The Justice Department has charged an alleged high-ranking member ofTren de Araguain Colombia with terrorism offenses, making the first case of its kind against a member of the gang the Trump administration has designated aforeign terrorist organization, officials said Wednesday.
The case is part of a broad push to target Tren de Aragua or TdA, a Venezuelan gang that has been blamed for drug smuggling and violence in the United States. President Donald Trump has labeled the gang an invading force under an 18th century wartime law to deport Venezuelan migrants to a notorious El Salvador prison as part of Trump's sweeping immigration crackdown.
The Justice Department's application of a criminal statute primarily reserved in recent years for extremist groups such as the Islamic State and al-Qaida underscores the extent to which the administration is relying on a strikingly expansive definition of terrorism as it pursues a national security agenda focused on drug trafficking and illegal immigration.
“TdA is not a street gang – it is a highly structured terrorist organization that put down roots in our country during the prior administration,” Attorney GeneralPam Bondisaid in a statement. “Today’s charges represent an inflection point in how this Department of Justice will prosecute and ultimately dismantle this evil organization, which has destroyed American families and poisoned our communities.”
Jose Enrique Martinez Flores, 24, was charged in Texas federal court with drug offenses as well as conspiring to provide and providing material support to a designated foreign terrorist organization. Prosecutors described him as part of the “inner circle of TdA leadership,” and accuse him of playing a role in the international distribution of cocaine.
He is in custody in Colombia awaiting further proceedings. The Justice Department said he faces up to life in prison.
The material support statute has long been a favored tool of the Justice Department to build prosecutions against people who are suspected of facilitating the operations of a militant group but not always carrying out violence themselves.
The addition of TdA to the State Department list of foreign terrorist organizations enables the Justice Department to wield the statute against individuals suspected of supporting that group.
In 2021, the Biden administration secured $42.5 billion from Congress to extend broadband Internet access to small and ever-shrinking portions of the country that didn’t yet have it. Four years later, that federal program still hasn’t connected one single person to the Internet.
Elon Musk’s DOGE efforts have so far uncovered tens of billions more in “waste, fraud, and abuse.” For example, the $40 billion USAID budget, DOGE found, is bloated with billions for indefensible bilge — from sex changes in Guatemala to tourism in Egypt.
Is there anyone in his right mind who would argue that the federal government stimulated the economy by this spending? Or if the money instead had been left in the private sector, it would have hurt the economy? Is it humanly possible to waste other people’s money more thoroughly than the government does?
Imagine a pickpocket who steals cash from the wallets and purses of unsuspecting shoppers in a mall. Then he goes from store to store and spends the loot. Whether or not he stimulated the mall economy depends on whom you interview — shopkeepers who are grateful for the pickpocket’s patronage or the thief’s dispirited victims who discover they must go home empty-handed.
When we employ our instinctive common sense, especially if we zero in on egregious and inexcusable profligacy, we are drawn to the conclusion that Milton Friedman expressed so well: “Nobody spends somebody else’s money as carefully as he spends his own.” Moreover, robbing Peter to pay Paul makes Paul richer but Peter equally poorer at the least.
But if we adopt a Keynesian “macro” perspective, we will assert that more government spending energizes economic activity, and that less government spending sends the economy into a tailspin. Is it not simply amazing that politicians possess such powers the rest of us do not?! When they spend your money, the magical multiplier kicks in, but when you and I spend our money (or save it in the bank so the bank can spend it), we just don’t get the same bang for the buck. Just think how prosperous we would be if we laundered everything through the government (like they do in poverty-stricken North Korea).
John Maynard Keynes himself once claimed that if the government simply paid people to dig holes and fill them back in, we could stimulate the economy. It didn’t matter to him what the government spent it for so long as it was the government doing the spending. In any event, he flippantly declared, “In the long run, we’re all dead anyway.”
If DOGE ends up cutting federal expenditures by the trillion dollars or more that Musk has promised, expect every unrepentant Keynesian to warn of dire consequences. It would be the same wrong-headed thinking that led Keynesians in the 1940s to predict another depression when World War II ended.
If another depression is in our future, it will not occur because government spends less. When it did spend less — decisively less — after World War II, depression didn’t materialize. Just the opposite.
Under the influence of the Keynesian consensus, a committee chaired by New York Senator James Mead issued a report in 1945. It argued that with the imminent end of the war, “the United States would find itself largely unprepared to overcome unemployment on a large scale.” Even President Harry Truman, in September of that year, told TheNew York Times that it was “obvious” that the process of reducing federal employment and spending would yield “a great deal of inevitable unemployment.” Indeed, between June 1945 and June 1946, more than ten million people were lopped off the federal payroll (mostly military), and millions returned from overseas to the US job market, while Keynesians held their breath and expected the worst.
One of the best assessments of what actually happened, in contrast to the Keynesian forecasts echoed by future Nobel laureates Paul Samuelson and Gunnar Myrdal, is that of economist David Henderson. In a November 2010 paper for the Mercatus Center titled The US Post-War Miracle, Henderson noted,
In the four years from peak World War II spending in 1944 to 1948, the US government cut spending by $72 billion — a 75-percent reduction. It brought federal spending down from a peak of 44 percent of gross national product (GNP) in 1944 to only 8.9 percent in 1948, a drop of over 35 percentage points of GNP.
While government spending fell like a stone, federal tax revenues fell only a little, from a peak of $44.4 billion in 1945 to $39.7 billion in 1947 and $41.4 billion in 1948. In other words, from peak to trough, tax revenues fell by only $4.7 billion, or 10.6 percent. Yet, the economy boomed. The unemployment rate, which was artificially low at the end of the war because many millions of workers had been drafted into the US armed services, did increase. But during the years from 1945 to 1948, it reached its peak at only 3.9 percent [italics mine] in 1946, and, for the months from September 1945 to December 1948, the average unemployment rate was only 3.5 percent.
Let that sink in: Federal spending plummeted by 75 percent. Millions re-entered the private job market. Yet unemployment remained lower than it is today, and the economy took off. Keynesians, with all their vaunted “New Economics” and sophisticated equations, got it dead wrong. Common sense would have served them much better.
One reason for the unexpected post-war “economic miracle” was the Revenue Act of 1945. Go to the search engine Bing.com. Type in “top corporate income tax rate 1944,” tap “Enter” and voila! The resulting number is staggering: 94 percent. Next, just change one digit in your search terms, from 1944 to 1945. The new figure? 38 percent. The Revenue Act cut marginal tax rates (on both business and personal income) a little, but more importantly, it eliminated surtaxes such as an “excess profits tax” that had driven rates so high.
You need only common sense, no equations required, to know that there’ll be a whole lot more risk-taking entrepreneurship and business investment when you cut tax rates dramatically.
Another reason for the boom was the abolition of all price controls. We had plenty of them during the war, but by 1946, they were all gone. Prices were freed to reflect supply and demand conditions in the marketplace, not the arbitrary whims of Congress or bureaucracies. The rationing of consumer goods ended as well.
Prone to mathematize and oversimplify, Keynesians love to boil an economy down to three main components: Consumption plus Investment plus Government Spending, they claim, equals GNP. C + I + G = Y is the Keynesian formula we all had to learn from our Keynesian economics profs. Their ideological bias prevented them from understanding that when there’s a lot less G, there’s a lot more C and I. That’s because ultimately, G has nothing that it doesn’t sooner or later take from C and I. This would be true even if G didn’t waste a penny.
Common sense tells me that the 75 percent reduction in federal spending after the war may have been the most significant contributor to the economic boom. It diverted resources away from blowing things up on the battlefield. Instead, we could now make cars, refrigerators, and an array of consumer goods of which Americans had been deprived for years. At the very least, the Keynesian fear that massive government spending cuts would tank the economy proved to be utterly and embarrassingly unfounded.
The US boom was no outlier. Once post-war Germany under Ludwig Erhard placed its faith in markets instead of government spending, the world began referring to “the German economic miracle.” Japan experienced a “Japanese economic miracle” for similar reasons. Hong Kong pursued smaller government/free-market policies after the war and awed the world with decades of phenomenal growth. Meantime, under a new socialist government, Britain plunged headlong into an expensive welfare state and became, by the 1970s, the “sick man of Europe.”
In the 1980s, New Zealand transformed itself from a slow-growth welfare state into a free and vibrant economy. In just two years, it slashed government spending from 60 percent of GDP to 40 percent. Once again, Keynesians expected a bust, but the country got a boom instead.
Some people besotted with Keynesian hangovers are worried that if DOGE cuts federal spending a lot, the American economy will lose the “stimulus” we somehow get from it all. But considering both common sense and the historical track record, our biggest concern should be that DOGE won’t cut enough.
Lawrence W. (“Larry”) Reed is the President Emeritus, Humphreys Family Senior Fellow, and Ron Manners Global Ambassador for Liberty at the Foundation for Economic Education.
If “immigrants do jobs that Americans won't do”, there should be occupations in which the workers are overwhelmingly foreign-born. However, among hundreds of occupations identified by the Census Bureau, natives outnumber immigrants in all but a handful, and in none of them do illegal immigrants constitute a majority. The willingness of natives to work a broad range of jobs is even more apparent in low-immigration localities. “There are jobs Americans won’t do” is clearly not a strong argument for immigration.
Overall findings:
Of the 525 civilian occupations identified in Census Bureau data, only five are majority immigrant (either legal or illegal) — with just one, “manicurists and pedicurists”, exceeding 60 percent.
The five majority-immigrant occupations account for only 0.6 percent of the civilian U.S. workforce. Moreover, native-born Americans still comprise 40 percent of workers in these occupations.
Many occupations often thought to be overwhelmingly foreign-born are in fact majority native-born:
Maids and housekeepers: 51 percent native
Construction laborers: 61 percent native
Home health aides: 61 percent native
Landscaping workers: 66 percent native
Janitors: 71 percent native
About half of agricultural workers are immigrants, but all agricultural workers — natives and immigrants together — constitute less than 1 percent of the U.S. workforce.
There are 65 occupations in which 25 percent or more of the workers are immigrants. However, these occupations are still held by about one in every nine native-born workers — 16 million natives in total.
Illegal immigrants:
There are no occupations in which illegal immigrants in the data constitute more than one-third of workers.
Illegal immigrants work mostly in construction, maintenance, food service, and agriculture. However, the majority of workers even in these occupations are either native-born or legal immigrants.
Low-immigration metropolitan areas:
The cities and surrounding suburbs of Pittsburgh, St. Louis, Richmond, Nashville, and Columbus are examples of relatively low-immigration areas with relatively high per capita incomes. In these places, the willingness of natives to work stereotypically immigrant jobs is even more apparent:
Taxi drivers: 67 percent native
Painters: 73 percent native
Maids and housekeepers: 76 percent native
Dishwashers: 87 percent native
Janitors: 88 percent native
Among the 431 occupations with sufficient data to analyze in these five low-immigration areas, just 13 are at least 25 percent immigrant.
Jason Richwine is a resident scholar at the Center for Immigration Studies, a Washington, DC-based research institute that examines the impact of immigration on the United States. He has written and spoken widely on issues of labor economics, both for a technical audience and for the general public. His work has appeared in publications ranging from Public Administration Review and Brookings Institution Press to the Wall Street Journal and Washington Post. He is also a regular contributor to National Review.
The first season of DOGE has been entertaining and transformative. The joy of watching the cronies and the parasites howl has been long overdue for budget hawks like me. But DOGE is just scratching the surface of government waste.
Limiting the size of the federal workforce is child’s play in comparison to taking on the welfare state. Figuring out how to fix the Social Security Ponzi scheme. Fixing the sprawling welfare programs that sign up a lot of people while ignoring those most in need because they are hardest to sign up. Or fixing a healthcare system that drives up the cost while ignoring cost, access, and quality. The spending in these programs threatens to overwhelm all government in the (rapidly approaching) years ahead if nothing is done. This is what DOGE can do to truly shape the government going forward.
Some reforms are easier than others when addressing the welfare state, and it would make sense if they started with some of the low-hanging fruit. One of the easiest fixes is to the current hospital payment structure.
In every market, except healthcare, bigger equals more affordable. This is because as companies increase in size, so does their efficiency. Large hospitals should be able to buy everything cheaper because they buy more of it – all the way down to the Band-Aids, and all the way up to their insurance. It is simple math that we see every day as we drive past Walmart and Target. The greater the volume, the lower the price. That is one of the reasons that businesses vertically integrate, and this type of cost refinement that is one of the first questions asked on Shark Tank.
From a hospital’s point of view, the greed makes sense – why not claim that something is expensive if the government is paying? However, the government’s days of blank checks need to end. If the government pays independent doctors an amount that they think is sufficient because they still take these patients, then large hospitals should be perfectly fine with that same amount of money. In fact, if hospitals were just paid the same amount as independent physicians, they would profit much more.
The policy solution is called Site-Neutral payments. If a patient is getting an injection at a hospital or an independent physician’s office, then taxpayers should pay the same for the treatment at both locations. This simple, rational, and fair idea would save taxpayers an estimated $150 billion over 10 years. That savings alone would get DOGE a significant percentage toward their goal of $1 trillion in savings and wouldn’t affect access or quality in healthcare.
Additionally, this would change the economics of healthcare, helping stop the further erosion of competition. Currently, because of government overpayments, hospitals are buying up independent physician practices around the country. This means that the $150 billion in savings is just the tip of the iceberg on the effect to the system. Correcting this change gives independent physicians a reason to stay solo. It gives them a reason both to innovate and to compete on price – the way Walmart and Target do. This additional competition increases access, increases quality, and hopefully lowers cost even further.
Fortunately, for DOGE this issue has already been discussed and debated on Capitol Hill and the support for reform is bipartisan. Last Congress the Lower Cost More Transparency (LCMT) bill passed out of the House with a bipartisan majority. The LCMT narrowly created Site Neutral payments for drug administration, but even that was forecast to save $50 billion. And the intelligence on the ground was that there was likely enough support to pass something much broader getting at the full $150 billion.
It is almost certain that DOGE will also look at other issues in healthcare policy like Medicare and Medicare Advantage waste, fraud, and abuse and pharmacy benefit managers and their manipulation of drug prices. These issues will also have bipartisan support, but starting an issue that already momentum and offers such large saving seems like one of the easiest decisions that DOGE could make.
This next iteration of DOGE is going to be the test. Can they really reform government, or are their reforms just going to be superficial? Real reformation will come from fixing the welfare state. It also doesn’t mean that the welfare state needs to go away. It merely means that the money should go where it is intended, to help the people that it is intended to help, and most importantly at an amount that actually makes economic and market sense.
Charles Sauer is president of the Market Institute and author of “Profit Motive: What Drives the Things We Do.”
The last four months have been a whirlwind of change in the gender debate. Just eight days into his second term, President Donald Trump signed an executive order provocatively titled “Protecting Children from Chemical and Surgical Mutilation.” It declared that the United States would no longer “fund, sponsor, promote, assist, or support the so-called ‘transition’ of a child from one sex to another.” The order arrived as the Supreme Court was deliberatingU.S. v. Skrmetti, a pivotal case challenging Tennessee’s ban on sex-trait modification procedures for minors.
As the U.S. enters an era of legal warfare over pediatric “gender-affirming” care, it’s time to shift the terms of debate from outcomes to the foundational premises of the practice.
I have served as an expert witness for several court cases on gender-affirming care. These courtroom debates fixate almost entirely on whether the treatments show evidence of benefit. This is a mistake.
True, the evidence is almost nonexistent. Last year, British authorities released the Cass Review, a devastating critique of the evidence supporting pediatric sex-trait modification. The report was grounded in seven systematic evidence reviews—the gold standard in evidence-based medicine. One of the reviews, consistent with the others, described the evidence in favor of “gender-affirming treatment” in children and adolescents as “remarkably weak.”
But while it’s not wrong to highlight this evidentiary void, focusing solely on outcomes cedes too much ground to proponents by implying that outcomes alone could legitimize the practice gender transition. The deeper flaw in gender-affirming care lies not in the data but in their premises. If the foundational assumptions used to justify these treatments collapse under scrutiny, the interventions would remain unjustifiable, even if some evidence of benefit eventually emerged.
At its core, gender-affirming care rests on two claims. First, it posits that biological sex is not a fixed binary but a malleable continuum, shaped by traits like sex chromosomes, hormones, genital morphology, and other physical characteristics—most of which doctors can alter with hormones and surgeries. Second, it asserts that a person can have a “brain sex”—equated with “gender identity”—that diverges from his body, creating a mismatch that drives gender dysphoria. The goal, then, is to align the body with this purportedly immutable “brain sex” through hormones and surgeries.
Both premises are scientifically untenable. Sex is not a spectrum. It’s a binary biological reality defined by reproductive function: males have the function to produce sperm, and females, ova. No hormonal or surgical intervention can change a person’s sex. Likewise, the notion that a person can have a “brain sex” incongruent with his body defies both biology and logic. Our bodies are an integrated whole, not a patchwork of independently sexed traits.
These unsound premises make gender-affirming care a house built on sand, not solid medical science.
Consider an analogy: exorcism might comfort a troubled patient who believes in demonic possession, but the practice’s legitimacy hinges on demons being real. Absent that, it’s a ritual, not medicine. Similarly, gender-affirming care presupposes both a “sex spectrum” and “brain sex,” which do not exist. No amount of reported benefit can salvage a practice rooted in pseudoscience.
This distinction exposes a contradiction among the defenders of gender medicine in U.S. v. Skrmetti. The litigants against Tennessee argue that bans on “gender-affirming” procedures for minors constitute a form of discrimination based on sex. The ACLU, representing private plaintiffs in the case, attempted to spotlight potential benefits of gender-affirming care while sidestepping the shaky premises, yet its legal arguments invoking sex discrimination implicitly relied on sex being concrete and immutable. This undermines the justification for the gender-affirming care it supports, which requires that sex be fluid and changeable. They can’t have it both ways.
The legal battle over gender-affirming care must shift focus. Legislation should not merely target procedures but dismantle the pseudoscientific terminology and concepts—“gender identity,” “brain sex,” and “sex assigned at birth”—that prop them up. Medical institutions must face accountability for embracing these falsehoods.
This is a rare moment to halt the medicalization of confused, distressed, and vulnerable youth. By attacking gender medicine at its ideological foundation, we can end this harmful practice.
Colin Wright is an evolutionary biologist and fellow at the Manhattan Institute.
Why should you care about the curious case of Dr. Peter Marks, MD, PhD? The recently resigned head of the FDA Center for Biologics Evaluation and Research (CBER)? Because Dr. Peter Marks provides an excellent case study of what happens when the government settles for acceptable instead of excellent in scientific administrator (bureaucrat) positions.
It is hard to find experienced, top-tier minds to fill government jobs. The salary is about 2/3 or less of comparable positions in industry, particularly in the pharmaceutical industry. Hardly a good way to raise a family and buy that five-bed colonial in Alexandria, McClain, or Potomac that would clearly demonstrate to your associates how important you really are. The work is generally a mundane daily grind, with mounds of paperwork interspersed by various required personnel and management activities. Lots of risk if the administrator veers away from standardized processes. There is little opportunity for innovation or discovery. Great minds crave independence. This dynamic is amply illustrated by the huge raises typically enjoyed by almost all of those who leave the government to take positions in Pharma – even the intellectual hacks and wannabees.
What a senior job in government does provide is power and status. You make decisions that massively impact on regulated industry profit and policy. Everyone wants your attention for their pet project. The press fawns on you because of the forces that drive “access journalism.”
Those who can, do. Those who can’t, regulate.
I am reminded of two examples of widely repeated wisdom concerning academia. The first example is that those who actively seek to become Department Chairperson are usually seeking power over their peers, and are the ones who should be specifically avoided when selecting a Department Chair or Dean position. The second is that the reason academic politics are so nasty is that there is so little to fight over.
After his initial selection as Deputy Director CBER, Dr. Marks rapidly rose to prominence in the ranks of the FDA, and was rewarded with a plum high-status appointment to the National Academy of Science – not on the basis of his intellect, scientific achievements, mastery of regulatory science or technical excellence – but because he advocated for reduced regulation of the pharmaceutical industry where he had worked prior to his initial FDA appointment.
At that point, why did you decide to switch career paths?
It was a mix of personal and professional reasons, but a driving factor was that, during my time at Brigham and Women’s, my spouse and I had two children and I wanted to have more family time.
So, I moved to a position in the pharmaceutical industry for a few years. It turned out to be a very productive period of my career: I was involved in the successful regulatory approval of the first oral iron chelator in the US and helped to set the direction for the regulatory approval of two other products that are now on the market.
The work I did there to bring that drug to market was exciting, but the idealist in me wanted to get back to patient care and public health. So, I returned to academic medicine at Yale University. While I was there, I helped expand the adult leukemia service. Eventually, I served as the first chief clinical officer of the then-new Smilow Cancer Center.
After you returned to academic medicine, why did you decide to move to the public sector?
I enjoyed my job at Yale quite a bit, but during that time I happened to see an advertisement in the New England Journal of Medicine for the position of deputy director of the FDA’s Center for Biologics Evaluation and Research (CBER). The job description seemed to match up nicely with my training and experience, so I applied. I didn’t expect much to happen, and that’s exactly what occurred. I got busy with other work and practically forgot that I had applied.
Then, several months later, I received a letter inviting me for an interview. That process went on for months, which ended with me being offered the position. I began as the deputy director of the CBER in January 2012 and took over as director at the beginning of 2016.
Just to say, in the pharmaceutical industry “was involved in” and “helped set the direction for” are other ways of saying “I played a modest role in the team that did these things.” There is no evidence that he held a senior appointment during his time in industry, just as he seemed previously to be on a “clinical” track in his academic medicine appointments – rather underwhelming for a MD, PhD. He seems to have “met expectations” through this pre-FDA phase of his career, but certainly did not exceed expectations.
The ultimate expression of Dr. Marks’ laissez-faire regulatory philosophy was “Operation Warp Speed” (OWS), during which both the regulatory and bioethical framework for gene therapy and vaccine product regulation and clinical testing that had been developed over decades of international experience and consensus was metaphorically thrown in the trash can. All based on hype and flawed modeling indicating a 3.4% case fatality rate (CFR) for SARS-CoV-2 infection, when the true CFR was akin to that of a more severe seasonal influenza outbreak – as demonstrated quite early in the outbreak by current NIH Director Jay Bhattacharya. OWS and the global harms incurred from the various gene therapy-based Covid vaccines that caused patients to produce high levels of the remarkably toxic “spike” protein for prolonged periods all flow directly from the regulatory philosophy and actions of Dr. Peter Marks.
Dr. Marks’ partner in this endeavor was then Assistant Secretary HHS for Pandemic Response (ASPR) Dr. Robert Kadlec, a notorious “deep state” operative with close historic ties to the company that markets the Anthrax vaccine (Emergent Biosolutions), the Defense Intelligence Agency, and Dick Cheney.
During the COVID-19 pandemic I had the privilege of watching the vision that I conceived for Operation Warp Speed in March 2020 in collaboration with Dr. Robert Kadlec become a reality under the leadership of HHS Secretary Azar and President Trump due to the unwavering commitment of public servants at FDA and elsewhere across the government. At FDA, the tireless efforts of staff across the agency resulted in remarkably expediting the development of vaccines against the virus, meeting the standards for quality, safety, and effectiveness expected by the American public. The vaccines undoubtedly markedly reduced morbidity and mortality from COVID-19 in the United States and elsewhere.
Dr. Peter Marks letter of resignation, March 28, 2025
As far as I am concerned, it is hard to make the case that President Donald Trump, whose core competencies are in real estate, business development, marketing, and media was responsible for OWS except for the fact that he was overly dependent on and insufficiently skeptical of the scientific administrators advising him – specifically including Drs. Peter Marks and Robert Kadlec.
Dr. Peter Marks, MD, PhD, decided to leave Federal employment after fourteen years at the FDA Center for Biologics Evaluation and Research (CBER), apparently in response to the Secretary of HHS indicating that he had the option of resigning voluntarily or being terminated for cause. Or so corporate press reports. At the time of his resignation, Dr. Marks had served the public as the Director of CBER since 2016 (three years prior to Covid), and before that had served as Deputy Director CBER from 2012-2016 (source).
As is standard HR practice in these types of personnel actions, the Secretary of HHS, Mr. Robert F. Kennedy, Jr. (or his office), has declined to comment or verify that this is what transpired. Therefore, we have no information as to what the specific cause for termination would have been. What we do have is a copy of Dr. Marks’ FDA resignation letter dated 28 March (attached below) in which he states:
Over the past 13 years I have done my best to ensure that we efficiently and effectively applied the best available science to benefit public health. As you are aware, I was willing to work to address the Secretary’s concerns regarding vaccine safety and transparency by hearing from the public and implementing a variety of different public meetings and engagements with the National Academy of Sciences, Engineering, and Medicine. However, it has become clear that truth and transparency are not desired by the Secretary, but rather he wishes subservient confirmation of his misinformation and lies.
My hope is that during the coming years, the unprecedented assault on scientific truth that has adversely impacted public health in our nation comes to an end so that the citizens of our country can fully benefit from the breadth of advances in medical science. Though I will regret not being able to be part of future work at the FDA, I am truly grateful to have had the opportunity to work with such a remarkable group of individuals as the staff at FDA and will do my best to continue to advance public health in the future.
In performing diligence for this essay, I wanted to understand Dr. Marks’ academic background, scientific achievements, and qualifications for running the dominant Western regulatory authority for biologics, vaccines, blood products, as well as cell and gene therapy, and so searched for information regarding key career milestones for Dr. Marks including his CV or Google Scholar listing (Google Scholar is a leading resource for evaluating academic contributions and standing). Nothing. Nada. Like his history has been wiped from the internet.
He claims to be trained as a Ph.D. Molecular Biologist (why does this matter you ask? See below), but in searching the federal PubMed database I only find five unremarkable cell biology papers during his PhD training. He claims to be a public health expert, but I can find no evidence of formal training or experience in public health, clinical research, or regulatory affairs prior to his joining the FDA. In his academic career he rose to the level of “Instructor,” which is a remarkably modest rank for an MD. PhD. Basically, I can find no evidence of scientific excellence, leadership, or remarkable achievements while investigating the scientific and clinical experience of Dr. Marks.
Why are Dr. Peter Marks’ scientific qualifications and experience important? Why am I focused on nitpicking these nuances? Four main reasons grounded in personal experience:
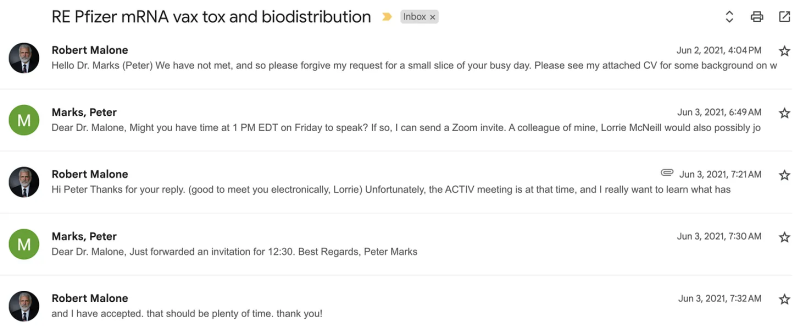
First, I met with him via Zoom on June 03, 2021 to discuss the Pfizer Japanese regulatory submission documents that Dr. Byran Bridle had discovered on a Japanese regulatory affairs server. These documents clearly reported that Pfizer had failed to meet both FDA and worldwide regulatory norms with their non-clinical studies concerning the mRNA Covid vaccine, and yet FDA/CBER/Marks was proceeding with Emergency Use Authorization. My belief at the time was that the FDA was acting in good faith, but lacked the specialized experience required to see through the misleading information that Pfizer had submitted (particularly regarding the biodistribution and toxicities of the injected product and resulting genetic transfer). In that meeting, which was also attended by an FDA PR representative, Dr. Marks indicated that he had seen additional data from Pfizer (what is now commonly referred to as the “Pfizer Papers,”) and that there was nothing there that “concerned” him. Furthermore, Dr. Marks asked me – as an expert in the area – to withhold public criticism until he could release the supporting data.
This was a manipulative ruse and a lie, and I hate being lied to and manipulated. He had no intention of releasing the data to the public, which data eventually required court action for release. Were it not for this like and misdirection, I would have spoken out earlier and more forcefully, but I acted to withhold my criticism out of respect for what I believed was an honest colleague. Furthermore, I remain convinced that Dr. Peter Marks was not then and remains unqualified by training and background to understand the nature and flaws in the non-clinical data submitted by Pfizer in support of this product.
Second, Dr. Peter Marks is inexperienced in the specialized domain of gene therapy technologies and products. His PhD may have been in “Molecular Biology,” but there is no indication that he was rigorously trained in modern Molecular Biology – which is one of my specialities. He is also neither experienced nor trained in vaccinology, nor in immunology. His ignorance in these areas became abundantly clear during the Covid crisis. This inexperience and ignorance, combined with his apparently average scientific acumen, played a key role in enabling the flawed global leadership of the FDA during the Covid crisis. It is important to understand that, during the Covid crisis, the US and specifically the US FDA set the standards for global regulatory policy among all NATO, EU, UK-affiliated, and Five Eyes intelligence network allies. The politicization of regulatory policy within all of these nation-states and super-national organizations flowed directly from the flawed analysis and insights of Dr. Peter Marks.
Third, when confronted by objections to his analysis and decisions by his two top vaccine subject matter experts concerning authorization of the genetic vaccine “booster” shots (Drs. Philip Krause and Marion Gruber), Dr. Peter Marks overruled them. Apparently, due to his sense of ownership of OWS and a certain obstinance and oppositional defiance, which is reflected in comments made in his resignation letter.
Turning to a recent essay from “A Midwestern Doctor” which succinctly summarizes this turn of events:
One of the most important whistleblowers to come forward was Philip Krause, who had worked in the FDA for 30 years. This was because Krause along with his direct superior Marian Gruber had been the most senior FDA officials in charge of America’s vaccines, and at the end of August 2021, in the middle of arguably the FDA’s most critical vaccine assessment in history, they abruptly resigned (which was a seismic enough event the mainstream media covered it and even mentioned it being due to political pressure from White House for the Covid boosters). Following this, Krause and Gruber published an article in the Lancet. Krause also published a series of editorials (e.g., this one, this one, this one in the Washington Post) arguing against the current booster program.
Following this, he testified in front of Congress about how the Covid vaccines were handled.
See the following for details of that testimony-
The entire March 02, 2025 Substack essay titled “Why Did The FDA Greenlight The COVID Vaccines? Recent whistleblower testimonies have revealed the anatomy of corruption within the FDA” is directly relevant to this current discussion concerning the incompetence of Dr. Peter Marks.
Finally, there is the issue of the DNA fragment contamination and adulteration of virtually all of the current “mRNA”-based Covid gene therapy products. Why do I put “mRNA” in quotes? Because these products to not actually employ mRNA – as anyone well trained in molecular biology would readily recognize – but rather employ a heavily modified synthetic mRNA analog more properly referred to as “pseudo-mRNA.” It is this modification that changes short-lived mRNA molecules into material that can be used to produce protein but is not actually mRNA – for which Kariko and Weissman were recognized by the Nobel Prize committee for making the Covid gene therapy technology-based vaccines possible.
As Dr. Kevin McKernan and so many other actual molecular biologists all over the world have documented, the current manufacturing process used to produce these Covid gene therapy-based products yields material that is contaminated – adulterated – with levels of DNA fragments (and sequences) that are neither acceptable nor disclosed to patients and their physicians. Under normal circumstances and under unbiased regulatory oversight, this adulteration issue should have been discovered long before these products were administered to humans.
Furthermore, upon discovery by McKernan and others, the FDA should have immediately launched an investigation and withdrawn these products from the market due to this adulteration. Instead, Dr. Peter Marks, in close coordination with vaccine industry-academic apologist and FDA Vaccine advisory board member Dr. Paul Offit launched an absurd media campaign to deny that the delivery formulations used for the pseudo-mRNA would also deliver the contaminating DNA fragments into patient’s cells.
This action was criminal, in my opinion, and should be both investigated and prosecuted to the extent supported by current federal law. Dr. Peter Marks was not pardoned by outgoing President Biden.
For further details, please see the following Substack essays:
This history of Dr. Peter Marks and his actions during the Covid crisis illustrate the potential consequences of allowing bureaucrat-scientists to set public policy. Dr. Marks could have provided substantial and productive long-term contributions at the FDA. But he was never suited for the position of Director of CBER. He lacked the experience, training, intellect, and temperament for the job. Throughout his career, he repeatedly failed upward, providing a classic example of the ironically named “Peter Principle.” Towards the end of his career as a public servant, he ran out of the FDA two highly qualified and experienced vaccine regulatory experts, both of whom have acted with integrity since that notable decision to leave – in particular Dr. Philip Krause.
Yes, the history of Dr. Peter Marks provides an excellent case study of what happens when the government settles for acceptable instead of excellent in scientific administrator (bureaucrat) positions. But beyond that, this particular example also illustrates a problem that has underpins the incompetency and chronic failure of the entire HHS enterprise to fulfill its primary mission – to protect and improve the health of American citizens. To repurpose and realign the HHS enterprise and bureaucratic infrastructure with the task of Making America Healthy Again will require aggressive reorganization and job cuts to eliminate redundant personnel and eliminate those who have been promoted to “a level of respective incompetence.”
This will disrupt families, cause personal trauma, and some of the good ones will unnecessarily be “made redundant.” This is the nature of organizational restructuring. The general guidance during this type of restructuring is that you should cut more deeply than you really need to, and then immediately begin hiring that aligns more closely to the new priorities and structure.
This is how you run a large business enterprise, and this is what needs doing at HHS. So spare me the tears and the angry backlash of privileged scientist-administrators like Dr. Marks and his ilk. He can take this as an opportunity to re-evaluate his actions, or he can just become another Pharma shill and double his salary. All of this reminds me of the curious case of Dr. Rick Bright – formerly Director of BARDA, who jumped to a nice position with the Rockefeller Foundation after departing HHS in a huff because he was reassigned to solve the problem of faulty Covid testing.
But for the rest of us, we have been damaged by the actions and inactions of Dr. Peter Marks. Global regulatory science, clinical research, and medical ethics have been damaged by his actions. And his emotional outbursts, attacks, and defamation of the Secretary of HHS together with his whining self-importance puts me in no mood to forgive these crimes against humanity and my profession.
Robert W. Malone is a physician and biochemist. His work focuses on mRNA technology, pharmaceuticals, and drug repurposing research.