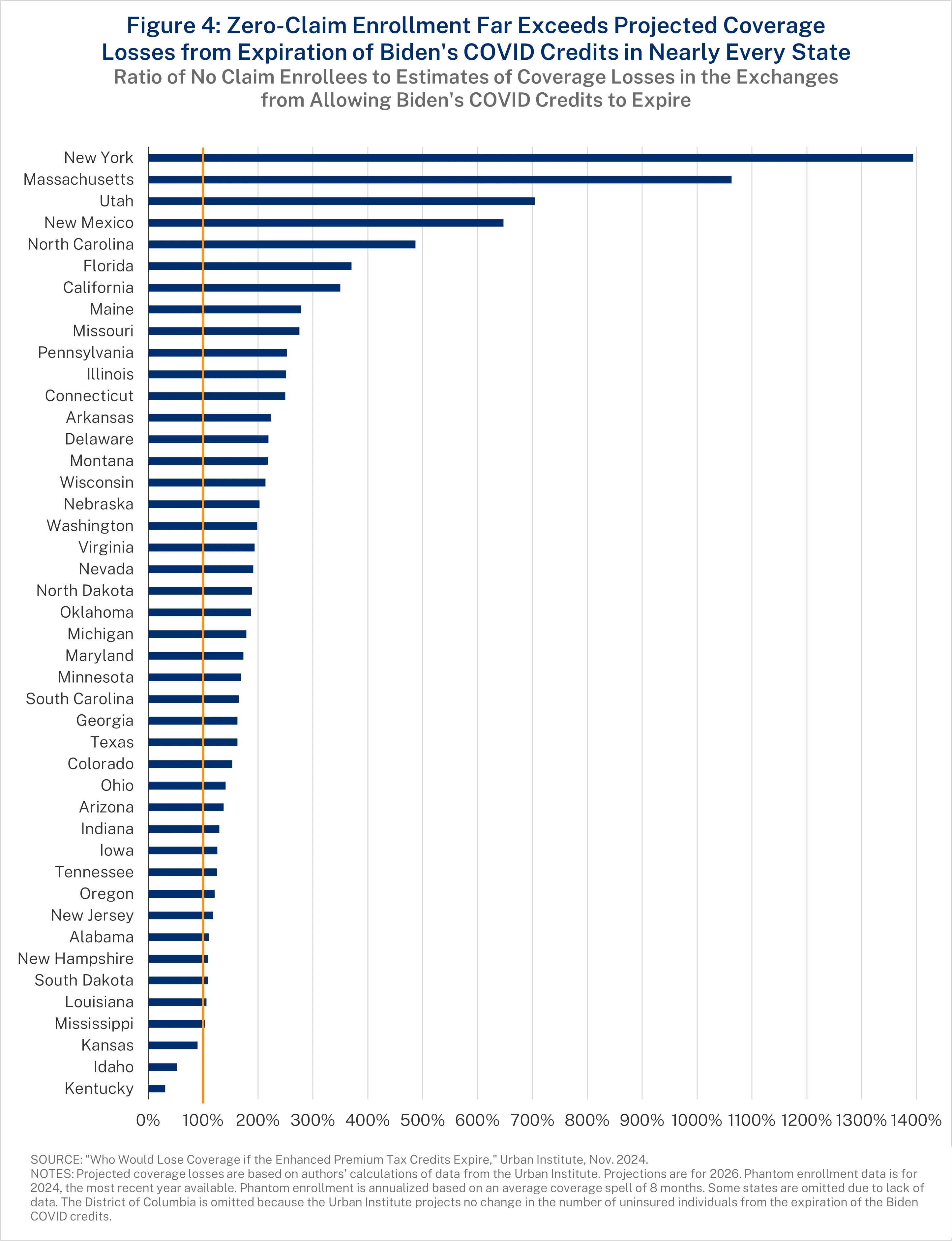
Zero-Claim Obamacare Enrollees by State
As a result of Biden’s COVID credits, there was a surge in enrollees with coverage who received no care. In fact, two in five enrollees in fully subsidized Obamacare plans did not use their coverage at all in 2024—not for a single doctor visit, test, or prescription.
In a new policy brief from Paragon, Niklas Kleinworth, John R. Graham, and Liam Sigaud uncover how these zero-claim enrollees cannot be explained by a surge of young, healthy enrollees without health care needs. The increase in zero-claim enrollees between 2021 and 2024 is more than double the increase in enrollees under 35 years of age. Rather, many of these enrollees are phantoms—people unaware of their coverage or enrolled in other plans.
Paragon estimates that more than 6.4 million individuals were fraudulently enrolled in exchange plans during 2025. These are people who claimed incomes between 100 and 150 percent of the federal poverty level to qualify for a fully subsidized 94% actuarial value plan, even though they did not earn that income. They found a very strong positive correlation between zero-claim and fraudulent enrollees by state (a correlation coefficient of 0.67). Of the top 20 states with zero-claim enrollees, 15 of them also ranked in the top 20 for fraudulent enrollment.
The large number of zero-claim enrollees severely undercuts the argument that permitting the COVID credits to expire will harm Americans’ health. Prior work from Paragon highlighted how health coverage does not translate to improved health, but those who are unaware of even having this coverage in the first place certainly would not face any negative health effect from losing coverage.
The new brief compares state projections of the increase in the uninsured if the COVID credits expire with zero claim enrollees. In all but three states, there are more zero claim enrollees (on an annualized basis) than enrollees who would lose coverage. As the figure below shows, zero-claim enrollees outnumber projected coverage losses by more than two-to-one in 17 states.
Though not all disenrollments will involve phantom enrollees, most coverage losses will likely come from people who valued coverage so little they enrolled only because it was free, or from individuals who were unknowingly enrolled by fraudsters, unaware they had ACA coverage entirely.
Covid Credits Hit Employer Coverage
In a September 29 editorial, The Wall Street Journal reviews data from the Bureau of Labor Statistics (BLS) and highlights a massive drop in the percentage of employees covered by their employers’ health insurance plan. According to The Journal’s analysis, “the share of workers with access to medical benefits increased to 74% this year from 71% in 2019.”
At the same time, “the share of workers who participate in employer medical plans…has fallen to 65% from 73%.” The drop is steepest among lower-income workers: “part-time workers (to 44% from 56%) and employees whose wages are in the bottom 25% (49% from 61%) and 10% (34% from 57%).”
The editorial asks why—and reaches the right conclusion. “Perhaps because they can now get ObamaCare plans at no cost.”
The COVID credits were massive new subsidies—but only for people who do not have employer-based health coverage. As a result, there is less incentive for workers to enroll in employer coverage or seek employers who offer coverage. The editorial concludes: “The BLS report shows that many workers could get employer coverage if the enhanced subsidies lapse… Don’t believe the Democrats’ ObamaCare scare.”
Brian Blase, Ph.D., is the President of Paragon Health Institute.
The manufacturer of Tylenol was keeping tabs on research into the drug and neurodevelopmental issues such as autism, and concluded in 2018 that evidence of a link between them was becoming significant, according to newly disclosed documents.
In a Feb. 8, 2018, email obtained by The Epoch Times, Rachel Weinstein, director of epidemiology at Johnson & Johnson subsidiary Janssen, wrote, “The weight of evidence is starting to feel heavy to me.”
Weinstein was emailing Jesse Berlin, Johnson & Johnson’s global head of epidemiology, about a review that concluded that nine studies suggested that use of acetaminophen—the active ingredient in Tylenol—by pregnant women was linked to autism and other neurodevelopmental issues in the women’s children.
Weinstein said that Janssen had been discussing with a neurologist about how acetaminophen could be beneficial.
“But now we’ve added the studies in prenatal exposure and neurodev [sic] outcome,” she said.
Berlin wrote that he read the review and that “there appears to be some specificity of the association.” While he took issue with how some papers did not analyze other drugs, “at least one study looked separately at specific indications and the association didn’t go away,” he said.
Johnson & Johnson was the maker of Tylenol for years. In 2023, a newly created company called Kenvue took over the Tylenol brand and other consumer brands.
“These documents show we were doing exactly the right thing,” a spokesperson for Kenvue told The Epoch Times in an email. “We have continuously evaluated the science, and there is no credible evidence that taking acetaminophen causes autism.”
‘Difficult Options’
Dr. Jørn Olsen of Aarhus University in Denmark and other researchers in 2014 released an observational study that determined maternal acetaminophen use during pregnancy was linked to a higher risk of attention-deficit/hyperactivity disorder-like behavioral problems or hyperkinetic disorders in their children.
Weinstein, in an email, told Olsen that the study had strengths but wondered whether the researchers had tried assessing any association between other drugs pregnant women take, such as aspirin, and the disorders. Olsen, in a brief reply, said the researchers planned to look at those drugs in future studies.
Weinstein forwarded the email to the company’s consumer medical safety division.
“Recall that we have ruled out the possibility of conducting a database study of our own because other existing databases would be underpowered to detect the same effect that the Danish study found, due to the lack of a large enough database,” she wrote in her email.
She asked whether the question for the company was whether there was a willingness to support Olsen “up to a reasonable amount with the provision that the investigator has final say on publication but the sponsor can review and comment on the manuscript prior to publication.”
Weinstein told Berlin that there were several options, including funding Olsen. They could also try to replicate Olsen’s study, conducted in Denmark, with Norwegian data on prescriptions and diagnoses, and by including other drugs.
“The outcome of such a study is unknown. We could end up confirming the Danish findings, for example,” she said.
She later drafted a note to Olsen that initially said Johnson & Johnson would be happy to work with him on additional research. Berlin in response proposed revisions. But Weinstein then told Berlin she was having second thoughts on engaging Olsen.
“Do we really need to stick our neck out and make this offer? Would we be surprised if the new analyses confirmed or did not confirm the existing studies?” she asked.
Berlin responded: “I’m trying to think through what we would do based on what we learn. I don’t have a huge problem abandoning this, if that’s where we end up after talking.”
Weinstein, who is now retired, could not be reached for comment. Berlin, now a professor at Rutgers University, did not respond to a request for comment.
Internal slides from around the time of the emails, obtained by The Epoch Times, stated that the company declined to pursue a collaboration with Danish researchers in part because executives were unsure about “the value to pregnant consumers,” who might be presented with “difficult options” such as “don’t use anything if you have a fever.”
Lawyer: ‘Irresponsible’
The emails came to light in lawsuits brought by women who say they should have been warned by Johnson & Johnson and retailers about the risks of neurodevelopmental problems associated with acetaminophen products.
The women have pointed to papers such as a 2020 prospective study in Canada that found an increased risk of ADHD among children born to women who used acetaminophen while pregnant.
“Drugmakers have a legal and ethical obligation to continually investigate the safety of their products. Yet despite recognizing the heavy weight of the scientific evidence years ago, Kenvue scientists made a deliberate decision not to ’stick our necks’ out to commission further research,” Ashley Keller, senior partner at law firm Keller Postman, which is representing the women in multiple cases, told The Epoch Times via email.
“The reason for that irresponsible choice is obvious. The company didn’t study the question for fear they would not like the answer. But pregnant moms deserve answers, and protecting a multi-billion dollar drug franchise is no excuse for ostrich-like corporate misbehavior.”
The emails were first reported by the Daily Caller and drewtheattention of the White House and the Department of Health and Human Services.
Government officials recently warned the public that Tylenol use during pregnancy may be associated with autism in children born to the mothers.
‘We Have Been Looking at It’
Weinstein said in a 2023 deposition that it would be unethical to run a randomized, controlled trial seeking to figure out whether there was a link between in utero acetaminophen exposure and neurodevelopmental problems. It would be good to do “more tightly controlled” observational studies, or research utilizing sources such as medical claims databases, she said.
Weinstein also said that Johnson & Johnson had been tracking literature on the topic for nearly a decade, including epidemiological, safety, and preclinical studies.
She said that the company has “essentially done a systematic review,” or an analysis of strong studies on the matter.
She said the company would be publishing the review but did not know when.
Internal slides from 2018, obtained by The Epoch Times, described the results of a company analysis of 16 studies regarding prenatal exposure to acetaminophen and neurodevelopmental disorders.
The slides stated that individual observational studies “show a somewhat consistent association of increased occurrence of neurodevelopmental outcomes with prenatal exposure,” with strengths including some studies being prospective. Limitations included researchers measuring children at different ages, such as 18 months and seven years.
A 2022 internal Kenvue slide deck stated that 12 studies featuring clinically diagnosed endpoints were analyzed. The studies were “too limited in methodological or analytical design to draw conclusions regarding a causal relationship between prenatal acetaminophen use and adverse neurodevelopmental outcomes in children,” and therefore, if acetaminophen is used as directed, it is safe to use during pregnancy, the slide deck stated.
A review coauthored by Kenvue scientists and funded by Kenvue was published by Critical Reviews in Toxicology in February.
The authors of the review said that they reviewed preclinical studies and determined that the data “demonstrates no consistent evidence of adverse effects following developmental exposure to acetaminophen at therapeutic and/or non-systemically toxic doses on the structure and function of the nervous system, including neuroanatomical, neurotransmission, and behavioral endpoints.”
Labeling Change
Other documents labeled the effort to study the matter Project Cocoon, stated that Weinstein was involved, and listed as the mission of the project “to protect acetaminophen.”
One slide stated, “Courage: We don’t need a label change.”
The label of Tylenol has long stated, “If pregnant or breastfeeding, ask a health professional before use.”
In 2017, one document showed that the company changed its internal label to add, “This product should not be used during pregnancy or lactation unless the potential benefit of treatment to the mother outweighs the possible risks to the developing fetus/nursing infant.”
When asked in a 2023 deposition about whether the change means doctors could give patients guidance on potential risks of developmental outcomes, Leslie Shur, Johnson & Johnson’s director of pharmacovigilance, replied, “and the risk of, in the case of fever ... of not treating.”
The U.S. Food and Drug Administration said on Sept. 22 that it has started the process to change the label for Tylenol and other acetaminophen-containing products “to reflect evidence suggesting that the use of acetaminophen by pregnant women may be associated with an increased risk of neurological conditions such as autism and ADHD in children.”
Regulators said a causal relationship has not been established and noted that acetaminophen is the only over-the-counter drug available to treat fevers in pregnancy.
The FDA in 2014 had decided to take no regulatory action, following advice from reviewers. In 2016, FDA reviewers said, “With growing evidence for adverse neurodevelopmental outcomes being associated with in utero [acetaminophen] exposure, even in the absence of proof of a causal relationship, it would be appropriate for FDA to bring this issue to the attention of consumers and health care providers through one of the communication avenues available to the agency.”
Reviewers in 2019 said data indicated that prenatal acetaminophen exposure “is not necessary completely benign for the fetus” and “it would be desirable for the agency to communicate this message to healthcare providers and pregnant women, considering that acetaminophen is so commonly used by women during their pregnancies, and that many perceive acetaminophen to be risk-free.”
Court Cases
U.S. District Judge Denise Cote dismissed the federal multidistrict litigation over acetaminophen in 2024, after finding that experts offered by the plaintiffs misrepresented the results of studies.
The case was appealed and is set for oral argument before an appeals court on Nov. 17, after being delayed from a date in early October.
Keller and other attorneys in a recent filing alerted the court to the government’s move to update Tylenol’s label. The filing noted that government officials quoted one of the plaintiffs’ witnesses, Dr. Andrea Baccarelli, dean of the faculty at the Harvard TH Chan School of Public Health, who said that, in his expert opinion, “there is a causal relationship” between prenatal acetaminophen exposure and neurodevelopmental disorders.
“Expert opinion that is sound enough to persuade every Senate-confirmed federal scientist easily clears Rule 702(d)’s bar,” or the rule governing expert witnesses in litigation, they wrote. Attorneys for Kenvue told the court that statements from the government and Baccarelli “confirm that the existing evidence does not support a causal relationship.”
In California, a state judge in May turned away a similar case, concluding that evidence on the link between prenatal acetaminophen exposure and autism is “profoundly uncertain and conflicting.”
The judge also wrote that slides and other internal documents showed “candid internal discussion,” which she described as “positive corporate behavior.”
As the government shuts down, Democrats are facing criticism over their alleged support for health care subsidies to noncitizens residing in the United States.
The Democrat continuing resolution bill would revoke Subtitle B in Title VII of the One Big Beautiful Act, effectively restoring accessibility to some government benefits to certain noncitizens, including inadmissible aliens granted parole for at least one year.
That subsection of the act had limited government health care benefits to American citizens, “(1) LPRs [lawful permanent residents]; (2) certain Cuban and Haitian immigrants; and (3) COFA [Compact of Free Association] migrants lawfully residing in the U.S.”
The subtitle also restricts Medicare eligibility and premium tax credits by restricting them to the four groups defined above.
The expansion of benefits to potentially reward illegal aliens with taxpayer dollars stands in stark contrast to points Senate Minority Leader Chuck Schumer, D-N.Y., made decades ago in Congress.
“All over where we go, people say, ‘Well, can’t you stop illegal immigrants or others from coming here?’ And the No. 1 answer we give our constituents is, when they come here, they can get jobs, get benefits against the law because of fraud,” Schumer, then a New York congressman, said in a speech on the House floor in 1996.
A clip from that speech was reposted by Vice President JD Vance on X on Tuesday, who wrote, “Chuck Schumer once recognized that it was disastrous to give illegal aliens rewards for breaking the law. Now he wants to shut down the government unless we … reward illegal aliens for breaking the law.”
In 2019, during a Democrat presidential primary debate, each candidateraised their handsin support of giving illegal aliens health coverage. That group of candidatesincludedformer President Joe Biden; former Transportation Secretary Pete Buttigeig; Andrew Yang; then-Colorado Gov. John Hickenlooper (who now represents Colorado in the Senate); Marianne Williamson; Sen.Bernie Sanders, I-Vt.; then-Sen. Kamala Harris, D-Calif.; Sen. Kirsten Gillibrand, D-N.Y.; Sen. Michael Bennet, D-Colo.; and Rep. Eric Swalwell, D-Calif.
In June, several Democrat senators, including Sanders and Sen. Elizabeth Warren, D-Mass., reintroduced legislation in the upper chamber to allow illegal aliens to participate in Obamacare marketplaces and to create the possibility for states to expand Medicaid and the Children’s Health Insurance Program to aliens not in the country lawfully.
“Health care is a human right—regardless of a person’s immigration status. With this critical legislation, we remove cruel, unnecessary barriers preventing immigrants from receiving the care they need to survive and thrive. By providing access to quality care and treatment, we strengthen our communities and bolster our nation’s public health,” Sen. Richard Blumenthal, D-Conn., stated in a press release about the bill.
Indivior has agreed to halt all marketing of its opioid overdose drug Opvee in New York after being rapped by the state attorney general for mispromoting it to health officials.
New York AG Letitia James announced a settlement with Indivior, which has been accused of marketing Opvee (nalmefene) to public officials throughout the state as an interchangeable alternative to Emergent BioSolution's Narcan (naloxone) even though it is not authorised for use without a prescription.
Opvee was approved by the FDA in 2023 as a prescription-only medicine, but has found it hard to compete in the US market against Narcan, which was approved in the same year as an over-the-counter (OTC) product that can be bought from a regular pharmacy without a doctor's scrip.
The product has not met Indivior's expectations, with the UK company – which has just announced a plan to switch domiciles to the US after listing on the Nasdaq and delisting from the LSE earlier this year – forecasting in July that full-year sales will reach just $10 to $15 million in 2025.
Aside from the lack of a legitimate OTC business, Opvee has also been hampered by what James described as advice from health officials across the US that Opvee is comparable in efficacy to Narcan but is associated with "significantly more severe side effects."
The settlement with New York includes a commitment to repay any taxpayer dollars Indivior received for Opvee, recall all the sold doses, stop making false statements about the drug, and reform its marketing and training practices. According to James, the company said it would stop all promotion of the drug shortly after the settlement was signed.
Indivior acquired Opvee when it bought Opiant for $145 million in 2023, and has predicted annual sales of $150 million to $250 million for the product. It was viewed as an important product for the company as it faced the loss of patent protection for Suboxone, an oral film formulation of buprenorphine/naloxone that approached $1 billion in sales at its peak before succumbing to generic competition.
Since then, Indivior has managed to grow sales of its new product Sublocade (buprenorphine extended release), which is expected to bring in up to $785 million in sales this year, although the company has been forced to cut staff and simplify its operating structure as it tries to rebuild growth and its presence in the long-acting injectables market.
It's not the first time that Indivior has run into trouble over marketing practices, however, and last year it was forced to pay $86 million to settle claims brought by 16 US states, including New York, that it contributed to the opioid epidemic in the US.
"Indivior cannot rewrite its history and exploit this drug crisis for profit," said James. "After playing a role in fuelling the opioid epidemic, the company tried to position itself as part of the solution while misleading public officials and the communities they serve about which overdose treatments are safe, legal, and effective."