The coronavirus disease
2019 (COVID-19) pandemic caused by severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) has already surpassed the combined mortality
inflicted by the severe acute respiratory syndrome (SARS) epidemic of
2002 and 2003 and the Middle East respiratory syndrome (MERS) epidemic
of 2013. The pandemic is spreading at an exponential rate, with millions
of people across the globe at risk of contracting SARS-CoV-2. Initial
reports suggest that hypertension, diabetes, and cardiovascular diseases
were the most frequent comorbidities in affected patients, and case
fatality rates tended to be high in these individuals. In the largest
Chinese study to date,1
which included 44 672 confirmed cases, preexisting comorbidities that
had high mortality rates included cardiovascular disease (10.5%),
diabetes (7.3%), and hypertension (6.0%). Patients with such
comorbidities are commonly treated with renin angiotensin system
blockers, such as angiotensin-converting enzyme inhibitors (ACEIs) or
angiotensin receptor blockers (ARBs). However, the use of ACEIs/ARBs in
patients with COVID-19 or at risk of COVID-19 infection is currently a
subject of intense debate. Below, we outline the mechanisms by which
ACEIs/ARBs may be of benefit in those with COVID-19, what the current
recommendations are for their use in infected patients, and suggested
areas for further research.
SARS-CoV-2 uses the angiotensin-converting enzyme (ACE) 2
receptor for entry into target cells. ACE2 is predominantly expressed
by epithelial cells of the lung, intestine, kidney, heart, and blood
vessels. Both ACE and ACE2 belong to the ACE family of dipeptidyl
carboxydipeptidases and exert distinct physiological functions. ACE
cleaves angiotensin I to angiotensin II, which in turn binds and
activates angiotensin II receptor type 1. This activation leads to
vasoconstrictive, proinflammatory, and pro-oxidative effects. In
contrast, ACE2 also degrades angiotensin II to angiotensin 1-7 and
angiotensin I to angiotensin 1-9. When angiotensin 1-9 binds to the Mas
receptor, it leads to anti-inflammatory, antioxidative, and vasodilatory
effects. It is important to note that 2 forms of ACE2 exists: a
structural transmembrane protein with extracellular domain that serves
as a receptor for spike protein of SARS-CoV-2 and a soluble form that
represents the circulating ACE2. Understanding the relationship between
SARS-CoV-2 and membranous and soluble ACE2 may help us better understand
the adaptive or maladaptive processes operative in COVID-19 infection.
Animal (mice) studies have shown that expression of ACE2 is substantially increased in patients treated with ACEIs/ARBs.2,3
Similar to these observations, higher urinary ACE2 levels were seen in
patients with hypertension treated with the ARB olmesartan. In another
study,4
circulating ACE2 levels were increased in patients with diabetes
treated with ACEIs. Based on these observations, some experts have
speculated that use of ACEIs/ARBs leading to increased expression of
ACE2 could potentially facilitate infection with COVID-19.
A recent study by Liu et al5
showed that serum angiotensin II levels in patients with COVID-19
pneumonia was significantly higher compared with healthy individuals and
were linearly associated with viral load and lung injury. Based on
this, it can be postulated that SARS-CoV-2 binding to ACE2 may attenuate
residual ACE2 activity, skewing the ACE/ACE2 balance to a state of
heightened angiotensin II activity leading to pulmonary vasoconstriction
and inflammatory and oxidative organ damage, which increases the risk
for acute lung injury (ALI). Conceivably, renin angiotensin system
modulation, either by ACEIs/ARBs or recombinant ACE2, leading to
increased expression of ACE2 may help mitigate some of these deleterious
effects of angiotensin II. It is also postulated that increased levels
of soluble form of ACE2 may act as a competitive interceptor of
SARS-CoV-2 and slow virus entry into the cells and protect from lung
injury.6
Presently, to our knowledge, there are no clinical data on the utility
of initiating ACEI/ARB therapy in treating patients with COVID-19. There
is some evidence that ACEIs/ARBs may be beneficial in patients with ALI
or acute respiratory distress syndrome (ARDS). In a meta-analysis of 37
studies,7
ACEIs and ARBs were associated with reduced risk of pneumonia and
pneumonia-related mortality compared with control treatment. In a small
double-blind, placebo-controlled randomized clinical trial of 61
patients,8
those randomized to receive enalaprilat (up to 10 mg intravenously over
24 hours following a regimen based on blood pressure) had numerically
higher ventilator-free days (12.3 vs 8.7 days; P = .18) and days alive outside the intensive care unit (8.9 vs 4.9 days; P = .09)
compared with those randomized to placebo. The trial did not complete
its intended sample size owing to slow enrollment. In a retrospective
cohort study from Korea with 132 patients with ARDS,9
patients taking ACEIs/ARBs showed better survival compared with
controls, albeit several confounding factors could have influenced the
results. In a subgroup of patients with severe COVID-19,
hyperinflammation and cytokine storm syndrome led to acute respiratory
failure from ARDS. What drives such intense hyperinflammation is not yet
known; however, through upregulation of ACE2, ACEIs/ARBs can exert
anti-inflammatory and antioxidative effects, which may be beneficial in
preventing ALI and ARDS.10
Based on the pathophysiology of SARS-CoV-2 infection and pleiotropic
effects of ACEIs/ARBs, these agents may have a potential role in the
management of select patients with severe COVID-19.
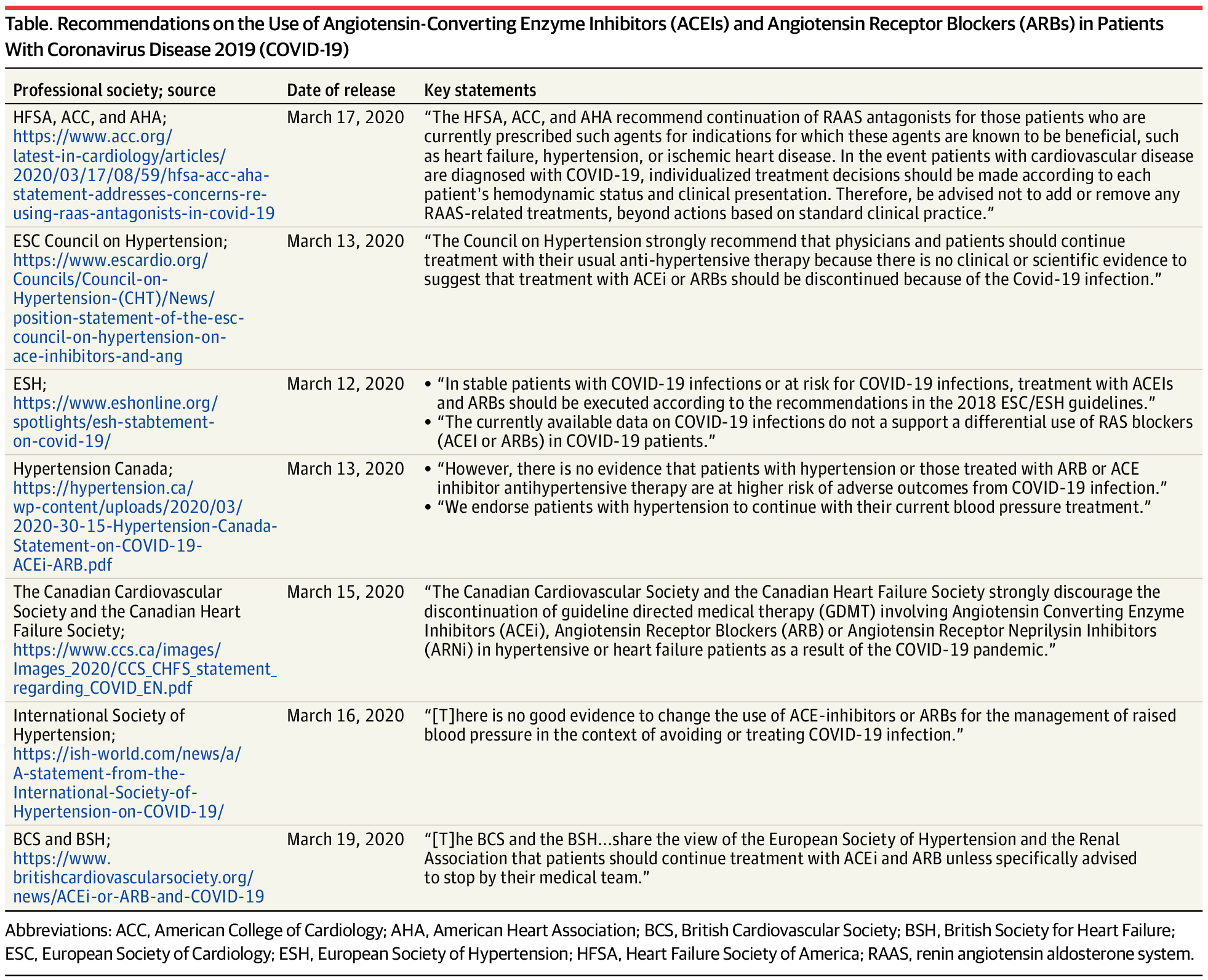
Several professional societies have put forward their
guidance regarding the use of ACEIs/ARBs in patients with COVID-19. In
summary, all guidelines recommend continuing ACEIs/ARBs in patients with
COVID-19 unless clinically indicated (Table).
Furthermore, they do not suggest initiation of ACEIs/ARBs in those
without another clinical indication (eg, hypertension, heart failure,
diabetes), given the lack of strong evidence showing benefit of these
medications in COVID-19. We agree with these recommendations, given the
current state of evidence. However, the biological plausibility of
salutary effects of ACEIs/ARBs in those with COVID-19 is intriguing. A
multicenter, double-blind, placebo-controlled phase 2 randomized
clinical trial of starting losartan in patients with COVID-19 in
outpatient settings (ClinicalTrials.gov identifier: NCT04311177) and in in-patient settings (ClinicalTrials.gov identifier: NCT04312009)
is currently being planned. Accordingly, further epidemiological
studies and prospective trials are urgently needed to investigate if use
of ACEIs/ARBs can reduce the incidence or mortality associated with
COVID-19–associated ALI or ARDS, both in patients with and without
additional clinical indications for ACEIs/ARBs.
Table. Recommendations on the Use of
Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin
Receptor Blockers (ARBs) in Patients With Coronavirus Disease 2019
(COVID-19)
Article Information
Published Online: April 3, 2020. doi:10.1001/jamacardio.2020.1282
Conflict of Interest Disclosures:
Dr Maddox has received grants from the National Center for Advancing
Translational Sciences, consulting fees from Creative Educational
Concepts and Atheneum Partners, and honoraria and personal fees from the
University of Utah, NewYork-Presbyterian, Westchester Medical Center,
Sentara Heart Hospital, Henry Ford Health System, and University of
California, San Diego; is the Executive Director of the Healthcare
Innovation Lab at BJC HealthCare/Washington University School of
Medicine in St Louis; advises Myia Labs through his institution, which
receives equity compensation; and is the director of JF Maddox
Foundation. Dr Messerli has received personal fees from Menarini,
Medtronic, and Pfizer. No other disclosures were reported.
https://jamanetwork.com/journals/jamacardiology/fullarticle/2764299