Heart disease is something ‘old people’ need to worry about.
Sure. That is true.
But so do ‘Young People’.
Here’s why.
The mistake most people make when it comes to heart disease is thinking that when someone has a heart attack that, the condition of ‘heart disease’ just appeared.
Heart attacks present suddenly. But heart disease presents slowly.
Heart disease, the build-up of plaque in the coronary arteries, typically starts years, if not decades, prior to an event.
In many cases, you can see the risk coming years in advance.
This doesn't apply to everyone, but on average, you can see the risk coming.
So When Does Heart Disease Appear?
The answer to this question depends on how you look for it.
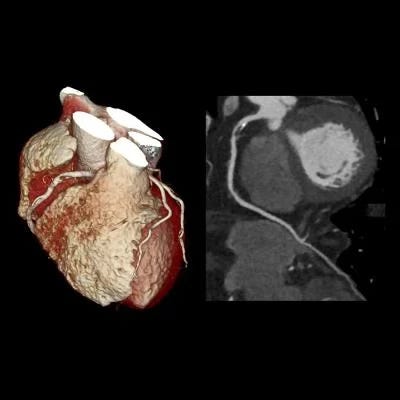
The most common way to assess the presence and extent of coronary artery disease is with a CT scan, called a CT CAC score or CT Coronary Angiogram.
These noninvasive scans look directly at the coronary arteries rather than assessing for the risk factors for coronary artery disease eg LDL cholesterol, high blood pressure etc.
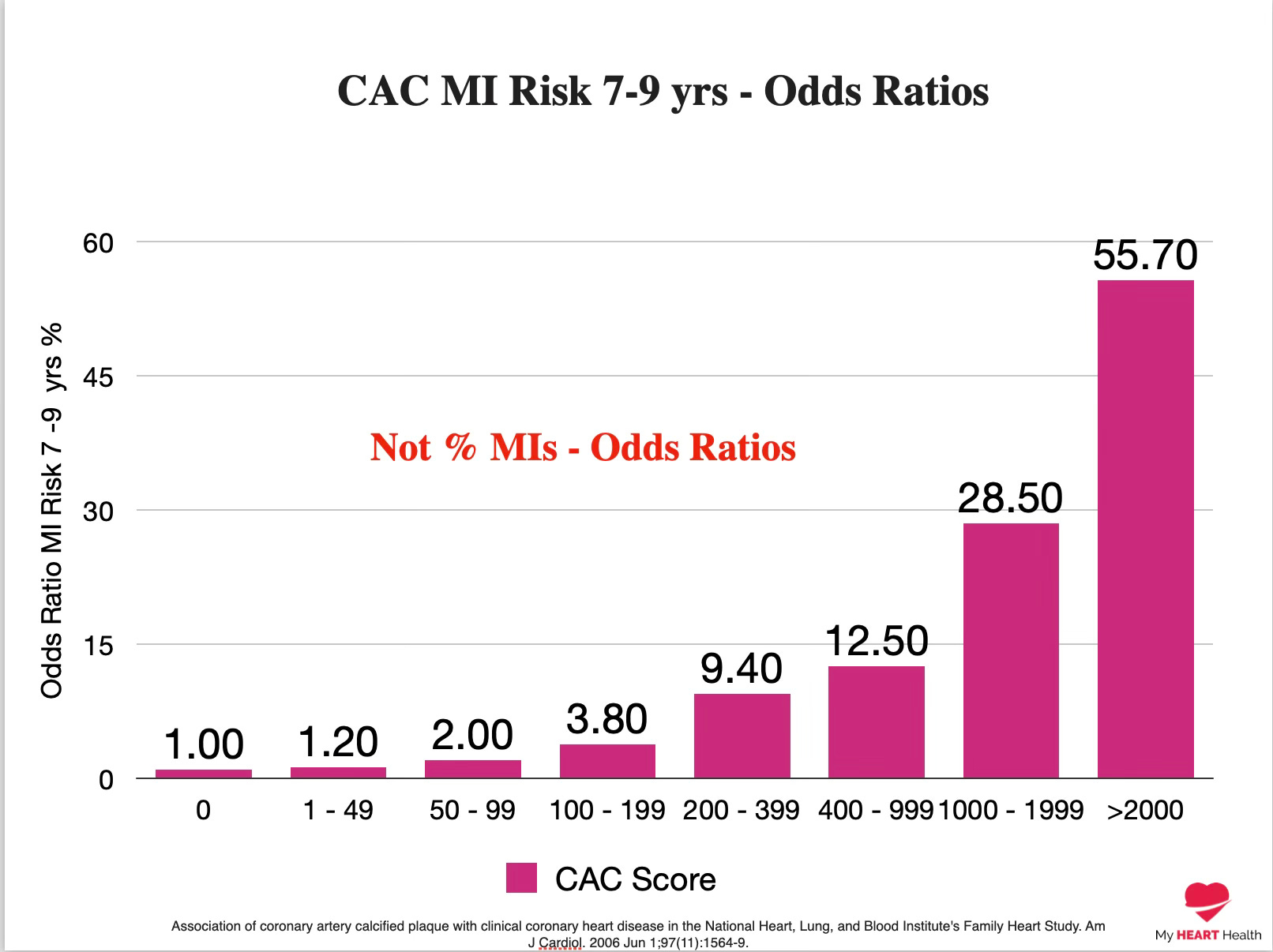
The amount of plaque is an excellent predictor of the risk of heart attack over the following 10-year period1.
The more plaque, the higher the risk.
The less plaque, the lower the risk.
As the line goes, “No Plaque. No Heart Attack”.
A CT CAC score of 0 indicates a very low risk of a heart attack over the following 10-year time frame.
However, over a long enough time horizon, everyone will convert from a CAC of 0 to a CAC above 0.
When that transition happens is important.
If it happens very early in life, then you have started to accumulate plaque and risk much earlier in life.
This transition happens about ten years later for females than males, which likely accounts for why females have major heart events later in life than aged-matched males.
In general, there is a 50% chance a male will have a CAC score > 0 at age 55, and for females, that is around age 662.
This is also why it is important to note that if you have a CAC score > 0 at below this age for your sex, you are accumulating plaque and risk earlier than compared to an aged-matched peer.
But waiting for the appearance of calcification is a bad idea.
Here’s why.
Atherosclerosis, or plaque, is a progressive condition that occurs in stages over decades.
The appearance of calcification seen on CT scans is a marker of late-stage plaque.
Calcification is primarily a feature of the later fibroatheroma stages.
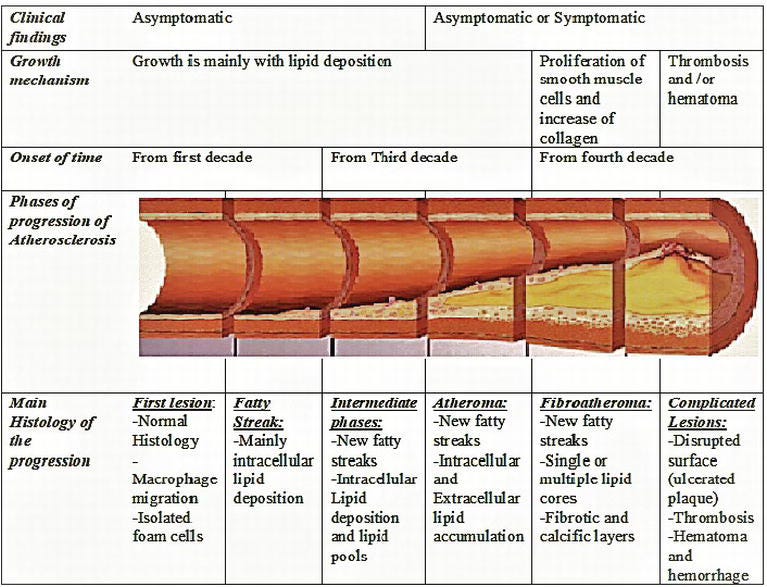
But as you can see, plaque has likely been accumulating for many years prior to the advanced stages.
So, if you have calcification in your 50s and 60s, you likely had earlier-stage plaque for many years before that.
How Much Earlier?
Way earlier than you might think.
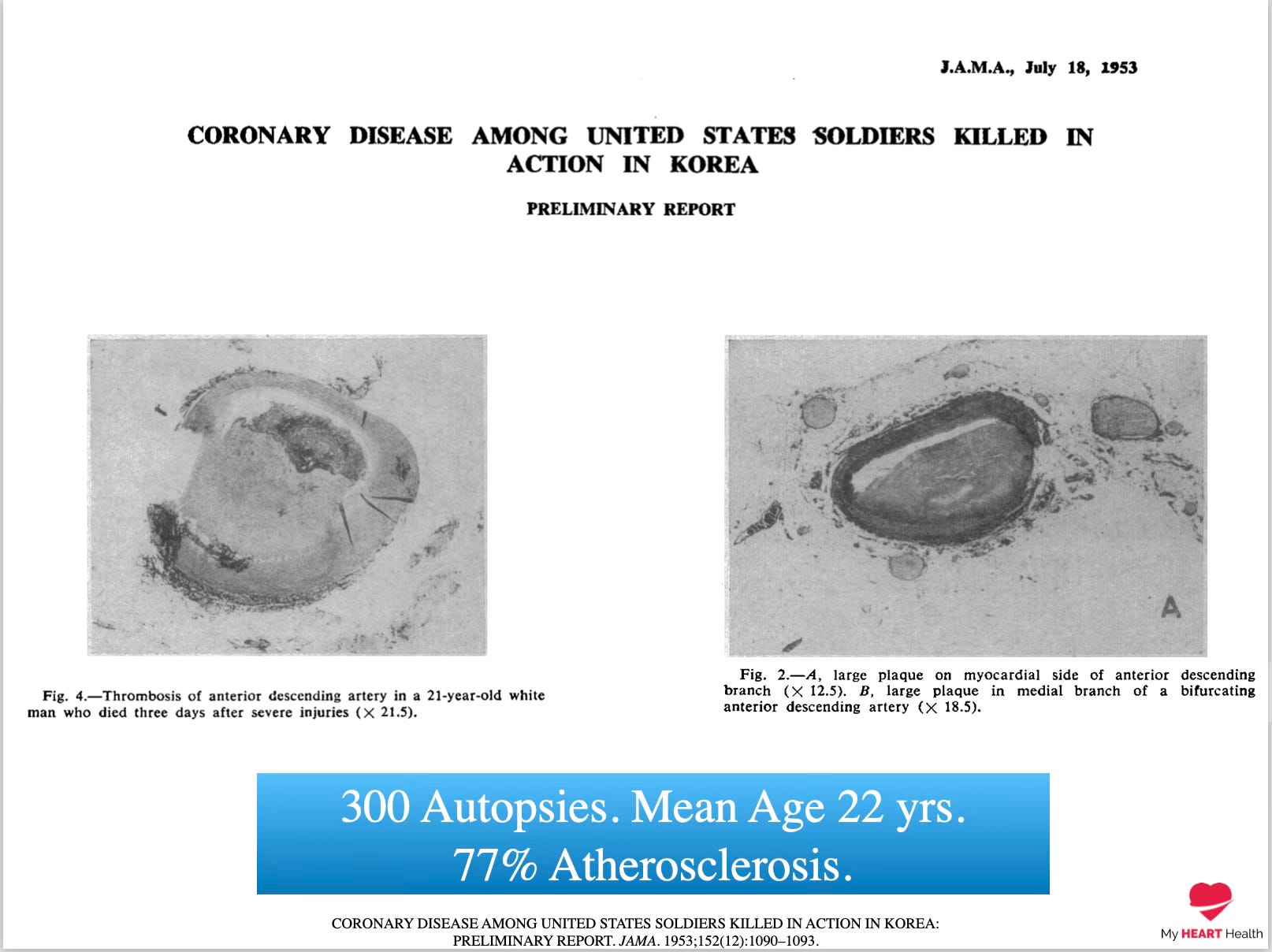
Autopsy studies of returning veterans from the Korean War who were killed in combat and not from heart-related issues were studied to see when the early stages of plaque accumulation began.
Out of 300 autopsies, 77% had evidence of early-stage plaque buildup.
The average age of these veterans was only 22 years of age3.
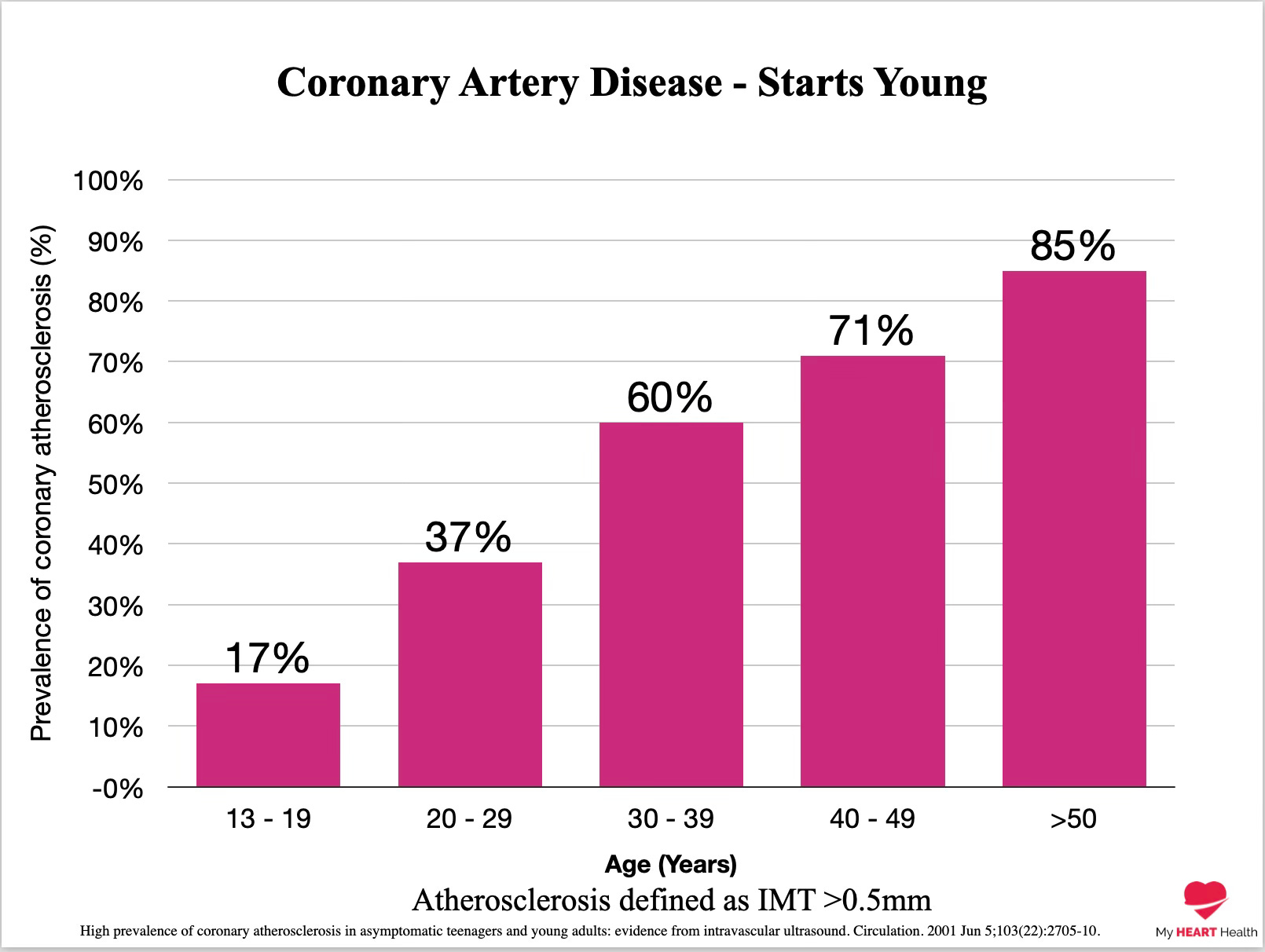
The prevalence of smoking back in the 1950s would have been much higher, but even recent studies on ‘healthy’ heart transplant donors who died from events such as road traffic accidents still show high rates of very early-stage plaque buildup4.
The very earliest stages of plaque build-up have even been noted in infants who died of sudden infant death5.
There seems to be no lower age bound on when early plaque accumulation can commence.
Two Points Should Be Made Very Clear.
Firstly, just because someone has evidence of very early-stage plaque buildup in their 20s or 30s does not mean they are at very high risk of a heart attack in the near future.
It is a marker of where someone is on a disease progression pathway.
Secondly and more importantly, IF your goal is to prevent the early build-up of significant amounts of plaque early in life, the risk factors for cardiovascular disease must be addressed early in life.
For most people, that will be an increased focus on lifestyle.
But for some, it may require medications.
The key here is to understand your goal and the time frame over which you are trying to reduce risk.
Because waiting until later in life to seriously address cardiovascular risk factors may not be the best plan.
Because the disease that is atherosclerosis is already very likely present in your coronary arteries as you read this.
And although today is an excellent time to start focusing on it.
Twenty years ago might have been even better.
Heart. An Owner’s Guide.
If you are looking for an easy and accessible explanation of heart disease and how to reduce your future risk, my best-selling book Heart. An Owner’s Guide is a great place to start.
It is suitable for all readers and is a series of two-page graphic spreads on topics ranging from insulin resistance to how to lower LDL cholesterol and high blood pressure with lifestyle measures to using fitness metrics for cardiovascular health.
Join thousands of other readers in getting started with your heart health.
You can purchase the book in all good bookstores or online by clicking here or on the image below.

Association of coronary artery calcified plaque with clinical coronary heart disease in the National Heart, Lung, and Blood Institute's Family Heart Study. Am J Cardiol. 2006 Jun 1;97(11):1564-9.
Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2006 Jan 3;113(1):30-7.
CORONARY DISEASE AMONG UNITED STATES SOLDIERS KILLED IN ACTION IN KOREA: PRELIMINARY REPORT. JAMA. 1953;152(12):1090–1093.
High prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasound. Circulation. 2001 Jun 5;103(22):2705-10.
Perinatal and infant early atherosclerotic coronary lesions. Can J Cardiol. 2008 Feb;24(2):137-41.
Dr Paddy Barrett, Preventive Cardiologist writing on how to prevent heart disease and live longer.
https://paddybarrett.substack.com/p/why-you-probably-already-have-heart
