Scientists are eyeing a potential culprit causing the allergic reactions to the Pfizer Inc. and BioNTech SE Covid-19 vaccine: the compound polyethylene glycol, also known as PEG.
Six severe allergic reactions to the vaccine have been reported in the U.S., according to the Centers for Disease Control and Prevention, out of 272,001 doses administered through Dec. 19. At least two cases of anaphylaxis have also occurred in the U.K. People in the U.S. began receiving Moderna Inc.'s vaccine Monday, and no allergic reactions to it have been reported so far.
In a statement, Pfizer said it "will closely monitor all reports suggestive of serious allergic reactions following vaccination." The company said its prescribing information includes a warning that "appropriate medical treatment and supervision should always be readily available in case of a rare anaphylactic event following the administration of the vaccine."
Scientists are homing in on PEG as a potential suspect even as health authorities say they are still investigating the incidents and plan to study the issue further. The compound is found in other drugs and is known to trigger anaphylaxis on rare occasions.
"Although I think we're just speculating here...it is known that one of the components that is present in both of the vaccines -- polyethylene glycol -- can be associated, uncommonly, with allergic reactions," said Peter Marks, director of the Food and Drug Administration's Center for Biologics Evaluation and Research, at a Dec. 18 press conference.
"What we're learning now is that those allergic reactions could be somewhat more common than the highly uncommon that we thought they were because people do get exposed to polyethylene glycol in various pharmaceutical preparations," he said, adding that the FDA also plans to watch the Moderna vaccine rollout "very closely" since both vaccines contain PEG.
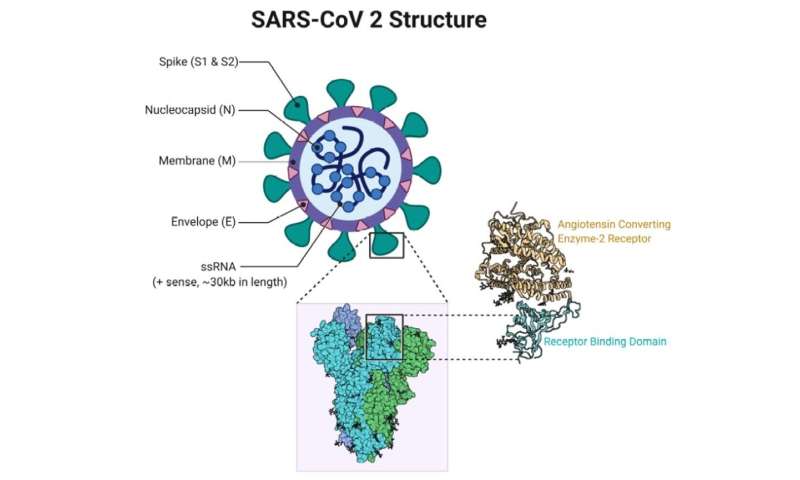
In both the Pfizer-BioNTech and Moderna vaccines, PEG is part of the fatty envelope that surrounds the messenger RNA, the main ingredient in the vaccine. Once the mRNA gets into cells, it teaches them to make a protein that resembles the spike protein found on the surface of the coronavirus. That induces a specific immune response that shores up the body's defenses for when it is exposed to the real virus. The PEG-containing fatty envelope helps ensure the mRNA gets across the cell membrane and into the cells.
Allergies to PEG are extremely rare, allergists and immunologists say, and it is possible that the few people who had reactions after getting the Pfizer-BioNTech vaccine reacted to something else. The compound is found in a range of products, they say, such as cosmetics, foods and drugs. Some vaccines also contain PEG-like compounds, they note.
Some types of PEG are more likely to cause allergic reactions than others, scientists say.
"They're all in a big large family, but in terms of their allergic potential, they're not equal," said Elizabeth Phillips, director of the Center for Drug Safety and Immunology at Vanderbilt University Medical Center. Types of PEG that are heavier are generally more likely to elicit allergic reactions than others, she said.
At the same time, "the PEG in the vaccines is different than what has been previously associated with allergic reactions," said James Baker, an immunologist who heads the Michigan Nanotechnology Institute for Medicine and the Biological Sciences at the University of Michigan.
"The overall structure is very different from anything that's been in a vaccine before," he said. That makes it hard to tell how allergic reactions to the PEG in the Covid-19 vaccines will compare to allergic reactions to other PEGs, like those in certain laxatives, that have caused rare allergic reactions in the past.
Allergy experts say it isn't certain yet whether the reactions seen so far were classic allergic reactions -- that is, immune reactions involving an antibody called immunoglobulin E, or IgE, which are part of the so-called adaptive arm of the immune system, which learns to recognize specific intruders. The reactions could also be due to a misfiring of the innate immune system, causing a cascade of reactions in what's known as the body's complement system.
"We have to look at all the possibilities," said Dr. Baker.
Both he and Dr. Phillips recently attended a virtual meeting hosted by the National Institute of Allergy and Infectious Diseases to discuss the Covid-19 vaccine allergic reactions. The agency said it is designing a study to look more closely at the issue.
"We anticipate studying highly allergic individuals with prior episodes of anaphylaxis, as well as some other groups such [as] patients with known PEG allergy," said Daniel Rotrosen, the director of the Division of Allergy, Immunology and Transplantation at NIAID, in an email. The study will include healthy individuals for comparison, he said, and researchers will gather biologic samples before and after vaccination to monitor for any immune changes induced by the vaccine.
While PEG is a possible culprit, "we need to keep an open mind regarding other possibilities," he added.
For now, the CDC says people who have a history of severe allergic reactions to any component of the Pfizer-BioNTech or Moderna vaccines should not receive the vaccine, and those who have a severe allergic reaction after the first dose should not receive the second.
People with severe allergies to any other vaccine or injectable may receive the vaccine, but should speak with their medical providers beforehand about weighing the risks of an allergic reaction with the benefits of receiving the vaccine, the agency advises.
There is no reason why people who have a history of mild or severe allergic reactions to food, pets, oral medications or environmental allergens shouldn't receive the vaccine, the CDC says.
The agency also says people who get the shots should be observed for 15 minutes after vaccination to monitor for possible adverse reactions. People with a history of anaphylaxis should be observed for 30 minutes, it says.
The FDA requires that appropriate medical treatment for allergic reactions be immediately available in the event of an acute, anaphylactic reaction.
https://www.marketscreener.com/quote/stock/PFIZER-INC-23365019/news/Scientists-Eye-Potential-Culprit-for-Covid-19-Vaccine-Allergic-Reactions-32085747/




{kind=link}
{kind=link}