Israel reported on Monday a decrease in the effectiveness of the Pfizer/BioNTech COVID-19 vaccine in preventing infections and symptomatic illness but said it remained highly effective in preventing serious illness.
The decline coincided with the spread of the Delta variant and the end of social distancing restrictions in Israel.
Vaccine effectiveness in preventing both infection and symptomatic disease fell to 64% since June 6, the Health Ministry said. At the same time, the vaccine was 93% effective in preventing hospitalizations and serious illness from the coronavirus.
The ministry in its statement did not say what the previous level was or provide any further details. However ministry officials published a report in May that two doses of Pfizer’s vaccine provided more than 95% protection against infection, hospitalization and severe illness.
A Pfizer spokesperson declined to comment on the data from Israel, but cited other research showing that antibodies elicited by the vaccine were still able to neutralize all tested variants, including Delta, albeit at reduced strength.
About 60% of Israel’s 9.3 million population have received at least one shot of Pfizer’s vaccine in a campaign that saw daily cases drop from more than 10,000 in January to single digits last month.
This spurred Israel to drop nearly all social distancing as well as the requirement to wear masks, though the latter was partially reimposed in recent days. At the same time, Delta, which has become a globally dominant variant of the coronavirus, began to spread.
Since then daily cases have gradually risen, reaching 343 on Sunday. The number of seriously ill rose to 35 from 21.
Data scientist Eran Segal of Israel’s Weizmann Institute of Science said the country was unlikely to experience the high levels of hospitalizations seen earlier in the year since there were much fewer critically ill.
He said it was fine to “continue with life back to normal and without restrictions” while stepping up measures like vaccination outreach and ensuring testing for Israelis returning home from abroad.
Last week, the CDC's Advisory Committee on Immunization Practices (ACIP) met to discuss the safety signal of myocarditis among young people who receive mRNA vaccination against COVID-19. This dialogue has been months in the making. Ultimately, the panel continued to endorse a two-dose mRNA strategy for all ages. We are concerned with this recommendation and offer five alternative considerations. But first, let's review how we got to this moment in order to make sense of vaccine-induced myocarditis.
A Recent History of Vaccine-Induced Myocarditis
The potential risk for vaccine-induced myocarditis was first raised on February 1 in the Jerusalem Post, which reported the hospitalization and intensive-care admission of a healthy 19-year old male 5 days after receiving his second dose of the Pfizer vaccine. This was followed by a nationwide report in the Times of Israel on April 23, later picked up by Reuters on April 25. These news reports suggested that Israel had seen elevated rates of this event after young men were vaccinated with the Pfizer vaccine, almost always after the second dose (56 out of 62 cases or 90%).
The European Medicines Agency announced an investigation on May 7, which was the same day several of us cautioned against FDA's use of emergency use authorization (EUA) to expedite the availability of COVID-19 vaccines to U.S. kids ages 12 to 15.
Although they were aware of this safety signal, the FDA issued the EUA on May 10 for Pfizer's mRNA vaccine in kids ages 12 to 15. Despite the fact that the vaccine was already widely in use in people ages 16 and above under the existing EUA, specific rates of myocarditis in the U.S. for 'near age' vaccine recipients (kids ages 16 to 18) were not made publicly available. In other words, no data on myocarditis events in kids close in age to the group receiving the new EUA (those ages 12 to 15) were leveraged in the process for granting this EUA. This is unfortunate, as these data would have had the greatest relevance and implications for the adjacent-age group.
Over the last 2 months, several news reports on clusters of cases of myocarditis after mRNA vaccination -- particularly in young men -- have been reported in the U.S. Revised estimates from Israel found the rate of myocarditis to be to one in 3,000 to one in 6,000 among males ages 16 to 24. On May 26, the Times of Israel reported that Israel's health ministry would consider just one dose in teens to balance getting most of the benefit of viral protection against mitigating much of the risk of myocarditis.
On May 22, the CDC announced they had received reports of myocarditis, and asked healthcare providers to file additional and missing reports into the Vaccine Adverse Event Reporting System (VAERS).
Last week, on June 23, ACIP met to discuss the findings. To date, CDC has documented myocarditis in at least 323 cases age 29 or under (of whom 96% were hospitalized), while 148 remain under review. The CDC acknowledged more cases in young people than older people, more cases in young males than young females, and higher incidence after dose two than dose one. The absolute risk of myocarditis after the second dose based on the number of CDC confirmed cases would be one in 15,000 to 20,000 for boys ages 12 to 24. There is a smaller but still excess risk in women age 24 and younger.
At its meeting, ACIP considered figures and data, which claimed to weigh the benefits versus harms of "dose two" of mRNA vaccines in this age group. However, in reality, the scenarios presented by the CDC compared the risks versus benefits to young people of no vaccination at all versus a scenario in which they received both shots.
The CDC did not consider the harms versus benefits of one versus two doses, but only the harms versus benefits of vaccination itself. But the CDC went beyond this. They also used base rates of infection from the past, rather than current rates of SARS-CoV-2 spread, which are substantially lower. They did not differentiate between healthy kids -- who are at risk of idiosyncratic events, such as myocarditis -- and kids with pre-existing medical conditions that place them at high risk of severe outcomes from COVID-19, including hospitalization.
This insistence on an all-or-nothing, one-size-fits-all binary approach -- treating healthy kids who have recovered from confirmed prior infection as equivalent to infection-naive kids with comorbidities -- is at the heart of the fallacy underpinning ACIP's decision.
While we acknowledge the CDC and ACIP had to act based on short-term studies and limited and variable data, vaccines must be used in a way that maximizes benefit and minimizes risk.
Ultimately, the CDC's recommendations came out so unequivocally in favor of vaccination that the following is true: If a 15-year-old recovers from COVID-19 and has high antibody levels, and this 15-year-old then receives one dose of mRNA vaccine causing hospitalization from myocarditis, the CDC would still contemplate proceeding with dose two once the "heart has recovered."
These events raise several points of concern:
VAERS is a suboptimal system. While the VAERS system was well-positioned to detect a rare and entirely unprecedented safety event (e.g., vaccine induced thrombocytopenia and thrombosis in the cerebral vessels), the system is suboptimal for elevations in naturally occurring health outcomes. Voluntary reporting requires a provider to make a mental link between vaccination and the outcome, and the mere fact that the CDC received more cases after coverage in the New York Times is evidence that VAERS failed to capture these events without prompting. This indicates cases may still be underreported: U.S. rates are likely a floor and not a ceiling. The meticulous tracking in Israel is likely closer to the real figure. Facing a factor-of-5 discrepancy between rates reported by Israel and the U.S., it is not prudent to simply assume that Israel is overcounting myocarditis, rather than the other way around.
If you change even one assumption, the CDC's model tips. Using the CDC's own framework of risk and benefit, key differences tip the calculus. First, the comparison doesn't have to be either two doses or no doses. We can also consider just a single dose. Dose two is associated with greater rates of myocarditis, and one dose of an mRNA vaccine has strong protection (over 90% for severe outcomes) -- even against novel variants such as Delta. If you do this, the calculus tips. Second, building on this model, if one assumes rates of myocarditis documented in Israel, accepting the hypothesis that VAERS underestimates risk, it gets even worse. One of us (Wes Pegden, PhD) re-ran the CDC's analysis accounting for this, which shows that second dose vaccination is unfavorable at young ages. Finally, the CDC's analysis uses SARS-CoV-2 rates from the past -- when fewer adults were vaccinated. Rates might rise in the fall, but that's unclear.
Figure by Wes Pegden, PhD
The CDC did not consider alternative strategies. The decision facing the CDC is not whether or not COVID-19 vaccination in children is generally a good idea. Most immediately, it is whether kids ages 12 to 15 should continue to receive second doses. A range of vaccination strategies are possible in children. Believing that COVID-19 vaccines can be valuable even for healthy children is different from thinking we cannot afford to proceed cautiously. Above all, it does not mean CDC should feel a need to stay the course with second doses whose marginal risks in teens appear likely to exceed their marginal benefits. Manufacturers could also reconsider the dose given to young people under 25 years old. Children's vaccination trials currently underway use lower doses than the adult studies; perhaps a lower or intermediate dose of vaccine could preserve most of the anti-COVID-19 benefit while avoiding the myocarditis risk. The CDC did not explore this option. And notably, dose optimization is an area of drug development for which there is a lot of room for improvement.
The CDC is not accounting for COVID-19 risk factors. Vaccination strategies for young people should be responsive to risk factors that place children at elevated risk of severe COVID-19 disease. While it is true that some cases of multisystem inflammatory syndrome in children (MIS-C) are idiosyncratic -- occur even in healthy kids -- the bulk of adolescent hospitalizations are among individuals with pre-existing risk factors. In contrast, the risk of myocarditis is entirely idiosyncratic and can strike anyone, including healthy adolescents at very low risk of severe disease. Vaccinating those at high COVID-19 risk, but not all young people, is a strategy that must be considered when balancing tradeoffs, as the harms versus benefits to healthy children are different than for kids with risk factors.
The CDC is not factoring in natural immunity. It is hard to believe that the risk benefit balance favors a 15-year-old young man who has recovered from COVID-19, and who has detectable antibodies, getting two doses of an mRNA vaccine. Such an individual is accepting a non-negligible risk of myocarditis, with limited upside in terms of decreased risk of severe infection. If the CDC recommends vaccination for these children, it is imperative they weigh benefits versus harms in precisely this population, which, to date, they have not presented.
Immediately after the ACIP meeting, various agencies and professional societies released ajoint statementarguing that the benefit of vaccination far outweighs the risk in all age groups and demographics. Yet, our analysis suggests this is a premature conclusion. It relies on models that use outdated COVID-19 risk rates -- the on-the-ground rates in the moment are far lower, shifting the harm/benefit calculus to harm. It assumes two doses or none at all are the only options. It does not tailor recommendations by sex, natural immunity, or even comorbidities. We acknowledge there are individual and community level benefits to vaccination that extend beyond preventing hospitalizations and are an important part of the discussion. But these omissions from ACIP/CDC are problematic.
The stakes of this decision are no small thing. Even ACIP acknowledged there is a lot we still do not know about myocarditis after vaccination. There are additional cases being adjudicated, including serious ones, and there are no long-term follow-up studies yet to determine, for example, whether documented evidence of myocardial scar may portend an increased risk of arrhythmias. The ACIP and CDC discussion around vaccinating young teenagers, specifically boys, left out reasonably middle ground positions.
True vaccine proponents -- as all of us are -- understand the best thing we can do for vaccines is deploy them in a way that maximizes benefit and minimizes risk. This is crucial to protect health and also to ensure public confidence in the safety of vaccination. The current CDC guidance is not that. It needs to be revisited.
Vinay Prasad, MD, MPH, is an associate professor in the Department of Epidemiology & Biostatistics at the University of California San Francisco. Ramin Farzaneh-Far, MD, is a cardiologist and drug-developer based in Boston. Wes Pegden, PhD, is a mathematician at Carnegie Mellon University. Venk Murthy, MD, PhD, is a cardiologist and associate professor of Medicine at the University of Michigan. Amy Beck, MD, MPH, is a pediatrician and associate professor at the University of California San Francisco.
Disclosures
Prasad has relationships with Arnold Ventures, UnitedHealthcare, eviCore, and New Century Health. Murthy owns stock in Eli Lilly, Pfizer, Johnson & Johnson, and Merck, which are marketing or are developing products related to COVID-19.
The US Army is preparing to enforce mandatory coronavirus vaccinations for service members from the beginning of September, according to an Army Times report.
The report published Saturday notes “The Army has directed commands to prepare to administer mandatory COVID-19 vaccines as early as Sept. 1, pending full Food and Drug Administration licensure.”
“The directive came from an execute order sent to the force by Department of the Army Headquarters,” the report adds.
An update to a purported leaked military directive says that “Commands will be prepared to provide a backbrief on servicemember vaccination status and way ahead for completion once the vaccine is mandated.”
Both the Army and the DoD have denied that there are plans for mandatory vaccinations.
Army spokesperson Maj. Jackie Wren staled that “As a matter of policy we do not comment on leaked documents. The vaccine continues to be voluntary.”
“If we are directed by DoD to change our posture, we are prepared to do so,” Wren added.
The latest study, published in JAMA’s Cardiology Journal on Tuesday, showed that 23 male soldiers (including 22 who were deemed “previously health”) between the ages of 20 and 51 presented “acute onset of marked chest pain” within four days of receiving their second dose. Patients who sought care for chest pain in the military health-care system following COVID-19 vaccination and were subsequently diagnosed with clinical myocarditis were included in the case study.
In the UK, soldiers have been warned that if they decline the vaccine they will face ‘punishment and re-education’.
Tech companies are alreadyat odds with the Hong Kong government, and that tension appears to be on the rise. TheWall Street Journalhaslearnedthat the Asia Internet Coalition, a tech alliance including Facebook, Google and Twitter, has quietly warned Hong Kong that companies would stop operating in the territory if officials move forward with data protection law amendments that could hold companies liable fordoxxingcampaigns.
The tech giants are worried that staff could face criminal investigations or even charges if users share personal info online, even if they didn't mean any harm. That would be a "completely disproportionate and unnecessary response" and could chill free speech, the Coalition wrote. The alliance instead suggested that Hong Kong narrow the scope of violations.
Hong Kong's Privacy Commissioner for Personal Data acknowledged the letter's existence, but said that new measures were needed after doxxing pushed the "limits of morality and the law." The Commissioner also insisted that the changed laws would "not have any bearing" on freedom of speech, and wouldn't deter outside investment in the Hong Kong region.
The amendments could be approved by the end of the legislative year.
The concern, as you might guess, is that pro-China officials might abuse the updated laws to silence dissent. Pro-democracy activists doxxed police officers and others frequently during the 2019 protests, and there's a worry that the revised laws could be worded loosely enough that merely sharing a photo of someone in a public space could get both sharers and tech companies in trouble. It could be harder to hold police accountable for violence, or to criticize officials for anti-democratic policies.
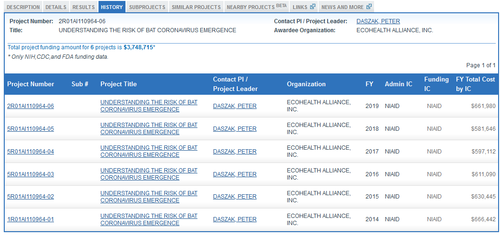
Four monthsbefore the Obama administration suspended federal funding for gain-of-function research on US soil, the process by which virologists manipulate viruses to be more transmissible to humans, a subagency of the National Institutes of Health (NIH) - headed byDr. Anthony Fauci - effectively shifted this research to the Wuhan Institute of Virology (WIV) via agrantto nonprofit group EcoHealth Alliance, headed by Peter Daszak.
The first $666,442 installment of EcoHealth's $3.7 million NIH grant was paid in June 2014, with similar annual payments through May 2019 under the "Understanding The Risk Of Bat Coronavirus Emergence" project, as we noted in April.
As we noted in April, the WIV "had openly participated in gain-of-function research in partnership with U.S. universities and institutions" for years under the leadership of Dr. Shi 'Batwoman' Zhengli, according to the Washington Post's Josh Rogin.
Now, Daszak is refusing to comply with a months-old document request from House Republicans related to his work at the Wuhan lab, according to Just The News.
As government investigators and journalists dig to uncover the full scope of Daszak's links to the WIV, Daszak is continuing to spurn a congressional request for that information.
In April, Republicans on the House Committee on Energy and Commerce sent Daszak a letter directing him to submit, among many other documents, "all letters, emails, and other communications between [EcoHealth] and [the WIV] related to terms of agreements, bat coronaviruses, genome or genetic sequencing, SARS-CoV-2, and/or laboratory safety practices" pursuant to key NIH research funding through EcoHealth to the Wuhan lab as a grant sub-recipient.
Yet Daszak himself has not cooperated with the request. An aide with the Energy and Commerce Committee confirmed to Just the News this week that the committee has "received no response still from EcoHealth Alliance and Peter Daszak to the April 16th letter from Leaders Rodgers, Guthrie, and Griffith." -JTN
"We have asked Daszak to provide information we know he has that sheds light on the origins of this pandemic," said GOP Rep. Cathy McMorris Rodgers, who has also publicly noted Daszak's refusal to play ball.
"Dr. Daszak, you received American funds you used to conduct research on bat coronaviruses at the Wuhan Institute of Virology," Rodgers continued during a House subcommittee meeting last week. "You owe it to the American people to be transparent."
Meanwhile, Congressional Democrats aren't actually interested in getting to the bottom of things - as they themselves hold subpoena power in both chambers. The ultimate authority, as JTN notes, rests with that party - specifically Energy and Commerce Committee Chairman Frank Pallone - who notably boosted funding to Fauci's NIH in 2015 to the tune of $2 billion per year through 2020.
Rep. Frank Pallone (D-NJ)
Why a subpoena hasn't been issued in more than two months is unclear, but we could venture a guess...
The UK’s Joint Committee on Vaccination and Immunisation (JCVI) has recommended that the NHS should start a COVID-19 booster shot programme in September, to run alongside the annual flu vaccine drive.
The programme should run in two stages, initially targeting elderly and vulnerable people and frontline health and social care workers like the initial vaccination push, and then be expanded to include all adults aged 50 and over, plus younger, at-risk people who qualify for a flu shot.
While not yet formally adopted by the government, the proposals would mean that millions of people – perhaps as many as 30 million – could be in line for a third dose in the autumn.
The recommendation comes as the UK is anticipating a more severe flu season than usual, which could place added pressure on the NHS if protection against COVID-19 afforded by the initial two-dose vaccinations starts to wane.
There’s no evidence that will happen, and just this week AstraZeneca reported results suggesting that a single shot of its Vaxzevria vaccine induced immunity for at least one year. The JCVI’s recommendation is a precaution while the UK waits for the results of its large-scale COV-BOOST trial in September.
A large-scale booster rollout will help to ensure that the protection already built up in the population does not decline through the winter months, and that additional protection is layered in to guard against any problem variants of SARS-CoV-2 that may emerge.
No decisions have yet been made on which vaccines will be used, but the COV-BOOST should provide important data on that front as it is including seven types – from AstraZeneca, Pfizer/BioNTech, Moderna, Novavax, Valneva, CureVac and Janssen.
With the UK now heading for a possible ending of social restrictions on 19 July, the country “is now heavily dependent on the continued success of the vaccination programme,” said England’s deputy chief medical officer Professor Jonathan Van-Tam.
“We want to be on the front foot for COVID-19 booster vaccination to keep the probability of loss of vaccine protection, due to waning immunity or variants, as low as possible – especially over the coming autumn and winter,” he added.
The latest estimates from Public Health England (PHE) suggest that vaccines deployed so far have already had an impact on hospitalisation rates, and prevented an estimated 7.2 million infections and 27,000 deaths in England alone.
Wales and Scotland’s devolved health administrations are also working on delivering booster shot campaigns in the autumn, according to a BBC report.
Armed with new data from its development partner Bharat Biotech, Ocugen is planning to press ahead with plans to file for approval of their COVID-19 vaccine Covaxin in the US and Canada.
Covaxin has already been approved for restricted emergency use in India, getting the green light in January months before the final results from the trial were available.
That data from the 25,800-patient phase 3 trial is now in, and suggested the shot has an overall protective efficacy of 77.8%, and 65.2% against the highly transmissible delta (B.1.617.2) variant of SARS-CoV-2 which is troubling health systems around the world.
Covaxin – a two-dose shot based on an inactivated form of the virus formulated with an immune-boosting adjuvant – is also 93.4% protective against severe symptomatic COVID-19, according to a preprint posted on the MedRxiv website, where studies can be published before being peer reviewed.
Bharat said in a statement that Covaxin is the first COVID-19 vaccine to report promising efficacy against asymptomatic infections based on PCR testing, adding that “will help in reducing disease transmission.”
According to Balram Bhargava, the director general of Indian Council of Medical Research (ICMR) which co-developed the vaccine, Covaxin “will not only benefit the Indian citizens but would also immensely contribute to protect the global community against the deadly SARS-CoV-2 virus.”
Ocugen licensed rights to Covaxin in the US and Canada earlier this year in twin deals that give it a 45% share of profits made from sales in the two countries.
Shares in the Philadelphia-based biotech fell after it said it would go after a full marketing application for Covaxin rather than emergency use authorisation, although the FDA had already said it had closed the door on the EUA route with multiple COVID-19 vaccines now available.
The data against delta is particularly encouraging as the variant is becoming dominant in the US, and President Biden has warned that the strain – coupled with low vaccination rates in some areas of the country – means that the pandemic is has yet to be “vanquished.”
The number of people choosing to remain unvaccinated has contributed to the Biden administration missing its goal of 70% of US adults receiving at least one shot of vaccine by the Fourth of July holiday.
There was more good news on the delta variant front last week when Johnson & Johnson announced that its single-shot vaccine generated “strong and persistent activity” against delta and other prevalent SARS-CoV-2 variants in a study of blood samples taken from its phase 3 trial.



{kind=link}