by David Hebert via TheDailyEconomy.org,
A recent report from The Heritage Foundation argues that “the wealthy” are not “idle idols” but are instead owners and investors of wealth-creating ventures.

Through their ownership of productive assets, they are the driving force behind overall wealth creation in the country and, in some cases, the world. The report reveals a crucial truth that is often lost in today’s political rhetoric: the overwhelming majority of American wealth among the most wealthy (88.2 percent) consists of assets linked directly to businesses and economic production. Despite the commonly accepted belief that millionaires hold their money in real estate or “yachts, sports cars, private planes, gold bars, and jewelry,” most of that wealth is investment, not consumption goods.

Building on this important truth, we emphasize two additional insights that may inform our current policy debates, particularly as the Trump administration seeks to expand government ownership stakes in private companies.
First, we must acknowledge that capitalism, for all its flaws in practice, is fundamentally a system that rewards serving others, not exploiting them.
Look at Henry Ford: he benefited tremendously from figuring out how to mass produce cars such that the common man was able to afford a vehicle. But I submit to you that, while he became fabulously wealthy from his innovations, the real winners of this exchange were people like you and me. Everyday Americans received better access to transportation, fundamentally transforming our lives. People like Ford already had access to this then-privilege, so while he may command more wealth as a result of his efforts, the efforts themselves improved our lives much more than his.
The people who create medical treatments and vaccines against disease also often become wealthy. But when people all around the world are freed from contracting diseases, enjoying a fundamentally better and happier life, the wealth gained by their inventors seems small.
Or think of tech moguls like Bill Gates, Steve Jobs, and Tim Cook. By bringing computing power to the masses, they fundamentally transformed the way we all live our everyday lives.
Consider this ad for computers from 1990:
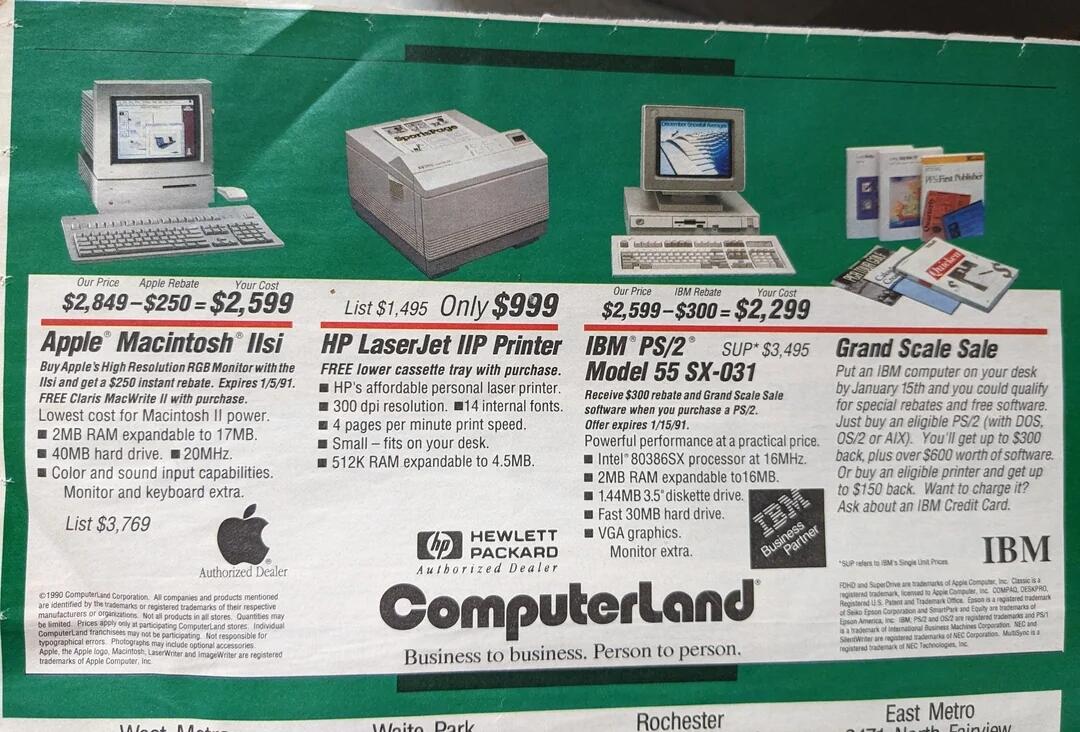
In today’s dollars, these items would cost $6,590, $2,533, and $5,829, respectively. Also in 1990, the average nominal pay for the whole United States was $23,602, meaning that the average person would have to work 220 hours, 84 hours, and 194 hours respectively, to buy these items. Today, with an average wage of $36.44 ($72,880 annually), the hours worked to afford these items (at their 2025 prices) would be 181, 70, and 160.
But we wouldn’t be buying computer equipment from 1990, anyway. Computer prices have actually fallen dramatically. At the time of this writing, a comparable baseline iMac costs $1,299 (35 hours of work). The latest LaserJet printer from HP costs $169 (4.6 hours). IBM sold its computer hardware division to Lenovo in 2005, and a Lenovo desktop computer now costs $859 (23.5 hours). Even if we ignore the massive improvements in quality and the explosion of computing power contained in those devices, computing power has never been more affordable. Millions of careers were transformed by the efforts of Bill Gates, Steve Jobs, Tim Cook, and everyone else from engineer to assembly line at Microsoft and Apple. And while the CEOs and employees of these companies have surely become wealthier, the real winners of the innovations are everyday people like you and me.
In a free society characterized by capitalism, wealth is generated by serving others.
Those who can best serve others — and consume less than they generate — find themselves amassing what we define as “wealth.”
The second lesson we can glean from the Heritage study is what the ultra-wealthy actually do with the wealth they amass. Nearly 90 percent of their fortunes are tied up in productive economic activity, not luxury consumption. Only three percent of the top one percent’s wealth is in consumer durables — things like cars, furniture, and jewelry. For the bottom quintile, that ratio is likely to be 15-20 percent.
Far from being “idle rich,” the wealthy invest their fortunes, providing the capital necessary to fund increased economic activity. For the rest of us, that means more jobs, more production, and better access to the goods and services that enable us to live healthily and wealthily, however we choose to define these terms.
That investment cycle also helps explain why “eating the rich” is a recipe for disaster. Sticking the rich with exorbitant federal taxes can only mean that wealth is removed from productive economic uses to pay for public sector malfeasance. Policymakers are not taking gold coins out of a swimming pool à la Scrooge McDuck, they’re taking investments out of the private sector. The loss of capital impacts not the rich, primarily, but the prosperity that the rest of us have come to enjoy and depend upon.
The reality is that the wealth of the wealthiest people in America largely represents the market’s assessment of their ability to continue serving their customers in the future. As new information comes to light, this assessment can and does change. Tesla, for example, started off white-hot, with stock prices skyrocketing. But lately, after the abysmal launch of the Cybertruck and delays in its production and delivery, combined with some of Musk’s stupendously bad investments, the market has revised its assessment of Tesla downward. As a result, Musk has lost more than $80 billion in wealth thus far in 2025 alone.
This brings us to a troubling development: President Trump, Congressional Republicans, and members of the so-called New Right have recently floated the idea that we should tax the rich more. Even more alarmingly, these same people hold that the federal government should take equity stakes in private companies. This is a fundamental departure from the principles that allowed for the creation of the wealth policymakers now wish to strip away, and a complete rejection of lower-tax, small-government Republicanism.
President Trump is “taking a 10 percent stake in Intel,” making the federal government the single largest stakeholder of the company. Earlier this year, the sale of US Steel to Nippon was approved, contingent on the US government receiving a “golden share.” While Trump is in office, this golden share is held by the President (i.e. Donald Trump), and after he leaves office, it will revert to being held by the Treasury and Commerce Departments. Importantly, while he is in office, the President will have veto power over some production and wage decisions. Not wishing to be left behind, the Pentagon is taking a 15 percent stake in MP Materials, a producer of rare-earth magnets, among other things.
All of this shifts the nation away from the capitalism that created an economy (and indeed, society) the likes of which has never been seen in human history and toward the type of capitalism found in, say, China. Trying to “out-China” China is a fool’s errand.
The reality is that economies, societies, and the nation itself are best served when individual people are given the freedom and tools to succeed, not when government bureaucrats pick winners and losers.
In a free-market, capitalist system like the one the US for the most part enjoys, the best way to serve oneself is by serving others.
https://www.zerohedge.com/personal-finance/why-eating-rich-undermines-everyones-prosperity






{kind=link}