A proposal to change the way the federal government pays some states
under the Medicaid program is causing headaches for healthcare groups
and Medicaid directors, even though it hasn’t actually been enacted yet.
The Medicaid Fiscal Accountability Rule (MFAR), released last November
by the Centers for Medicare & Medicaid Services (CMS), would reduce
the amount of money that CMS gives to states as part of their Medicaid
matching funds when the money is generated through various supplemental
means.
“CMS is aware of numerous schemes states have used that are not consistent with federal statute,” the agency said in a press release.
“Some examples include states that generate extra payments for private
nursing facilities that enter into arrangements with local governments
to bypass tax and donation rules, and the use of a loophole to tax
managed care entities 25 times higher for Medicaid business than for
similar commercial business. States can then use that tax revenue to
generate additional payments, with no commensurate increase in state
spending.”
“Many of the vulnerabilities in Medicaid financing arise from
high-risk financing mechanisms that states have used, or sought to use,
to finance the state portion of Medicaid payments,” the release
continued. “These include intergovernmental fund transfers … provider
taxes, and provider donations that provide additional payments to
institutions with no clear link to improving care for patients. The
proposed rule would provide clearer guidance on the law to states and
other stakeholders, help close regulatory loopholes, and improve
reporting to help CMS ensure that states fund their share of payments to
providers through only permissible sources and with methodologies that
comport with statutory requirements.”
Concerns About Payment Cuts
But critics of the proposed rule say that it would mean a cut in federal Medicaid funds that states have come to rely on.
“Through the proposed rule, CMS outlines a number of changes that
reduce states’ ability to generate state share to finance their Medicaid
program,” wrote Margaret Murray, CEO of the Association for Community
Affiliated Plans (ACAP), which represents safety-net health plans, in a Jan. 31 letter
to CMS. “ACAP is concerned that these changes will limit state
flexibility to generate state share, which will have downstream effects
on state Medicaid funding and ultimately reduce access to critical
services for Medicaid beneficiaries.”
States could lose $37 billion to $49 billion annually under the rule, according to a report from Manatt Health and the American Hospital Association.
The agency gave two justifications for developing the rule, explained
Edwin Park, JD, a research professor at Georgetown University’s Center
for Children and Families, in a phone interview. First, “they document
problems where states have violated existing federal requirements, and
they say, ‘We don’t have enough data on what states and providers are
doing,'” he said.
Two Justifications
In the rule’s preamble, CMS gives some examples of states violating
current rules; however, “What’s not clear from that preamble is that
they found these problematic arrangements under existing rules and …
there are existing enforcement arrangements to prevent them. The rule
changes really have nothing to do with those examples; they’re using the
examples to make a very broad change to rules that have been in place
for almost three decades.”
The other justification for the rule is a need for more transparency
about these miscellaneous financing mechanisms like intergovernmental
transfers and provider taxes; the rule would require more reporting from
states. “There is general acceptance that there should be more known
about these arrangements,” Park agreed. “But the reporting is only one
small portion of the proposed rule, and the large majority of the rule
is about prohibiting existing arrangements.”
As the COVID-19 pandemic advanced on the U.S., healthcare groups were
encouraged that several of the stimulus bills passed by Congress
addressed states’ healthcare funding needs. For example, the Families
First Coronavirus Response Act, which President Trump signed into law on
March 18, provides enhanced Medicaid matching funds to states to help
them through the pandemic. But if there is less state money on the table
because the federal government has disallowed some of these financing
mechanisms, “you draw down less federal dollars, including the enhanced
matching rate that Family First provides,” said Park.
“If you add on the COVID 19 crisis, as revenues fall and program
costs rise, states are going to be cash-strapped,” he continued. That
will mean Medicaid cuts, “and one of the obvious places states would go
would be provider rates, as was done in previous economic downturns.”
Push for Delay or Rescission
During the debate over the most recent stimulus bill, Democratic
legislators presented alternative legislation that included a provision
that would delay the implementation of MFAR, but it didn’t get included
in the final bill. The only possible good news on the MFAR front,
according to Matt Salo, executive director of the National Association
of Medicaid Directors, “is that CMS is telling us that all non-COVID-19
work is on the back burner. That’s good, but what does that really mean?
Back burner until 6 weeks from now? Eighteen months from now? We of
course don’t know.”
“There are assurances that when they do get back around to MFAR, two
things will have happened — a lot of people commented, including us, and
it sounds like they’re going to take those comments into consideration,
which is good, and they also said everything they do post-COVID will be
in light of the fact that they’re post-COVID,” so maybe the final MFAR
rule won’t be as bad as people fear, Salo said in a phone interview.
“But you can’t bank on any of that.”
In an ideal world, Congress would rescind MFAR entirely, the rule’s
critics say, but that hasn’t happened yet. “We sent a letter to Congress
recently calling for Congress to rescind the regulation, and sent a
letter to the administration asking for the same thing,” Murray, of
ACAP, said in a phone interview. “Ideally, they would rescind it, but if
they can’t do that, could they at least delay it?”
With the comment period for the rule now closed, CMS is now in a
period of finalizing the rule. The agency did not respond by press time
to a request for comment on this story.
With the comment period for the rule now closed, CMS is now in a
period of finalizing the rule. Asked to comment on this story, a
spokesperson responded in an email that “in light of the 2019 Novel
Coronavirus outbreak, CMS is looking closely at all its policies and
across all its programs to see where we can strengthen the nation’s
response.” Since MFAR is only a proposed rule, “no current regulations
have been changed” yet, the spokesperson added.
https://www.medpagetoday.com/publichealthpolicy/medicaid/85798
It’s the most
dramatic government intervention into our lives since World War II. To
fight the coronavirus outbreak, governments across the globe have closed
schools, travel and businesses big and small. Many observers have
fretted about the economic costs of throwing millions of people out of
work and millions of students out of school.
Now, three weeks after the
United States and other countries took sweeping suppression steps that
could last months or more, some public health specialists are exploring a
different consequence of the mass shutdown: the thousands of deaths
likely to arise unrelated to the disease itself.
The longer the suppression
lasts, history shows, the worse such outcomes will be. A surge of
unemployment in 1982 cut the life spans of Americans by a collective two
to three million years, researchers found.
During the last recession, from 2007-2009, the bleak job market helped
spike suicide rates in the United States and Europe, claiming the lives
of 10,000 more people than prior to the downturn. This time, such
effects could be even deeper in the weeks, months and years ahead if, as
many business and political leaders are warning, the economy crashes
and unemployment skyrockets to historic levels.
Already, there are reports
that isolation measures are triggering more domestic violence in some
areas. Prolonged school closings are preventing special needs children
from receiving treatment and could presage a rise in dropouts and
delinquency. Public health centers will lose funding, causing a decline
in their services and the health of their communities. A surge in
unemployment to 20% – a forecast now common in Western economies – could
cause an additional 20,000 suicides in Europe and the United States
among those out of work or entering a near-empty job market.
None of this is to
downplay the chilling death toll COVID-19 threatens, or to suggest
governments shouldn’t aggressively respond to the crisis.
“Depressions are deadly for people, poor people especially.”
A recent report by
researchers from Imperial College London helped set the global lockdown
in motion, contending that coronavirus could kill 2 million Americans
and 500,000 people in Great Britain unless governments rapidly deployed
severe social distancing measures. To truly work, the report said, the
suppression effort would need to last, perhaps in an on-again, off-again
fashion, for up to 18 months.
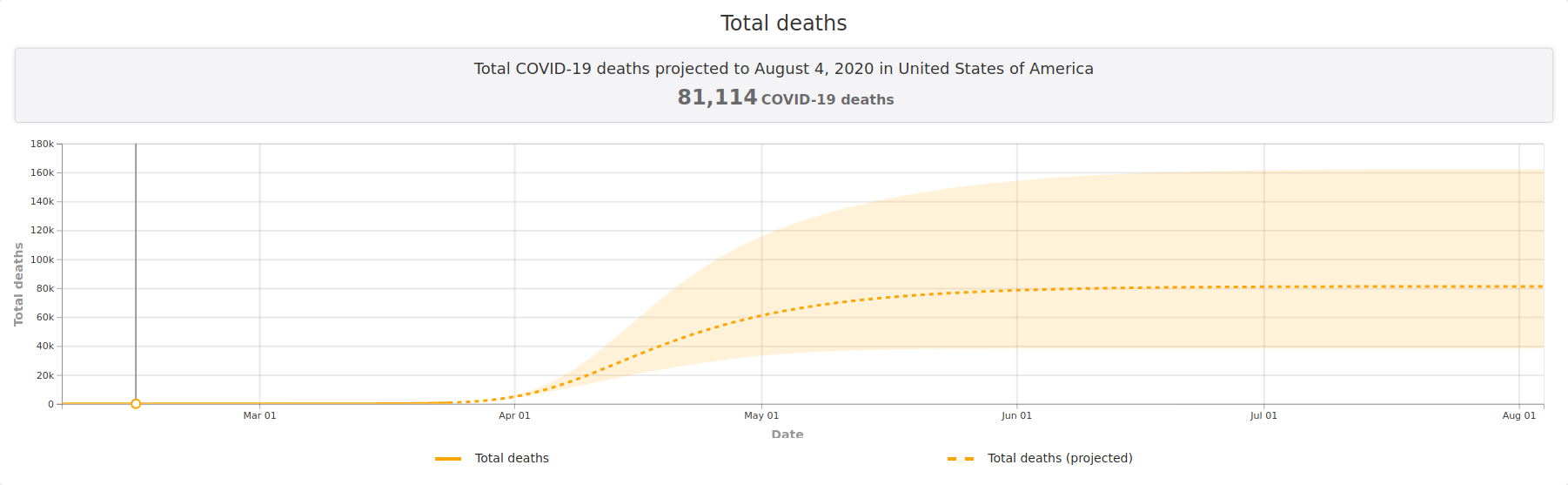
In the United States, the
White House this week said the final toll could rise to 240,000 dead.
States have responded to the dire warnings, and the escalating number of
cases revealed each day, by extending stay-at-home shutdowns.
The medical battle against
COVID-19 is developing so rapidly that no one knows how it will play
out or what the final casualty count will be. But researchers say
history shows that responses to a deep and long economic shock, coupled
with social distancing, will trigger health impacts of their own, over
the short, mid and long term.
Here is a look at some.
Domestic Violence
Trapped at home with
their abusers, some domestic violence victims are already experiencing
more frequent and extreme violence, said Katie Ray-Jones, the chief
executive officer of the National Domestic Violence Hotline.
Domestic violence
programs across the country have cited increases in calls for help, news
accounts reported – from Cincinnati to Nashville, Portland, Salt Lake
City and statewide in Virginia and Arizona. The YWCA of Northern New
Jersey, in another example, told Reuters its domestic violence calls
have risen up to 24%.
“There are special
populations that are going to have impacts that go way beyond COVID-19,”
said Ray-Jones, citing domestic violence victims as one.
Vulnerable Students
Students, parents and
teachers all face challenges adjusting to remote learning, as schools
nationwide have been closed and online learning has begun.
Some experts are
concerned that students at home, especially those living in unstable
environments or poverty, will miss more assignments. High school
students who miss at least three days a month are seven times more
likely to drop out before graduating and, as a result, live nine years
less than their peers, according to a Robert Wood Johnson Foundation report.
Among the most
vulnerable: the more than 6 million special education students across
the United States. Without rigorous schooling and therapy, these
students face a lifetime of challenges.
Special needs students “benefit the most
from highly structured and customized special education,” said Sharon
Vaughn, executive director of the The Meadows Center for Preventing
Educational Risk at the University of Texas. “This means that they are
the group that are most likely to be significantly impacted by not
attending school both in the short and long term.”
In New Jersey, Matawan’s
Megan Gutierrez has been overwhelmed with teaching and therapy duties
for her two nonverbal autistic sons, eight and 10. She’s worried the
boys, who normally work with a team of therapists and teachers, will
regress. “For me, keeping those communications skills is huge, because
if they don’t, that can lead to behavioral issues where they get
frustrated because they can’t communicate,” Gutierrez said.
Soaring Suicides
In Europe and the United States, suicide rates rise about 1% for
every one percentage point increase in unemployment, according to
research published by lead author Aaron Reeves from Oxford University.
During the last recession, when the unemployment in the United States
peaked at 10%, the suicide rate jumped, resulting in 4,750 more deaths.
If the unemployment rate increases to 20%, the toll could well rise.
“Sadly, I think there is a
good chance we could see twice as many suicides over the next 24 months
than we saw during the early part of the last recession,” Reeves told
Reuters. That would be about 20,000 additional dead by suicide in the
United States and Europe.
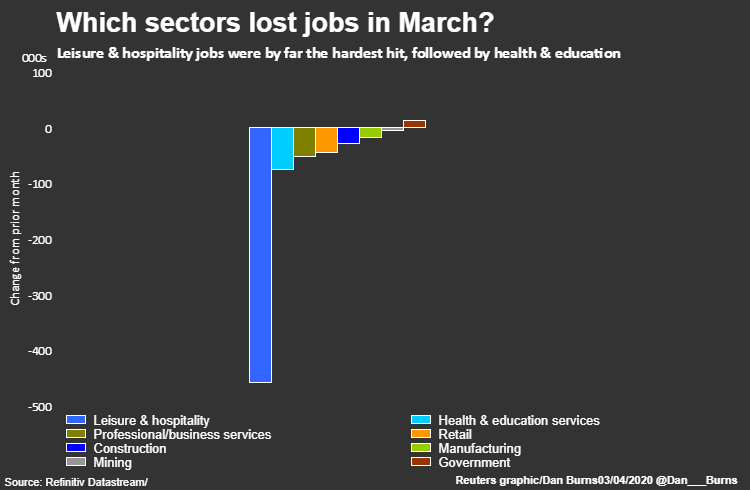
Less than three weeks
after extreme suppression measures began in the United States,
unemployment claims rose by nearly 10 million. Treasury Secretary Steven
Mnuchin warned the rate could reach 20% and Federal Reserve economists
predicted as high as 32%. Europe faces similarly dire forecasts.
Some researchers caution
that suicide rates might not spike so high. The conventional wisdom is
that more people will kill themselves amid skyrocketing unemployment,
but communities could rally around a national effort to defeat COVID-19
and the rates may not rise, said Anne Case, who researches health
economics at Princeton University. “Suicide is hard to predict even in
the absence of a crisis of Biblical proportions,” Case said.
This week, the Air Force
Academy in Colorado Springs, Colorado, relaxed its strict social
isolation policies after the apparent suicides of two cadet seniors in
late March, The Gazette, a Colorado Springs newspaper, reported. While
juniors, sophomores and freshmen had been sent home, the college seniors
were kept isolated in dorms, and some had complained of a prison-like
setting. Now, the seniors will be able to leave campus for drive-thru
food and congregate in small groups per state guidelines.
Public Health Crippled
Local health departments
run programs that treat chronic diseases such as diabetes. They also
help prevent childhood lead poisoning and stem the spread of the flu,
tuberculosis and rabies. A severe loss of property and sales tax revenue
following a wave of business failures will likely cripple these health
departments, said Adriane Casalotti, chief of government affairs with
the National Association of County and City Health Officials, a
nonprofit focused on public health.
After the 2008 recession, local health departments in the U.S. lost 23,000 positions as
more than half experienced budget cuts. While it’s become popular to
warn against placing economic concerns over health, Casalotti said that,
on the front lines of public health, the two are inexorably linked.
“What are you going to do when you have no tax base to pull from?” she
asked.
Carol Moehrle, director
of a public health department that serves five counties in northern
Idaho, said her office lost about 40 of its 90 employees amid the last
recession. The department had to cut a family planning program that
provided birth control to women below the poverty line and a program
that tested for and treated sexually transmitted diseases. She worries a
depression will cause more harm.
“I honestly don’t think we could be much leaner and still be viable, which is a scary thing to think about,” Moehrle said.
Job-loss Mortality
Rises in unemployment
during large recessions can set in motion a domino effect of reduced
income, additional stress and unhealthy lifestyles. Those setbacks in
income and health often mean people die earlier, said Till von Wachter, a
University of California Los Angeles professor who researches the
impact of job loss. Von Wachter said his research of past surges in
unemployment suggests displaced workers could lose, on average, a year
and a half of lifespan. If the jobless rate rises to 20%, this could
translate into 48 million years of lost human life.
Von Wachter cites
measures he believes could mitigate the effects of unemployment. The
Coronavirus Aid, Relief, and Economic Security Act approved by the White
House last week includes emergency loans to businesses and a short-time
compensation program that could encourage employers to keep employees
on the payroll.
Young People Suffer
Young adults entering the job market during the coronavirus suppression may pay an especially high price over the long term.
First-time job hunters seeking work during periods of high unemployment live shorter and unhealthier lives, research shows.
An extended freeze of the economy could shorten the lifespan of 6.4
million Americans entering the job market by an average of about two
years, said Hannes Schwandt, a health economics researcher at
Northwestern University, who conducted the study with von Wachter. This
would be 12.8 million years of life lost.
Thousands of college
graduates will enter a job market at a time global business is frozen.
Jason Gustave, a senior at William Paterson University in New Jersey who
will be the first in his family to graduate from college, had a job in
physical therapy lined up. Now his licensure exam is postponed and the
earliest he could start work is September.
“It all depends on where the economy goes,” he said. “Is there a position still available?”
In the weeks ahead, a clearer picture of
the disease’s devastation will come into focus, and governments and
health specialists will base their fatality estimates on a stronger
factual grounding.
As they do, some public
health experts say, the government should weigh the costs of the
suppression measures taken and consider recalibrating, if necessary.
Dr. Jay Bhattacharya, who
researches health policy at Stanford University, said he worries
governments worldwide have not yet fully considered the long term health
impacts of the impending economic calamity. The coronavirus can kill,
he said, but a global depression will, as well. Bhattacharya is among
those urging government leaders to carefully consider the complete
shutdown of businesses and schools.
“Depressions are deadly for people, poor people especially,” he said.
https://www.reuters.com/investigates/special-report/health-coronavirus-usa-cost/