Fasting plasma glucose levels outside 80-94 mg/dL, male sex, older age, and abnormal body mass index (BMI) categories all contribute to diabetes development, with additive effects.
METHODOLOGY:
Understanding the interplay between the risk factors for diabetes and its development is crucial for developing individual, practice, and population-level prevention strategies.
Researchers evaluated the risk for incident diabetes in 44,992 participants (mean age, 43.7 years; 57.8% women; mean BMI, 28.9) who had at least two fasting plasma glucose measurements between January 2005 and December 2017; participants were followed for a median of 6.8 years.
Diabetes diagnosis was defined as having a fasting plasma glucose level ≥ 126 mg/dL.
Those who met the diagnostic criteria for diabetes on or before their first fasting plasma glucose measurement were excluded.
The risk for diabetes was assessed on the basis of six categories of baseline BMI (underweight; normal weight; overweight; and class I, II, and III obesity), nine categories of initial fasting plasma glucose levels ranging from < 70 to 120-125 mg/dL, four categories of age ranging from 18 to 65 years, and sex (male or female).
TAKEAWAY:
Over the median follow-up period, 8.6% of participants developed diabetes, with a Kaplan-Meier 10-year cumulative risk of 12.8% (95% CI, 12.4%-13.2%).
Compared with a reference fasting plasma glucose level (80-94 mg/dL), both low fasting plasma glucose (< 70 mg/dL; hazard ratio [HR], 3.49; 95% CI, 2.19-5.57) and high fasting plasma glucose (120-125 mg/dL; HR, 12.47; 95% CI, 10.84-14.34) levels showed a positive association with an increased risk for diabetes.
Male sex demonstrated a higher risk for diabetes than female sex (HR, 1.31; 95% CI, 1.22-1.40); older age (≥ 60 years) also showed a higher risk than younger age (HR, 1.97; 95% CI, 1.71-2.28).
BMI variations from the normal range (18.5-24.9) increased the risk for diabetes, with both underweight (< 18.5; HR, 2.42; 95% CI, 1.77-3.29) and severe obesity (≥ 40; HR, 4.03; 95% CI, 3.56-4.56) showing notable associations.
IN PRACTICE:
"This risk estimate allows for identification of individuals with the highest risk and can facilitate options for tailored intervention," the authors wrote.
SOURCE:
This study was led by Aoife M. Egan, MBBCh, PhD, Division of Endocrinology, Diabetes and Metabolism, Mayo Clinic, Rochester, Minnesota. It was published online on January 23, 2025, in JAMA Network Open.
LIMITATIONS:
The study population was less racially and ethnically diverse and more highly educated than the overall US population. The retrospective design required participants to have at least one follow-up fasting plasma glucose test, potentially introducing selection bias. Further validation of this risk categorization tool is needed for different populations. This study omitted the second confirmatory diabetes test for asymptomatic individuals, which may have led to an overestimation of diabetes prevalence.
DISCLOSURES:
This study received support through the Mayo Clinic Robert and Elizabeth Strickland Career Development Award in Endocrinology, Metabolism, Diabetes, and Nutrition and awards from the National Institutes of Health and other sources. One author reported receiving grants from the National Institutes of Health, and another author reported receiving grants and personal fees from some pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
When new medications are so effective that physicians refer to them as “gamechangers,” it tends to generate a lot of interest. In the case ofglucagon-like peptide 1 receptor agonists (GLP-1 RAs) such assemaglutideandtirzepatide, the demand was so intense that shortages resulted.
Supriya Rao, MD
“They work really well, and the amount of weight loss that people are seeing is unprecedented,” said Supriya Rao, MD, a gastroenterologist and obesity medicine specialist, managing partner of Integrated Gastroenterology Consultants, Lowell, and director for medical weight loss at Lowell General Hospital in Lowell, Massachusetts. “These injectables have really changed the landscape.”
Many experts now suggest that the medications work so well that it’s time to expand access to these medications and allow more high-risk patients to benefit.
In fact, according to the results of a recent Medscape survey, many doctors believe that some patients deserve priority access. The survey of physicians in September found that 73% of doctors believe high-risk patients should get better access to obesity medications. For the purposes of the survey, “high risk” was defined as having conditions such as heart disease and hypertension that are exacerbated by excess weight.
Who Gets Access
Both Novo Nordisk’s Ozempic (semaglutide) and Eli Lilly’s Mounjaro (tirzepatide) received approval from the US Food and Drug Administration (FDA) for the treatment of type 2 diabetes. Demand surged when people realized the drugs also enabled people to lose significant amounts of weight.
Eventually, the FDA expanded access to these drugs by approving Wegovy (semaglutide) and Zepbound (tirzepatide) specifically for treating patients with obesity and weight-related health conditions. Wegovy was also granted approval to prevent cardiovascular events in adults with cardiovascular disease and obesity. The FDA also expanded its approval for Zepbound in December to include treatment for obstructive sleep apnea, a condition common in people with obesity.
And many doctors would like to see even more conditions approved to give easier access to people who could benefit from these weight loss medications.
“I think they should start allowing more of these metabolic comorbid conditions to qualify,” said Rao, suggesting fatty liver disease as one potential example.
The potential for lifesaving benefits would justify expanding access, said Elizabeth Benge, MD, an instructor in the Division of Sleep Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston. “For example, reducing obesity in a patient with severe comorbidities not only alleviates their symptoms but also decreases the risk of long-term complications and healthcare costs,” she said.
Brian Wojeck, MD, MPH
In fact, these medications could also benefit people who are obese and are at risk for weight-related comorbidities but haven’t developed them yet, according to Brian Wojeck, MD, MPH, an endocrinologist and assistant professor of medicine with the Yale School of Medicine, New Haven, Connecticut.
The benefit would be prevention of obesity-related comorbidities rather than addressing the damage that’s already occurred over time from conditions like type 2 diabetes, he said. “If you can prevent that from occurring, that’s huge,” Wojeck said.
Already, research continues to delve into other potential benefits of GLP-1 RAs, including a new study in Nature Medicine that suggests that these drugs may reduce the risk for dementia and other neurocognitive disorders, among others.
Two Major Barriers: Cost and Coverage
Although shortages have prevented some from getting access to semaglutide and tirzepatide, the shortages of both are over for the time being.
Currently, cost is perhaps the biggest barrier to access for most people. GLP-1 RAs are known to be expensive. Insurance coverage and manufacturer coupons can make GLP-1 RAs much more affordable with significant discounts to the list price. However, there’s a wide variation when it comes to insurance coverage of GLP-1 RAs for obesity treatment or weight loss.
Medicare doesn’t cover the cost of these medications solely for weight loss, although Medicare Part D will cover the cost of Wegovy for patients if the patients have an additional medically accepted indication, such as a history of cardiovascular disease. Many state Medicaid programs don’t cover the cost for weight loss purposes either. Some private insurance companies cover part of the cost for this purpose, but many don’t. A May 2024 Kaiser Family Foundation Health Tracking Poll found that even among the majority of patients with insurance, the cost of GLP-1 RAs was “ difficult to afford.”
Ethan Lazarus, MD
According to Ethan Lazarus, MD, obesity medicine physician, former president of the Obesity Medicine Association and owner of Clinical Nutrition Center in Greenwood Village, Colorado, cost is the main barrier for many of his patients, even high-risk patients who’ve undergone bypass surgery.
“Obesity is generally a carve-out, and in my practice, 80% of people do not have coverage, no matter how high-risk they may be,” he said. “Yes, this is unethical and needs to change.”
The majority of doctors surveyed by Medscape in September agreed that private insurance companies should start covering the cost of obesity medications and remove any existing coverage restrictions.
Physicians hope the costs will eventually drop. “In time there will be enough competition out there that these drugs will have to get cheaper,” said Wojeck.
One recent development could pave the way for lower costs. Semaglutide was named as one of 15 drugs up for Medicare price negotiations, as set up by the Inflation Reduction Act. (This will include Ozempic, Wegovy, and Rybelsus, an oral form of semaglutide.) The move could eventually lower the prices of Ozempic and Wegovy enough to make them accessible to many more older adults.
But in the meantime, that leaves physicians trying to determine how to help patients who need these medications gain access to them.
“I write a lot of appeal letters,” said Wojeck.
Also, physicians should make the effort to collect data to help them better understand their patient populations and learn what other barriers to access may exist, noted Faith Fletcher, PhD, associate professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine in Houston. For example, in some cultures, stigma may exist around weight loss, so not everyone who could benefit from GLP-1 RAs may be asking for them.
Shortages Are Over…for Now
Shortages could happen again in the future, and that could restrict access to these medications again. Physicians need to be ready, if that happens.
“If some of your patients that need GLP-1 drugs cannot get them, you should work collaboratively and creatively with others to reduce barriers to accessibility and identify viable alternatives,” said Gerard Wong, PhD, associate professor and director of the master of arts in bioethics program with Emory University’s Center for Ethics in Atlanta. “When doing so, you should consider all of the factors that affect the patient’s health, including socioeconomic status and challenges to access healthcare.”
On the morning of President Trump’s inauguration, former NIAID Director Anthony Fauci received a blanket pardon from outgoing President Joe Biden, covering any crime he may have committed in the course of his official duties and extending back to 2014. That was the year that Fauci allocated grant funding to the creation of mutant lab engineered SARS-related coronaviruses in work done at the Wuhan Institute of Virology.
Anthony Fauci is best known as the public face of the COVID-19 pandemic response, exhorting, mocking, and denouncing Americans who challenged his policy prescriptions. Fauci enjoyed robust support from the mainstream media and politicians and used his power to silence his critics. He left his post at the end of 2022, but his biggest collaborator remains at the NIH: his wife, chief bioethicist Dr. Christine Grady.
Fauci notoriously claimed that attacks on him were ‘attacks on science’. If Fauci is “the science,” Grady is “the ethics.” She received several awards in 2021 and 2022 for her work during the pandemic, but little is understood by the public about what her job entails, its consequences, or her positions on various pandemic policies. A survey of her public statements, though, reveals an authoritarian streak in her philosophy that supported Fauci’s policies, raising questions about her suitability as America’s chief bioethicist.
***
Grady has led the Bioethics Department of the NIH since 2012. Her own research focuses on ethics in clinical research design, particularly surrounding informed consent and clinical trial recruitment. She practiced as a nurse before receiving her PhD and also writes about ethical issues pertaining to that profession (a recent paper is titled “The Value of Nurse Bioethicists”). She is also a part of the Bioethics Consultation Service; a group of ethicists that help medical workers make decisions about patient care and runs a fellowship program for recent college graduates involved in ethical consultations whose alumni often go on to elite PhD programs or medical schools.
Grady’s official job description emphasizes that all her work functions “have an influence on ethical science and research, clinical practice, and health policy.” Arguably the principal vector of influence is her husband. Fauci and Grady have been married for four decades and frequently credit each other for inspiring their work in interviews, writings, and public speaking engagements.
During the COVID response, Grady influenced Fauci to push for extreme government overreach. As she explained in one co-interview with her husband: “We’ve had conversations about the sort of consequences of telling people to stay home and what it would do for the economy… And I remember having this conversation, I don’t know if you remember it? Where I said that one of the messages should be: how many lives are you willing to sacrifice? And so we’ve had that kind of conversation over dinner more than once, actually.” Fauci acknowledged that these conversations “sharpened [his] resolve to push forward” with lockdown policies.
***
Open the Books systematically analyzed Christine Grady’s public statements and publications during the COVID-19 pandemic to understand her role in the national policy conversation from 2020-2022. Fundamentally, Grady prioritized “public health” over individual freedom. Wearing a mask whenever you go outside, social distancing, getting a vaccine—to her these were simple things to do for the good of the “community” rather than questions of individual autonomy.
In a November 2021 interview, Grady outlined her philosophy: “What’s striking to me is that the kinds of burdens that we’ve asked people to undertake, like putting on a mask, don’t really infringe on one’s freedoms very much. They’re low burden and they have an effect. They do protect the person who’s wearing the mask, as well as the people that are around them.”
Yet wearing a mask at all times is not a small thing. And people were being told to do more than that by November 2021. But this posture anchors all of Christine Grady’s pandemic policies, which became more authoritarian over time.
By April 2022 Grady published a co-edited book that advocated turning bioethics on its head through the adoption of a collectivist ‘solidarity model’. She wrote: “Bioethics tends to emphasize the ethical principle of respect for persons and the right of individuals to make decisions in accordance with their interests. We should recognize that there are times when solidarity takes precedence over individual liberties.”
During an April 2020 Q&A, Grady claimed: “Unfortunately, because of visiting policies and fear of contagion sometimes when somebody is really sick their family cannot visit them, they can’t see them, but people are being creative with devices and other things where they can talk to each other… but to the questioner’s point, the stress and the sadness and the isolation on families is and is going to be great.” Two years later, her position was changed. Her co-edited April 2022 book included an essay which stated: “the solidarity model may apply to restricted family visitation, which generated moral distress for nurses, particularly when patients died without loved ones present… Designing visitation policies using a solidarity lens means considering the well-being of patients, families, and health-care professionals, and community transmission risk.”
How did Grady’s philosophy impact the Clinical Center, the on-site medical facility where she gives “bioethics consultations,” during COVID-19? We filed a FOIA request in January 2023 and have yet to receive a response.
President Joe Biden greets former Chief Medical Adviser Anthony Fauci and his wife Christine Grady in the Oval Office (January 24, 2023).
***
Grady’s position on mandates changed radically from 2020 to 2022. At first, she dismissed the idea of an “immunity passport” as a form of discrimination; because of her role as a “nurse bioethicist,” she was particularly concerned about mandates in healthcare settings. Then in early 2021, she stated vaccination should be a free choice for healthcare workers. But by November she decided the choice should be between vaccination and their jobs.
Ironically, early in the pandemic, Grady released a paper on how to respond to patients’ advance directives (written statements describing the care they wish to receive if they can no longer communicate) during COVID-19. She wrote, “Respect for persons and in particular respecting patients’ wishes regarding their medical treatment remain paramount… Not inflicting patients with invasive treatments that they do not want must remain a high priority.” Evidently, this philosophy did not survive the release of the vaccines developed by her agency and pushed by her husband. The choice between a salary and bodily integrity, for many Americans facing financial difficulties, is no choice at all.
Grady was also a strong proponent of vaccinating children, which she claimed would protect their teachers and their families. One of her major research papers from this time described the ethics and urgency of testing COVID-19 vaccines on children; despite admitting that children were at extremely low risk of serious harm from the disease. In the paper, and also in subsequent interviews, Grady listed the mental health harms inflicted on children from school closures. COVID-19 itself, rather than policy choices, was blamed for these deleterious impacts.
Although Grady does not seem to have conducted research in resource allocation directly, she often discussed frameworks developed by bodies including the CDC’s advisory committee and the World Health Organization (WHO), and emphasized that these guidelines put patient-facing healthcare workers first in line for vaccines, and nursing home patients second. Grady also spoke approvingly of race-based allocation of vaccines and other resources to address what she saw as social “inequities.”
Grady is committed to the ideology of ‘antiracism’. She participated in a Bioethics “Anti-Racism Working Group” in 2020 that sought to “develop concrete anti-racist actions that the Department can take as a whole.” During a 2021 conference held for her Bioethics fellows, participants discussed creating a “justice-oriented bioethics” in “service of social change.”
At the WHO “Ethics to Policy Summit” in December 2021, Grady argued that ethicists like herself should be involved in top-level policy discussions in order to mitigate “nationalism.” Greater international coordination and guidance from ethicists, she claimed, is needed to limit local and state “autonomous discretion” in health care decisions including decisions concerning resource allocation. Fauci, who was also at the summit, concurred: “Nationalism is a strong pull, and politicians and people are very nationalistic. To try to get them to think about global equity, and how it affects them, is an important step, but it’s not always going to win.”
***
Grady has repeatedly stated that the role of the ethicist is to “ask questions” in order to illuminate new areas of consideration in medical or policy decisions. But questions she asked during COVID were consistently leading in order to put the collective ahead of individual rights.
Where does this leave bioethics at the NIH? With respect to the question of cost-cutting via DOGE, it is unclear how much funding the Bioethics Department requires. The department belongs to the NIH Clinical Center, which is itself under the Intramural Research Program at NIH. The IRP gets about $120 million a year, but the NIH Clinical Centre doesn’t show up individually in federal budget justification documents. Open the Books asked for the Bioethics budget over a year ago and has yet to receive a response.
But even if the cost were merely Grady’s own $243,749 salary, it’s too much for the American people to bear. COVID was a test of leadership, morals, and ethics, and Grady failed it. If she cannot be fired, the department under her leadership must be radically downsized, and its influence diminished. In particular, the fellowship program that sends young people radicalized by her tutelage into elite graduate programs must be disbanded.
This is not to say there is no use for formal ethical considerations in the government. Grady, for instance, was a member of the Presidential Commission for the Study of Bioethical Issues, which was created by executive order in 2009 and expired in 2017. Commission members were selected by the president and advised on bioethical issues related to science and technology. The Commission also produced reports on a variety of bioethical issues.
President Trump could establish his own Bioethics Commission examining COVID policies like vaccine mandates, social distancing, masking, and patient isolation. Its members could lay down philosophical arguments that favor liberty and targeted interventions to protect the highly vulnerable. Before his nomination to NIH Director, Jay Bhattacharya served on the editorial board of Collateral Global. The nonprofit researches the effects of these policies and would be a good place to start looking for Commission members.
Between Grady and Fauci, COVID-19 demonstrated that ethics claims can determine policy response in disastrous ways. Although Fauci has now retired, his self-defined ethical compass and sounding board remains at NIH with a much lower profile. There’s little reason to believe the casual authoritarianism that buttressed his recommendations has changed. Fauci has gone, but Faucism has not. The Trump administration must roll it back and return public health policy to principles that safeguard individual liberty and bodily autonomy before another contagious disease licenses the administrative state to roll out a disastrous response again.
Amber Todoroff is deputy policy editor for OpenTheBooks.com, the nation’s largest private database of public spending. She holds a master’s degree from Oxford University.
The 14th Amendment does not confer automatic citizenship.
Claremont Institute scholars, including me, Ed Erler, Tom West, John Marini, and Michael Anton, President Trump’s incoming Director of Policy Planning at the State Department, have been contending for years—decades, really—that the 14th Amendment’s Citizenship Clause does not provide automatic citizenship for everyone born on U.S. soil, no matter the circumstances. Other prominent scholars, such as the late University of Texas law Professor Lino Graglia, University of Pennsylvania Professor Rogers Smith, and Yale Law Professor Emeritus Peter Schuck, have come to the same conclusion based on their own extensive scholarly research.
Claremont scholars have made the argument in books, law reviewarticles, congressional testimony, and legal briefs. President Ronald Reagan’s Attorney General, Edwin Meese, even joined one of those briefs, in which we argued against treating enemy combatant Yaser Esam Hamdi as a citizen merely because he had been born in Baton Rouge, Louisiana, while his father was working in the U.S. on a temporary work visa. Perhaps as a result of our brief in that case, the late Justice Antonin Scalia referred to Hamdi as a “presumed citizen” in his dissenting opinion.
Our argument is straightforward. The text of the 14th Amendment contains two requirements for acquiring automatic citizenship by birth: one must be born in the United States and be subject to its jurisdiction. The proper understanding of the Citizenship Clause therefore turns on what the drafters of the amendment, and those who ratified it, meant by “subject to the jurisdiction thereof.” Was it merely a partial, temporary jurisdiction, such as applies to anyone (except for diplomats) who are subject to our laws while they are within our borders? Or does it instead apply only to those who are subject to a more complete jurisdiction, one which manifests itself as owing allegiance to the United States and not to any foreign power?
Think of it this way. Someone from Great Britain visiting the United States is subject to our laws while here, which is to say subject to our partial or territorial jurisdiction. He must drive on the right-hand side of the road rather than the left, for example. But he does not thereby owe allegiance to the United States; he is not subject to being drafted into our army; and he cannot be prosecuted for treason (as opposed to ordinary violations of law) if he takes up arms against the United States, for he has breached no oath of allegiance.
So which understanding of “subject to the jurisdiction” did the drafters of the 14th Amendment have in mind?
Happily, we don’t need to speculate, as they were asked that very question. They unambiguously stated that it meant “complete” jurisdiction, such as existed under the law at the time, the Civil Rights Act of 1866, which excluded from citizenship those born on U.S. soil who were “subject to a foreign power.”
The Supreme Court confirmed that understanding (albeit in dicta) in the first case addressing the 14th Amendment, noting in The Slaughterhouse Cases in 1872 that “[t]he phrase, ‘subject to its jurisdiction’ was intended to exclude from its operation children of ministers, consuls, and citizens or subjects of foreign States born within the United States.” It then confirmed that understanding in the 1884 case of Elk v. Wilkins, holding that the “subject to the jurisdiction” phrase required that one be “not merely subject in some respect or degree to the jurisdiction of the United States, but completely subject to their political jurisdiction, and owing them direct and immediate allegiance.” John Elk, the Native American claimant in the case, did not meet that requirement because, as a member of an Indian tribe at his birth, he “owed immediate allegiance to” his tribe and not to the United States.
Thomas Cooley, the leading treatise writer of the era, also confirmed that “subject to the jurisdiction” of the United States “meant full and complete jurisdiction to which citizens are generally subject, and not any qualified and partial jurisdiction, such as may consist with allegiance to some other government.” More fundamentally, this understanding of the Citizenship Clause is the only one compatible with the consent of the governed principle articulated in the Declaration of Independence.
All of this matters a great deal because on the first day of his second term in office, President Trump issued an executive order, “Protecting the Meaning and Value of American Citizenship,” which adopted the view of the Citizenship Clause I and other Claremont scholars have espoused. It directs every department and agency of the U.S. government to accept our view henceforth as the correct interpretation of the Constitution’s Citizenship Clause.
This may be the most legally controversial executive order issued by the president on day one. And because of that, it is already being challenged in court, as 22 states have filed a lawsuit trying to block its implementation a little more than 24 hours after it was signed.
In the coming days and weeks, just as with that lawsuit, there will be lots of pundits opining that the president had no authority to issue such an order because the Constitution mandates automatic citizenship for everyone born on U.S. soil, a mandate that cannot be changed with the stroke of a president’s pen. They will contend that the Supreme Court already settled the issue more than a century ago in the 1898 case of United States v. Wong Kim Ark.
But even if Wong Kim Ark was correctly decided (as Ed Erler points out, it was not), honest scholars must acknowledge that Wong Kim Ark involved a child born to parents who were permanently domiciled in the United States, not those who were only here temporarily or illegally. Indeed, honest scholars will be forced to acknowledge that the Supreme Court has never held that the children of illegal immigrants, or even temporary lawful visitors, are constitutionally entitled to automatic citizenship merely by virtue of their birth in the United States. And they will be forced to acknowledge as true the claim in Trump’s executive order that “the Fourteenth Amendment has never been interpreted [in any formal, binding way] to extend citizenship universally to everyone born in the United States.”
Alas, when it comes to anything related to Trump, there are very few honest scholars. Instead of acknowledging the Supreme Court’s limited, actual holding in Wong Kim Ark, they will point to dicta in which the Court’s majority falsely claimed that the Citizenship Clause codified the old English common law rule known as jus soli—that anyone born on the king’s soil owed perpetual allegiance to the king. They will overlook that our Declaration of Independence was an explicit and eloquent repudiation of jus soli, stating in its closing paragraph that “these United Colonies…are Absolved from all Allegiance to the British Crown.” They will overlook that Congress did not view Wong Kim Ark as mandating automatic citizenship for everyone born on U.S. soil when, a quarter century later, it extended citizenship to Native Americans pursuant to its power under the Naturalization Clause, an act that would have been superfluous if Wong Kim Ark had already settled the matter that everyone born in the U.S., including Native Americans, were automatically citizens. And they will overlook that when a 1920s guest worker program ended in the wake of the Great Depression and more than a million Mexican workers were repatriated to Mexico, the repatriation included their U.S.-born children. No one at the time claimed that the children were U.S. citizens.
Nevertheless, despite the original meaning of the Constitution’s text, its initial interpretation by the Supreme Court, and its compatibility with the social compact “consent of the governed” political theory of the Declaration, our government agencies have for more than a half-century, without any formal amendment, court decision, or official authoritative pronouncement, been acting as though birth alone is sufficient to confer citizenship. And many children of illegal immigrants or temporary visitors have organized their lives in reliance on those informal views. (President Trump’s executive order does not disturb those interests. It makes the order applicable only to children born on U.S. soil more than 30 days after the order’s effective date, to parents who were unlawfully present, or lawfully but only temporarily present, in the United States at the time of their birth.)
As a result of this order and the inevitable legal challenges to it, the Supreme Court will now, for the first time, have the opportunity to acknowledge that the Claremont Institute’s long-standing view of the Citizenship Clause is the correct one. With the Court currently composed of more originalist justices than has been the case in more than a century, we anticipate with great optimism a careful and considered assessment of the clause and a restoration of the fundamental notion that ours is a country rooted in consent, not in the old feudal notion of jus soli that was so thoroughly rejected in our Declaration of Independence.
John C. Eastman is Founding Director of the Claremont Institute's Center for Constitutional Jurisprudence, a Senior Fellow of the Claremont Institute, and a long-time professor of constitutional law.
Liz Cheney was pardoned by former President Joe Biden for her crimes against America, but congressional investigators will continue to uncover the truth of what really happened at the 2020 election protest at the United States Capitol — including the presence of FBI informants in the crowd, the placement and discovery of pipe bombs at party offices, and various other FBI abuses.
A new select subcommittee led by Rep. Barry Loudermilk, R-Ga., will be established under the Judiciary Committee to continue the work of the previous Congress, according to multiple sources familiar with the plan. Loudermilk led the previous effort as chair of the House Administration Oversight Subcommittee. That subcommittee released and published 40,000 hours of security footage from Jan. 6, uncovered interviews suppressed by Cheney’s committee that disputed her made-for-TV allegations, and referred Cheney for prosecution over her tampering with star witness Cassidy Hutchinson. Hutchinson, a low-level Trump aide, began dramatically changing her story after clandestine correspondence with the former Republican representative. Cheney, who was hand-selected by former Speaker of the House Nancy Pelosi to run the committee and its televised show trial, accepted a pardon for her alleged witness tampering and other crimes she may have committed.
Speaker of the House Mike Johnson announced the work would continue and be fully funded in a Jan. 2 social media post after President Biden awarded Liz Cheney the Presidential Citizens Medal for leading a controversial committee that shaped the left’s understanding of the Jan. 6 protest.
“The Jan 6 Select Committee manipulated AND destroyed evidence — created a fake, phony narrative all to try and hurt Trump. They even hired a TV producer from the legacy media in a desperate attempt to legitimize what Americans knew was a total hoax and complete waste of time,” Johnson said on X. “Be assured of this: House Republicans WILL continue our investigation into this corrupt committee and it will be FULLY FUNDED so it can continue next Congress.”
As noted earlier, Loudermilk and his staff uncovered transcribed interviews Cheney’s committee had suppressed because they were at odds with the narrative she was creating. For instance, Cheney suppressed evidence that President Donald Trump pushed for 10,000 National Guard troops to protect the nation’s capital, falsely claiming she had “no evidence” to support Trump officials’ claims the White House had communicated its desire for 10,000 National Guard troops.
In fact, an early transcribed interview conducted by the committee included precisely that evidence from a key source. The interview, which Cheney attended and personally participated in, was suppressed from public release. Deputy Chief of Staff Anthony Ornato’s first transcribed interview with the committee was conducted on Jan. 28, 2022. In it, he told Cheney and her investigators that he overheard White House Chief of Staff Mark Meadows push Washington, D.C., Mayor Muriel Bowser to request as many National Guard troops as she needed to protect the city. He also testified President Trump had suggested 10,000 troops would be needed to keep the peace at the public rallies and protests scheduled for Jan. 6, 2021.
In addition, Ornato described White House frustration with Acting Secretary of Defense Christopher Miller’s slow deployment of assistance on the afternoon of Jan. 6, 2021. Not only did the committee not accurately characterize the interview, it suppressed the transcript from public review. On top of that, committee allies began publishing critical stories and even conspiracy theories about Ornato ahead of follow-up interviews with him. Ornato was a career Secret Service official who had been detailed to the security position in the White House.
Hutchinson’s televised testimony included claims Donald Trump had lunged at the steering wheel in order to commandeer a vehicle to the Capitol. The driver of the vehicle testified that Trump did not grab or reach for the steering wheel. “I didn’t see him, you know, lunge to try to get into the front seat at all,” the driver, a Secret Service agent, testified. Cheney hid the full testimony, Loudermilk revealed.
Details about the funding and composition of the select subcommittee are still being arranged. Authorizing language is being drafted and will be finalized within the next two weeks.
Mollie Ziegler Hemingway is the Editor-in-Chief of The Federalist. She is Senior Journalism Fellow at Hillsdale College and a Fox News contributor.
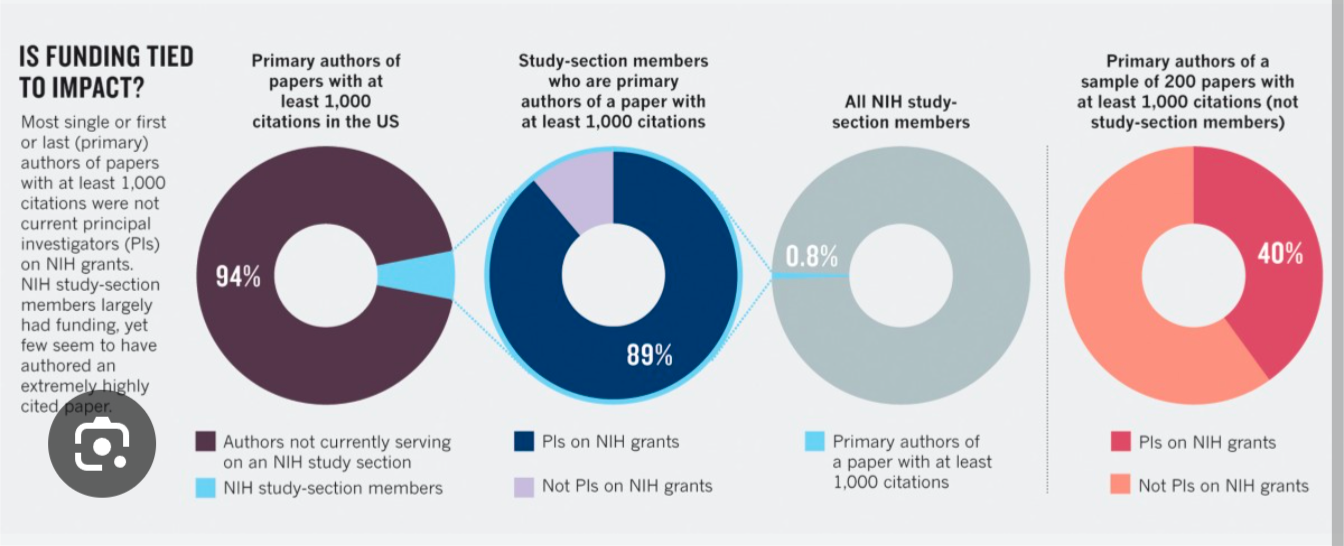
Panic unfolded yesterday as the NIH announced a pause in study sections. Study sections are groups of mediocre scientists who decide which grants are funded. You may bristle at my word choice of ‘mediocre’ but data support that claim. Here is research by Ioannidis in Nature:
He looked at authors of papers with more than 1000 citations. These are highly influential studies. I have published 530+ papers, but only one of mine fits this bucket. As such, I would make this group, but I would not have 2 years ago.
He compares this to study sections members and you can see the poor overlap. Ioannidis conclusion: conform and be funded. NIH seeks mediocre ideas that tread along established lines and not highly novel views. It does a bad job of funding people who do truly transformational work.
Trump has paused study sections to allow future NIH director Jay Bhattacharya to revisit the priorities. This is completely normal and reasonable. Jay might decide to run a randomized trial testing the current study section structure against proposed alternatives, such as the modified lottery, and other ideas.
If you randomized grant giving to several strategies, and follow the portfolio of funded projects 5 or 10 years into the future, you could analyze measures of citation, publication, impact, patent and other downstream proxies. If, there are no differences between the current process, and less bureaucratic processes, you should choose the method that has the least overhead price. This might be something Jay explores.
Alternatively, Jay might decide that having NIH funding for things like CT screening for homeless people is a misplaced used to priorities. There are many examples of woke science funding that will not survive in a Trump administration.
Scientists who quit X may protest but we live in a democracy. If you prefer more funding for diversity supplements, try to win the next election. For the time being, prepare for cuts in diversity supplements.
Interestingly, the one type of diversity that NIH is not interested in funding is intellectual diversity. That's probably a reason why they've had so much stagnation on intractable problems such as cancer and neurological conditions. They went all in brute force sequencing of tumors, and the amyloid hypothesis, for e.g.
Some people say that if the pause, which is completely reasonable, continues, people will lose their jobs in research. Of course this is true. I suspect the pause will not continue for a great period of time, but, at the same time, some people in research need to lose their jobs.
The government cannot be a welfare program for everybody doing low quality, low credibility, irreproducible, low value of information research. It has to use public dollars in a wise way. That has absolutely not occurred in the past. A pause is necessary to tackle this intractable problem.
In many ways, Jay is the perfect person to tackle this problem. He's not a laboratory scientist. He's an economist. The difference between laboratory scientists and economist is that the latter are much better at thinking brutally and clearly about the trade-offs and expected payoffs of research. Jay has already been on record as saying he thinks the NIH is not willing to push the envelope. It doesn't fund truly transformative work. I completely agree with him. And he should direct funding in that way.
The NIH call some of its pathways early innovation or something similar, but typically this is derivative work as well. The NIH does not actually take risks on truly different ideas. The envelope is not being pushed.
And the American people that want the envelope pushed. They don't want continued marginal drugs. They want new ideas. We have made no progress in Alzheimer's disease in part because of the NIH's dogmatism. I look forward to a renewed focus on a diversity of ideas in science research.
Finally, if academics want to take a sky is falling approach to every single thing Donald Trump does, they're only going to exhaust themselves.