By Mish Shedlock of Mishtalk
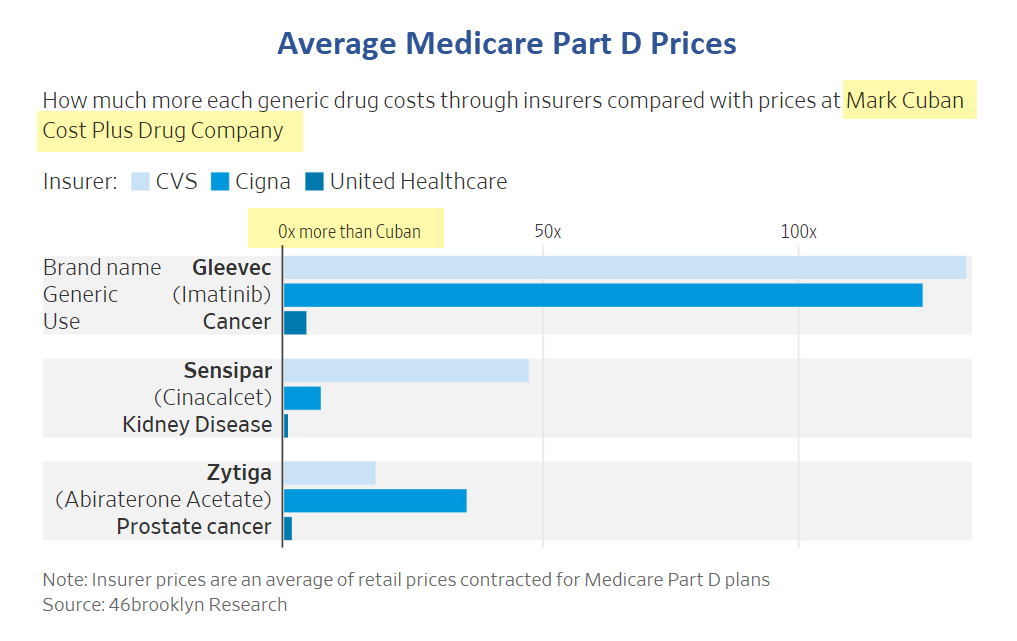
Health insurers dramatically mark up prices of generics and pharmacies are in on the scheme.
By Mish Shedlock of Mishtalk
Health insurers dramatically mark up prices of generics and pharmacies are in on the scheme.
by Simon White, Bloomberg macro strategist,
The top half of the highest-earning US households have increased their ownership in financial assets to near all-time highs, leaving them ever more exposed to rising inflation. Bonds and especially stocks are thus acutely vulnerable to a re-acceleration in price growth.
Ronald Reagan called inflation as violent as a mugger, as frightening as an armed robber and as deadly as a hitman.
During a recent flight through a Texas international airport, my experience at its airport security checkpoint exposed a major problem with the Transportation Security Administration (TSA) operations.
When I passed through the PreCheck lane, the line was backed up so that the TSA Officers (TSOs) could not authenticate passenger IDs in a timely manner. The bottleneck was caused by the computed tomography (CT) screening device that was used to screen passenger carry-on bags. The time used to screen such bags was so excessive that the line was grinding to a near stop.
Unfortunately, the situation was worse than first imagined.
Once passing through the magnetometer, the majority of carry-on bags were being pulled aside for secondary (additional) screening. A small sample of carry-on bags that I observed put the percentage selected for secondary screening at around 60 percent.
The likelihood that such a high percentage of bags contained a prohibited item is so small that the problem was either the image that the CT screening device was projecting, or the TSO’s skill set being inadequate to make informed real-time decisions to pull the bag for secondary screening.
The TSA has spent more than $2 billion for these new screening devices. However, there are additional costs of using CT devices for carry-on bags, independent of the direct costs to purchase and maintain them.
The most obvious is that it is slowing checkpoint passenger flow to a point as to congest checkpoints. Any time people congregate in large numbers on the nonsterile side of checkpoints, security risks are elevated.
The secondary screening is also requiring TSOs to resolve every such bag, which most certainly were false alarms. Yet false alarms are expensive. Most importantly, they distract TSOs from what could be more critical risks that may be less obvious to detect.
To justify all such costs requires benefits beyond what the previous X-ray devices provided.
The CT screening devices were justified because they could obtain three-dimensional images of carry-on bags, an improvement over the two-dimensional images provided by X-ray devices. But enhanced functionality alone is insufficient to justify a new technology. The functionality must produce improved performance, as measured by enhanced efficiency or stronger security, or both.
The CT screening devices permit travelers to leave more belongings in their carry-on bags. For those undergoing enhanced screening through standard security lanes, this means less time unpacking their bags. However, if the CT screening devices are slower in processing carry-on bags so that passengers are congregating in the screening area, any such benefits are certainly diminished, and perhaps even completely evaporate.
The situation gets even worse in PreCheck lanes. PreCheck passengers do not need to remove belongings from their carry-on bags. So by adding CT screening devices to these lanes, the TSA has added an unnecessary technology enhancement that does not improve security, while slowing down the processing of passengers, making them less efficient.
The one advantage of CT screening devices is that they can better assess liquids for explosives. As a result, some airports in the UK have relaxed the 100 milliliter liquid requirement.
Explosives pose the biggest threat to the air system. Other prohibited items, like knives and firearms, may cause damage and even result in lives lost. However, such prohibited items pose little risk to destroy an airplane in flight, much like what was experienced on 9/11.
It is reasonable to expect that the relaxation of the 3-1-1 liquid ban is on the TSA’s agenda. The first group that should be eligible to bring larger liquid and gel containers (beyond 3 ounces) are PreCheck vetted passengers. The only benefit that justifies the expense of CT screening devices in PreCheck lanes is that they will be the first group permitted to bring full size tubes of toothpaste, 10-ounce bottles of shampoo and sun block and half-liter bottles of water through security.
Given that there is an autumn lull in air travel until the holiday season, this is the time to sort out the use of CT screening devices. A short-term fix is that every airport with CT screening devices can train a dedicated group of TSOs to man such devices. This will reduce the number of bags that require secondary screening, easing the burden on all TSOs and improving the flow of passengers through checkpoints.
Given the surge in passenger volume during the holiday season, any adjustments that can improve passenger flow while maintaining air system security is a win for all stakeholders. It is conceivable that on some day before the end of 2023, the TSA will screen more than 3 million passengers. Preparing for such extreme numbers is critical to reduce bottlenecks that serve no one’s interests.
The TSA is committed to CT screening devices. They are also committed to biometrics using facial recognition technology to authenticate passenger identity. The former is more accepting by the public, yet provides limited security benefits (unless they impact the liquid limitations). The latter draws suspicion by some, while it provides significant security benefits.
If the TSA wants to maintain and enhance its reputation among the traveling public, it must provide a secure and efficient checkpoint process. Rethinking how CT screening devices are being deployed and used is critical.
Sheldon H. Jacobson, Ph.D., is a professor of Computer Science at the University of Illinois at Urbana-Champaign. He applies his expertise in data-driven risk-based decision-making to evaluate and inform public policy. He has studied aviation security for over 25 years, providing the technical foundations for risk-based security that informed the design of TSA PreCheck.
https://thehill.com/opinion/technology/4200323-the-tsa-has-a-problem/
Alnylam stock tumbled Thursday after a split advisory panel recommended that the Food and Drug Administration approve its heart disease treatment.
The FDA's Cardiovascular and Renal Drugs Advisory Committee voted 9 to 3, saying the benefits of Alnylam Pharmaceuticals' (ALNY) drug, Onpattro, outweigh the risks for patients with transthyretin amyloid cardiomyopathy. In this condition, abnormal plaque called amyloid builds up on the heart. This can lead to heart failure.
But panelists suggested Onpattro would only be useful for patients who worsen while receiving Pfizer's (PFE) tafamidis, which sells as Vyndaqel and Vyndamax. Patients treated with Onpattro showed improvements in symptoms. But Pfizer's drug has a proven benefit on mortality.
RBC Capital Markets analyst Luca Issi remained upbeat, despite the tumble for Alnylam stock.
"The vote is nonbinding, but we think approval on Oct. 8 is likely at this point," he said in a note.
Guggenheim Partners downgraded 2seventy Bio Inc
to Neutral from Buy and removed the price target.
On Tuesday, 2seventy Bio announced restructuring its business operations and research and development model to reduce costs.
Approximately 40% workforce reduction combined with related actions expected to achieve over $130 million in savings in 2024-2025, with a projected cash runway into at least 2026.
CEO Nick Leschly announces plans to step down and transition to Chairman of the Board of Directors.
Based on an anticipated decline in Abecma sales in Q3, U.S. revenue for full-year 2023 for Abecma could be lower than the previously projected $470-$570 million range.
Although TSVT has reaffirmed expectations that the Abecma joint venture will generate positive cash flow this year and the next, Guggenheim writes that the visibility into immediate upward potential is constrained.
This limitation stems from a recent manufacturing pause for maintenance and the escalating competition from other BCMA-targeted agents, as indicated by management's remarks.
Simultaneously, substantial operating expenses persist, heightening the risk of potential future dilutive financing activities without significant pipeline catalysts. TSVT remains committed to supporting Phase I studies for bbT369 and SC-DARIC33, along with programs concentrating on solid tumors (MAGE-A4, MUC-16, and a newly revealed program in partnership with JW Therapeutics. Updates on these initiatives are anticipated in 2024-25.
The psychedelic drug MDMA, also known as ecstasy or molly, has passed another key hurdle on its way to regulatory approval as a treatment for mental illness. A second large clinical trial has found that the drug — in combination with psychotherapy — is effective at treating post-traumatic stress disorder (PTSD). The results allow the trial’s sponsor to now seek approval from the US Food and Drug Administration (FDA) for MDMA’s use as a PTSD treatment for the general public, which might come as soon as next year.
“It’s an important study,” says Matthias Liechti, a psychopharmacologist who studies MDMA at the University of Basel in Switzerland, but who was not involved with the trial or its sponsor. “It confirms MDMA works.”
In June, Australia became the first country to allow physicians to prescribe MDMA for treating psychiatric conditions. MDMA is illegal in the United States and other countries because of the potential for its misuse. But the Multidisciplinary Association for Psychedelic Studies (MAPS), a non-profit organization in San Jose, California, has long been developing a proprietary protocol for using MDMA as a treatment for PTSD and other disorders. MAPS has been campaigning for its legalization — a move that could encourage other countries to follow suit.
In 2021, researchers sponsored by MAPS reported the results of a study1 in which 90 people received a form of psychotherapy developed by the organization alongside either MDMA or a placebo. After three treatment sessions, 67% of those who received MDMA with therapy no longer qualified for a PTSD diagnosis, compared with 32% of those who received therapy and a placebo.
The results were widely hailed as promising, but the FDA typically requires two placebo-controlled trials before a drug can be approved. The results of a second trial, involving 104 further individuals with PTSD and published on 14 September in Nature Medicine2, were similar to those of the original: 71% of people who received MDMA alongside therapy lost their PTSD diagnosis, compared with 48% of those who received a placebo and therapy. The drug seemed to work just as well in people who had other mental illnesses, such as depression, and in those who’d had PTSD for a long time. It also seemed to work equally well across racial and ethnic groups.
Jennifer Mitchell, a neurologist at the University of California, San Francisco, who led both studies, says that one of the most promising things about the latest trial is the low drop-out rate: only 9% of participants left the study. Most were individuals who received the placebo, and thus were more likely to continue having symptoms. By contrast, a recent study3 comparing psychotherapies in veterans with PTSD reported drop-out rates of up to 56% for prolonged exposure therapy, a commonly used approach in which patients undertake the difficult task of addressing the traumatic event that triggered their condition.
MDMA doesn’t make the therapy process more “fun”, Mitchell says, but the drug seems to induce self-compassion in a way that other therapies don’t. She calls it “a communication lubricant” that helps people to recall traumatizing events and talk to their therapists without experiencing shame or horror.

During MAPS trial sessions, people are given MDMA doses alongside psychotherapy.Credit: Multidisciplinary Association for Psychedelic Studies (MAPS)
“It’s nice to see it could be replicated,” Liechti says. Although the trials are small, he says, the immense improvement in symptoms makes the results statistically significant. But he adds that questions remain as to whether some people will need more than three treatment sessions, and whether the effects will last long-term.
A MAPS spokesperson says that the organization plans to seek formal FDA approval before the end of this year, and that because the agency has already designated MDMA as a ‘breakthrough therapy’ — a category for treatments that address serious or life-threatening conditions — it will be evaluated quickly. If approved, MDMA will no longer be strictly illegal in the United States, and researchers will be able to seek federal funding to pursue larger clinical trials of the drug and ask additional questions. Mitchell wants to study why some people don’t respond to MDMA, and whether taking it in certain contexts or alongside different types of therapy improves its effect.
Vaile Wright, senior director of health-care innovation at the American Psychological Association (APA) in Washington DC, says that the scale of the improvement in the MAPS trials is significant for a PTSD treatment. But she notes that MDMA is unlikely to be the solution for everyone. “I see this as one solution to a very complicated problem that needs multiple solutions,” she says. The APA has urged caution around the drugs, stating last year that there was a “lack of adequate scientific evidence to endorse the use of psychedelics” outside controlled trials.
Erick Turner, a psychiatrist at Oregon Health & Science University in Portland, says that the difference between the MDMA and placebo groups is impressive, but doubts that it is as big as it seems. Because MDMA produces an intense psychedelic experience, around 94% of people who received the drug and 75% of those who didn’t correctly guessed which group they were in. “That is not a blinded study,” Turner says.
‘Blinding’ participants and providers to who is getting the drug is particularly important in psychiatry trials, because people tend to feel better if they think they are taking an active drug. Responding to this criticism, Mitchell says that this happens with many drugs that work extremely well — people correctly guess which trial group they’re in because their symptoms are gone.
But even if MDMA is safe, Turner says, it doesn’t meet the FDA’s usual criteria for a well-controlled study. To partially address the placebo concern, the FDA approved a special protocol that MAPS used in this study: an independent evaluator who was not involved in the treatment session and who didn’t know whether a participant had received the drug. The evaluator examined each person before and after treatment to assess their improvement.
The FDA still has to work out how it will regulate the drug, given that MAPS has said MDMA should only be given in the context of therapy, both for efficacy and safety reasons. Mitchell says she worries about people trying MDMA on their own: it could be harmful to people with heart conditions, for instance. And it hasn’t been tested in people with a family history of schizophrenia, which could be triggered by the drug. If people have bad reactions to taking the drug when they are not in a controlled environment, she says, MDMA might regain the harmful reputation that led to it being banned in the first place.
doi: https://doi.org/10.1038/d41586-023-02886-x
Taldefgrobep alfa is the only myostatin inhibitor in clinical development that targets both myostatin and activin A signaling, two key regulators of muscle mass and adipose tissue
- RESILIENT, the pivotal clinical trial in spinal muscular atrophy, was designed to test the efficacy and safety of taldefgrobep alfa as adjunctive therapy to increase muscle in SMA patients treated with standard of care nusinersen, risdiplam or onasemnogene abeparvovec-xioi
https://finance.yahoo.com/news/biohaven-completes-enrollment-pivotal-phase-110000712.html