This paper describes and explains the function of Pharmacy Benefit Managers (PBMs) in the American health care economy. PBMs are private businesses that developed in the free market to manage prescription drug benefits for health insurance plan sponsors.
Nearly all Americans have private or government prescription drug insurance coverage that is managed by PBMs. PBMs enhance competition through group purchasing and negotiated discounts that provide substantial economic and health benefits for consumers and taxpayers.
Multiple legislative proposals are pending that would restrict PBM functioning by limiting or eliminating rebates and discounts that pass through PBMs and by requiring PBMs to disclose pricing and other confidential terms of their contracting. But the legislation is likely to be counterproductive, resulting in reduced competition, higher costs, and an end to the natural evolution in the market of terms and arrangements which benefit the actors in the drug distribution system.
Contents 1 Executive summary 1 Introduction 2 PBMs in the prescription drugs market 5 How PBMs create value 7 Counterproductive proposals to restrict PBMs 8 Targeting rebates and discounts 10 Transparency and reporting requirements 11 Conclusion
...
Conclusion
PBMs are a pro-competitive creation of the market for prescription drugs that improve consumer welfare. They lower costs for drug insurance plan sponsors and their patient-customers through group purchasing and negotiations on a variety of contract terms leading to lower drug prices, better drug utilization, and improved health. The fact that PBMs have flourished in a free market confirms that they add value for participants in the prescription drug distribution system.
The prescription drug distribution market is not perfect. But the various legislative proposals to restrict PBMs are more likely to make it worse than better. Congress should not enact them. There are signs that new entrants could disrupt the current market, further improving consumer welfare. The market for prescription drugs should be allowed to continue to evolve and become more efficient through negotiations among the market actors.
Joel M. Zinberg, M.D., J.D. is a senior fellow with the Competitive Enterprise Institute, and the Director of the Public Health and American Well-Being Initiative at Paragon Health Institute. He is a native New Yorker who recently completed two years as General Counsel and Senior Economist at the Council of Economic Advisers in the Executive Office of the President. He practiced general and oncologic surgery in New York for nearly 30 years at the Mount Sinai Hospital and Icahn School of Medicine where he is an Associate Clinical Professor of Surgery. He has been involved with health policy issues and the interaction between law and medicine for his entire career. Dr. Zinberg taught for 10 years at the Columbia University Law School as a Lecturer in Law where he created a course on the legal, policy and ethical issues surrounding organ transplantation. He served for many years on the New York State Board of Professional Medical Conduct and on Mount Sinai’s Ethics Committee and Institutional Review Board. He is past President and Trustee of the New York County Medical Society. Between 2015 and 2017 he was a Visiting Scholar at the American Enterprise Institute.
The House Oversight Select Subcommittee on the Coronavirus Pandemic has been investigating the numerous outstanding questions regarding the origins of the COVID-19 virus, the government’s response to it, the impact of US dollars that were illegally beingfunneledfrom the National Institutes of Health (NIH) to the Wuhan lab, and the cover-up campaign that appears to have been undertaken by multiple people within the government and scientific communities.
This week, the committee wrote letters to CIA Director William Burns and former CIA Chief Operating Officer Andrew Makridis detailing whistleblower testimony it has received claiming the CIA paid monetary incentives to six agents on its Covid Discovery Team to change their position on the lab leak hypothesis.
The whistleblower’s identity is being protected, but they are reportedly a “multi-decade, senior-level, current Agency officer.” According to their testimony, the analysts believed the coronavirus originated in the Wuhan lab, a theory many on the Left tried to downplay as a ‘conspiracy theory’ and others within the government went to lengths to censor on social media.
The reasons for this seem pretty obvious. Fauci and the NIH had illegally been funding gain-of-function research in the Wuhan lab via a passthrough “nonprofit” called EcoHealth Alliance for some time. If the virus did originate in that lab, it’s highly possible its creation was funded by Fauci via our tax dollars—hence their apparently desperate need for it to have not originated there.
We know all this, and have known it since the spring of 2020 thanks to Freedom of Information Acts (FOIAs) filed by the White Coat Waste Project (where I am a Fellow), which had been investigating taxpayer funded gain-of-function research long before COVID-19 as it involves animal torture.
The agents were paid to instead say they believed the virus jumped from animals to humans, the popular narrative being pushed by “experts” and the government throughout most of 2020 and 2021.
The letter to Director Burns reads, “According to the whistleblower, the Agency assigned seven officers to a COVID Discovery Team (Team). The Team consisted of multi-disciplinary and experienced officers with significant scientific expertise. According to the whistleblower, at the end of its review, six of the seven members of the Team believed the intelligence and science were sufficient to make a low confidence assessment that COVID-19 originated from a laboratory in Wuhan, China.”
It continues, “The whistleblower further contends that to come to the eventual public determination of uncertainty, the other six members were given a significant monetary incentive to change their position.”
Burns has until Sept. 26, 2023 to respond to the subcommittee’s request, which includes all documents and communications related to the Covid Team and the origins of the coronavirus, including its correspondence with relevant federal agencies and the Team’s pay history. Makridis of the CIA is also being asked to participate in a transcribed interview later this month due to the role he played in forming the COVID Team.
This is just the latest finding among many on the ways the US government appears to have worked in lockstep to keep the American public in the dark about what was happening to them and the role their government may have played in it all along—using their own tax dollars against them.
Earlier this summer, the committee published a report accusing Dr. Fauci of orchestrating a campaign to cover up the lab leak theory.
Meanwhile, emails show some of the most popular names behind the infamous “experts” of 2020 (namely scientist Kristian Andersen and colleagues he worked with to produce the now largely discredited ‘Proximal Origins’ report) manipulating the New York Times to achieve reporting on the origins they desired.
In February of 2020, Andersen wrote, “Accidental escape is in fact highly likely—it’s not some fringe theory,” but he then quickly changed his tune—drafting Proximal Origins with the heavy influence of Dr. Fauci. Documents have since revealed Andersen had an $8.9 million grant request sitting on the desk of the NIH at the time.
“At the CIA we are committed to the highest standards of analytic rigor, integrity, and objectivity. We do not pay analysts to reach specific conclusions,” CIA Director of Public Affairs Tammy Kupperman Thorp told the New York Post in a statement. “We take these allegations extremely seriously and are looking into them. We will keep our Congressional oversight committees appropriately informed.”
The FBI and the Department of Energy have reached separate conclusions that the virus likely originated in the Wuhan lab. Former Director of National Intelligence John Ratcliffe told Congress that the so-called ‘lab leak theory’ was the ‘only’ credible explanation for the pandemic.
“My informed assessment as a person with as much access as anyone to our government’s intelligence … has been and continues to be that a lab leak is the only explanation credibly supported by our intelligence, by science and by common sense,” Ratcliffe told the special committee in a hearing. He continued, “If our intelligence and evidence supporting a lab leak was placed side by side with our intelligence and evidence pointing to a natural origins or spillover theory, the lab leak side of the ledger would be long, convincing, even overwhelming — while the spillover side would be nearly empty and tenuous.”
As for the CIA they say they, “remain unable to determine the precise origin of the COVID-19 pandemic, as both hypotheses rely on significant assumptions or face challenges with conflicting reporting.”
Hannah Cox is a Fellow at the White Coat Waste Project, a free market animal welfare seeking to end taxpayer-funded animal torture.
The Biden administration’s weak and ineffective border actions allow cartels to freely smuggle fentanyl across our southern border. And while you’d think the administration wouldn’t want to make it any easier for the cartels to enrich themselves, that’s exactly what could happen if Biden’s Food and Drug Administration (FDA) moves forward with its plan to ban all menthol cigarettes. The administration must stop this misguided effort.
This month, the FDA committed to banning the sale of menthol cigarettes, a third of all cigarettes sold and a $30 billion category in the US with millions of adult consumers. Banning menthol cigarettes will create a void in the market that cartels will rapidly exploit. Criminal cartels have always changed what they supply to the American public based on demand. From marijuana to cocaine, methamphetamine to fentanyl, there is no reason to think menthol cigarettes will not be the next revenue stream for cartels.
It’s well known that illicit tobacco sales already fund terrorism. Hezbollah expanded beyond drugs and into illicit tobacco due to the high profit and low risk. Hamas has also used illicit tobacco smuggling in the U.S. to fund terrorism. In 2013, authorities in New York took down a massive eastern seaboard cigarette trafficking enterprise known as “Operation Tobacco Road” with many members linked to Hamas.
Since at least 2018, The Jalisco New Generation Cartel, a cartel sanctioned by the United States for its role in trafficking narcotics and fentanyl into the U.S., has been involved in the sale of tobacco products to generate a new revenue stream. The $30 billion U.S. market for menthol cigarettes would be a tempting opportunity.
Recently, five U.S. Senators wrote Treasury Department Secretary Yellen requesting sanctions on Mexican Tobacco Cartel companies, such as Tobacco International Holdings Switzerland SA (TIH), and specific individuals known to be or suspected of having ties with The Jalisco New Generation Cartel. They’re asking the U.S. Treasury department to take immediate steps to close off illicit tobacco as the new source of funding for the cartels that continue to ship fentanyl into the US. This is a good start, but more needs to be done.
Most troubling, FDA hasn’t even considered the gift a menthol ban would be to cartels. When asked about this at a recent hearing, FDA Commissioner Califf said, “I'm not aware of any study of tobacco cartels in -- in Mexico.”
FDA is already struggling to prevent a thriving illicit market for tobacco products in the U.S. Manufacturers operating under the China State Tobacco Monopoly are flooding the U.S. market with thousands of illegal e-vapor products. These products represent nearly half of the e-vapor market today, according to estimates. They come in highly flavored options and routinely top the list of products used by kids. FDA’s response to this? The Agency said slow enforcement is attributed to the fact that FDA “cannot be everywhere at all times.”
President Biden’s failed border policies have made the cartels more powerful than ever. At a time when we should be cutting off revenue sources for the cartels, another bad policy decision by this Administration will only make them richer and fuel both the humanitarian and fentanyl crisis on our border.
Rather than rushing into creating a void that the cartels can exploit, it would be prudent for the Biden administration to study the real-world impact of its prohibitionist policies. While encouraging fewer people to smoke is a worthy goal, it shouldn’t come at the expense of our national security or by enriching drug cartels.
Jobe Dickinson is the President of the Border Security Alliance and a retired law enforcement officer.
On Tuesday, the Biden Administration’s Center for Medicare and Medicaid Services (CMS) will announce which ten drugs will be subject to new price caps. While this will be welcome news to Medicare patients, it’s a gut punch for Americans suffering from Alzheimer’s. In Maine, the state with the oldest population in the nation, the impact of Medicare drug price controls will be felt for decades.
Most of the profits that pharmaceutical companies reinvest into developing cures for diseases like Alzheimer’s come from drugs covered by Medicare. Patients on Medicare make up the highest users of prescription drugs. That means that drug makers cannot realistically make a profit without providing products through Medicare. For companies employing researchers to test potential treatments for Alzheimer’s, price caps mean less funding for product development.
Companies like Eli Lilly and AstraZeneca are scrambling to reorganize their research and development (R&D) plans and deprioritize the development of different drugs to account for lost revenue. Both of these companies are developing new drugs to treat Alzheimer’s, and the cost of those developments are currently reflected in the drug prices through Medicare. With enough profit to invest in R&D, companies could expand product options, potentially lowering costs of today’s medications in the future. Price controls ensure that won’t happen and postpone drug development for Alzheimer’s patients across the nation.
Alzheimer's impacts 6 million Americans and is the seventh-leading cause of death in the United States. There are currently only two FDA-approved drugs on the market now that can treat it: Leqembi, which costs $26,500 for a year of treatment out of pocket, and Aduhelm, which costs $28,200. It’s small wonder that few drugs can accomplish what they can: Effective medication must deliver the drug to the human brain’s separate blood supply and regulate the buildup of plaques. Multiple companies like Pfizer and Johnson & Johnson have sunk millions into Alzheimer’s research, only to come up empty-handed. A single Alzheimer's drug developed by both companies that scrapped in 2012 cost them a combined $300-400 million dollars.
More funding is needed to develop better, cheaper, and more accessible drugs to treat Alzheimer’s. But when pharmaceutical companies are not able to make money off the drug their researchers’ spent years and millions creating, the incentive to develop new, cheaper drugs for complex diseases like Alzheimer’s is devastated.
The drugs being developed to treat and cure Alzheimer’s, Eli Lilly’s lecanemab and AstraZeneca’s saracatinib need more research before hitting the shelves, and that means more investment. Most attempts to bring a drug to market end in failure as they must undergo multiple test trials, get approved by the FDA, and account for any side-effects that may make the drug more of a risk to take than the disease it treats. AstraZeneca’s saracatinib was originally developed to treat cancer, but was discontinued in tests due to lack of efficacy. Now, AstraZeneca is considering delaying launches of some cancer drugs as it tries to adapt its R&D spending to these new price controls. That could mean AstraZeneca’s Alzheimer’s drugs are not within reach of U.S. patients.
Americans having access to only two FDA-approved Alzheimer’s drugs will likely remain the status quo. Pharmaceutical sales correlate with research and development (R&D). In 2018 alone, if price controls in 32 OECD were lifted, $56.4 billion more dollars would have been invested into pharmaceutical R&D. Since then, multiple companies like Pfizer, Roche, and Eli Lilly have abandoned several drugs that may have cost more than $2 billion dollars each. Existing price controls in other countries already limit pharmaceutical companies’ ability to reinvest profits into further R&D. By instituting extensive price controls on commonly-used drugs, the U.S. will reduce the manufacturing of new drugs by almost 40% in the long run, with complex diseases like Alzheimer’s being left on the table first.
Capping prices treats the symptom of medical costs, not the disease. Maine has a total of geriatricians as of 2021 and needs to increase the trained caregiver workforce by 8% to meet the demand for Alzheimer’s care. The need to develop more effective and affordable medicine to combat this disease cannot be ignored. By capping prices, the Biden Administration is cutting short the industry’s search for a cure.
Medicare’s recent announcement of the ten prescription medications that will be subject to government price controls, under the provisions of the Inflation Reduction Act, provides an opportune juncture for policymakers in Congress and the executive branch. Before moving forward with the price controls on these drugs that would go into effect in 2026, there is one very important question they should be asking.
What do America’s seniors, the people ostensibly being helped by this radical change in the drug pricing infrastructure, really want?
The Medicare Today coalition asked that question in the form of a Morning Consult survey of 1,000 65-and-older Medicare beneficiaries, and it was abundantly clear that there is an enormous chasm between the policies the government thinks seniors should have and what older Americans actually prefer.
The Inflation Reduction Act’s drug pricing provisions set out to fix a Medicare Part D prescription drug program that seniors, in huge numbers, believe is not the least bit broken. Our survey showed that 91 percent of the senior population is satisfied with their Medicare prescription drug coverage. They also aren’t experiencing any affordability challenges, with 86 percent saying their monthly premiums are affordable and that their Part D plan offers good value. Eight out of every 10 seniors say their out-of-pocket costs are reasonable. And 81 percent reported that their plan covers all of the medicines they need.
One has to question the sense of urgency that led to the first-time-ever imposition of government price controls in the Medicare Part D program. (Yes, these are called “negotiations,” but when companies have the threat of a 95 percent excise tax hanging over their heads if they don’t cooperate, it’s clear the government will be dictating the terms.) Seniors say they aren’t feeling a financial pinch when they pick up their medicines at the pharmacy, and Part D monthly premiums aren’t exactly spiraling upward in cost. In fact, the Centers for Medicare and Medicaid Services announced in July that average premiums are expected to decrease by almost two percent in 2024.
Naturally, seniors have been following this issue as it has unfolded, and they have made it clear in the Morning Consult survey that their wishes are not in alignment with what Congress and the administration want to do to their drug benefit. Two of every three seniors say they would prefer to maintain the status quo in which private Part D plans negotiate prices with biopharmaceutical manufacturers, and only 16 percent say they want the government to set prices and determine which drugs are covered.
Over 80 percent, in fact, said they are concerned that, under this new paradigm, the government could choose to restrict access to medicines that seniors and Medicare beneficiaries with disabilities currently use, and 79 percent said they fear these price controls will limit access to newer prescription drugs.
As the Inflation Reduction Act was written, there was an implicit tradeoff. Yes, price controls would have an adverse effect on biopharmaceutical innovation, as we’ve already seen with companies pulling drugs out of the clinical trial process because price controls will make it difficult to gain a return on the massive investment required to bring them to market, in exchange for improved drug affordability for seniors.
Seniors are saying overwhelmingly, though, that this is a quid pro quo they don’t want. There is still time for lawmakers to correct this course and pursue alternative policies that boost competition and lower prices without utilizing heavy-handed price controls and the negative consequences that come with them. The first step must involve listening to the millions of Americans who will be directly affected.
Mary R. Grealy is president of the Healthcare Leadership Council and chair of the Medicare Today coalition.
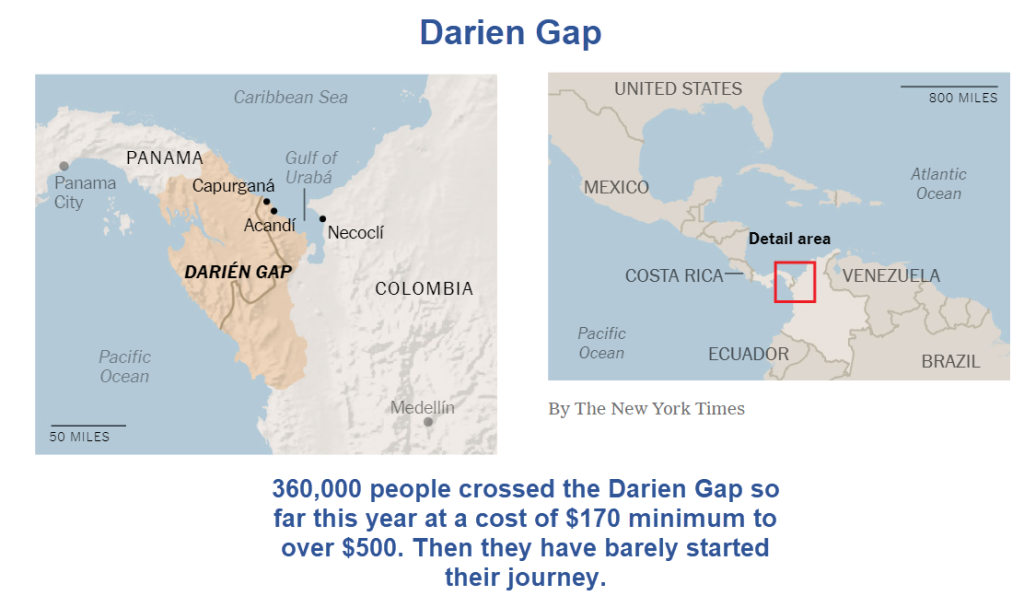
Biden vowed to “end the illicit movement” of people through the Darién jungle in Colombia. But the profits are too big to pass up. A record 360,000 made passage this year. That’s well above the record 250,000 for all of 2022.
Politicians and other human traffic smugglers in Colombia charge a minimum of $170 a head, not to reach the US, but simply to get through the Colombian jungle on route to Panama. And that’s just for a guide. The all inclusive package is $500 or more.
The Math
$170 * 360,000 = $61,200,000
$500 * 360,000 = $180,000,000
The Colombian politicians and helpers have made somewhere between $61 million and $180 million this year selling services that the Biden administration vowed to end.
This story is not from radical rightwing newsletters, it’s from the New York Times. I have a free link below.
‘A Ticket to Disney’? Politicians Charge Millions to Send Migrants to U.S.
“We have organized everything: the boatmen, the guides, the bag carriers,” said Darwin García, an elected community board member and former town councilman in Acandí, a Colombian municipality at the entrance to the jungle.
Now, Mr. García’s younger brother, Luis Fernando Martínez, the head of a local tourism association, is a leading candidate for mayor of Acandí — defending the migration business as the only profitable industry in a place that “didn’t have a defined economy before.”
More than 360,000 people have already crossed the jungle in 2023, according to the Panamanian government, surpassing last year’s almost unthinkable record of nearly 250,000.
“This is a beautiful economy,” said Fredy Marín, a former town councilman in the neighboring municipality of Necoclí who manages a boat company that ferries migrants on their way to the United States. He says he transports thousands of people a month, charging them $40 a head.
the business is run by elected community board members like Mr. García, through a registered nonprofit started by the board’s president and his family. It’s called the New Light Darién Foundation, and it manages the entire route from Acandí to the border with Panama — setting prices for the journey, collecting fees and running sprawling campsites in the middle of the jungle.
The foundation has hired more than 2,000 local guides and backpack carriers, organized in teams with numbered T-shirts of varying colors — lime green, butter yellow, sky blue — like members of an amateur soccer league.
Migrants pay for tiers of what the foundation calls “services,” including the basic $170 guide and security package to the border. Then a migration “adviser” wraps two bracelets around their wrists as proof of payment.
“Like a ticket to Disney,” said Renny Montilla, 25, a construction worker from Venezuela.
Hanging over the entire business is a large and powerful drug-trafficking group called the Gaitanist Self-Defense Forces, sometimes known as the Gulf Clan. Its control over this part of northern Colombia is so complete that the country’s ombudsman’s office calls the group the region’s “hegemonic” armed actor.
The New Light Darién Foundation is helping to turn that natural barrier into something much more passable, with restaurants, camps, porters and guides.
Once Through Darien, Then What?
There is much more to the article. Importantly, once through the Darien Gap, everyone is on their own.
“On the Panamanian side, small criminal bands rove the forest, using rape as a tool to extract money and punish those who cannot pay,” notes the New York Times.
People need to cough up more money to make it through Panama to Mexico, then from Mexico to the US border, then still more money from the US border to the US.
People without adequate funds are subject to rape or torture or death.
What if I told you one in 50 people who took a new medication had a “medically attended adverse event” and the manufacturer refused to disclose what exactly the complication was — would you take it?
And what if the theoretical benefit was only transient, lasting about three months, after which your susceptibility goes back to baseline?
And what if we told you the Food and Drug Administration cleared it without any human-outcomes data and European regulators are not universally recommending it as the Centers for Disease Control and Prevention is?
That’s what we know about the new COVID vaccine the Biden administration is firmly recommending for every American 6 months old and up.
The push is so hard that former White House COVID coordinator Ashish Jha and CDC head Mandy Cohen are making unsupported claims the new vaccine reduces hospitalizations. long COVID and the likelihood you will spread COVID.
None of those claims has a shred of scientific support.
In fact, if the manufacturers said that, they could be fined for making false marketing claims beyond an FDA-approved indication.
The questions surrounding Moderna’s new COVID vaccine approved this week are still looming.
One in every 50 Americans has a complication with the COVID-19 vaccine.REUTERS
Pfizer’s version, approved this week as well, also has zero efficacy data and has not been tested on humans at all. We only have data about antibody production from 10 mice.
The FDA, or Moderna (frankly it’s hard to tell the difference sometimes), should disclose what happened to the patient who took the new vaccine and had a complication that required medical attention.
The public has a right to know.
The last time the Biden administration approved and recommended a novel COVID bivalent booster, last fall, with no human-outcomes data, it was an epic fail.
Only 17% of Americans took it (and some of those were forced to do so by their employer or school).
Not foreseeing such weak public support for the booster last year, the Biden administration had prepaid pharma $4.9 billion for 171 million doses — many of which were tossed in the wastebasket.
Now it is making the same mistake.
Two weeks ago, the Biden administration upped its orders for the pediatric version of the new COVID vaccines from 14.5 million doses at $1.3 billion to 20 million doses for $1.7 billion, which is more than four times as many pediatric doses used last year.
There clearly seems to be a special push this time to give it to children — the same group European regulators are not supporting.
In fact, the original Moderna vaccine was banned in parts of Europe for people under age 30.
European doctors are not alone.
Dr. Paul Offit, a vaccine-mandate supporter and FDA adviser from the University of Pennsylvania, told The Atlantic this week that he’s not going to take the new COVID vaccine.
He didn’t take the bivalent booster last fall either, despite being 72 years old.
While he disagreed with White House adviser Dr. Ashish Jha on the booster, he recently confessed, “Yes, he was wrong, but you know you can’t say that exactly.”
Yes, you can.
America is tired of political apologists as medical experts. They want the truth.
Offit is at least more honest than most experts who put their heads in the sand and parroted whatever public-health officials said.
Pfizer made $100 billion during the pandemic. It can afford to fund a randomized trial to demonstrate to the American people the new booster is effective.
That’s the scientific process.
Unlike influenza, COVID-19 is constantly circulating so there is ample opportunity to run a trial; indeed Moderna already ran a randomized trial.
Its trial of just 50 people began four months ago and oddly only reported 14-day side effects.
Why didn’t it enroll more people in its trial? Why didn’t it report three-month effectiveness and do a proper trial?
Conducting a placebo-controlled trial in people during this time would not only yield useful information; it would enable further study of those subjects three and six months from now, when a winter surge may occur.
Let’s be honest: Follow-up studies of COVID vaccines in general have revealed a disappointing truth — mild efficacy against infection is transient, lasting just a few months.
Perhaps Pfizer and Moderna knew the FDA regulatory process was greased for them and they didn’t have to.
It’s time for the FDA to resume its role as a regulator and not the marketing department for Pfizer and Moderna.
It is possible a new booster may help downgrade the severity of COVID infection for select high-risk populations, but that’s all the more reason a proper clinical trial is needed.
It’s also worth noting the CDC’s new recommendation ignores natural immunity, which means many schools will do the same.
A February Lancet review of 65 studies concluded natural immunity is at least as good as vaccinated immunity and probably better.
So if a college student had COVID a few months ago, the CDC wants him or her to get the new shot anyway, but the correct scientific answer is the risks are expected to outweigh the benefit.
Supporters of pushing the novel COVID boosters point to the annual flu-shot approval process, which does not require a randomized trial.
But COVID vaccines are very different from flu vaccines.
COVID vaccines have higher complication rates, including severe and life-threatening cardiac reactions. Flu shots have a 50-plus-year safety record whereas COVID vaccines have been associated with a serious adverse event rate of one in 5,000 doses according to a German study by the Paul-Ehrlich-Institut.
Anotherstudy, published last year in the medical journal Vaccine, estimated the rate of serious adverse events to be as high as one in 556 COVID-vaccine recipients.
And for young people, the incidence of myocarditis is six to 28 times higher after the vaccine than after infection, even for females, according to a 2022 JAMA Cardiology study.
That’s one of the reasons a study we and several national colleagues published last year found that college booster mandates appear to have resulted in a net public-health harm.
Finally, at a molecular level, some scientists are concerned about what is called immune imprinting and additional ways multiple booster doses can weaken the immune system.
A study published last year in the journal Science described a reduced immune response among people infected who then received three COVID-vaccine doses.
If public-health officials get their way, a healthy 5-year-old boy will get 72 COVID-vaccine shots over the course of his lifetime, if he has an average lifespan, with a risk of myocarditis after each one.
Inexplicably and defying science, the CDC is saying even if a child had COVID three weeks ago, he or she should still get the new COVID shot.
Two of the FDA’s two best vaccine experts are gone. Dr. Marion Gruber, who was director of the FDA’s vaccine office, and her deputy director, Dr. Philip Krause, both quit the agency in 2021 in protest over political pressure to authorize vaccine boosters in young people.
Ever since the loss of these two vaccine experts, the agency’s vaccine authorizations have been consistent with an overly cozy relationship between pharma and the White House.
Pushing a new COVID vaccine without human-outcomes data makes a mockery of the scientific method and our regulatory process.
In fact, why have an FDA if White House doctors can simply declare a drug to be safe after discussing secret data in private meetings with pharma?
If public-health officials don’t want a repeat disappointing turnout of Americans who get the COVID booster shot, they should require a proper clinical trial to show the American people the benefit.
Public-health leaders cannot afford to squander any more credibility and money on interventions with no scientific support.
Marty Makary, MD, MPH, is a professor at the Johns Hopkins School of Medicine and author of “The Price We Pay.” Tracy Beth Høeg, MD, PhD, is an epidemiologist at the University of California, San Francisco.