New emails show how pandemic preparedness was reframed through a military lens at Davos in 2016, with senior NIH officials drawn into the discussions.
Behind closed doors at the World Economic Forum in Davos in January 2016, senior figures from the Gates Foundation and the World Bank proposed a new approach to pandemic preparedness: large-scale simulations modelled on military war games.
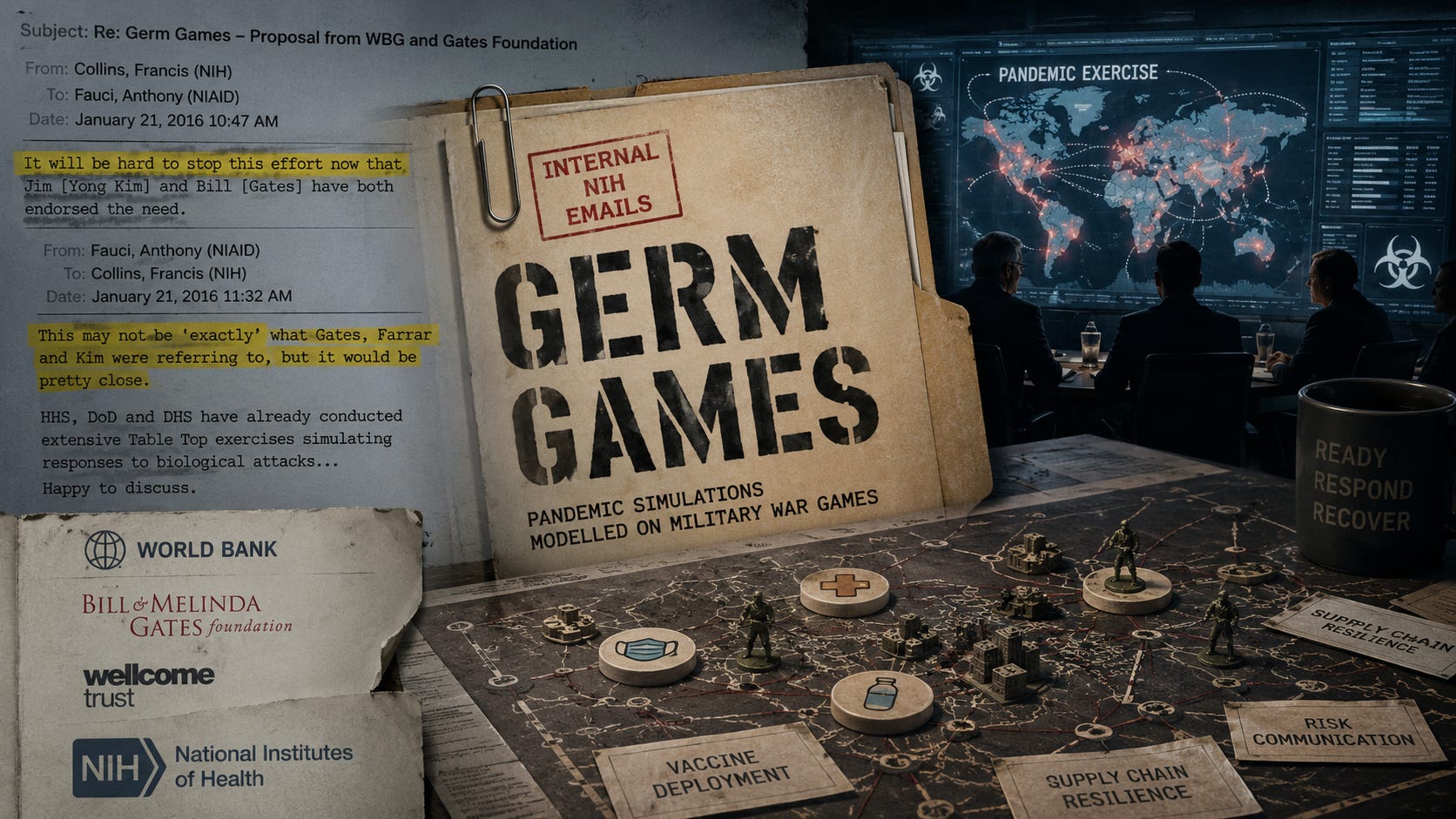
Newly obtained internal emails show how the idea — referred to as “Germ Games” — gained rapid momentum and drew in the US National Institutes of Health (NIH).
A potential land mine
On January 10, 2016, as then-NIH Director Francis Collins prepared to attend the World Economic Forum's annual meeting in Davos, he emailed an advance copy of his schedule to Anthony Fauci, one of his closest advisers.
One session, in particular, caught his attention.
“This Davos session sounds like a potential land mine,” Collins wrote.
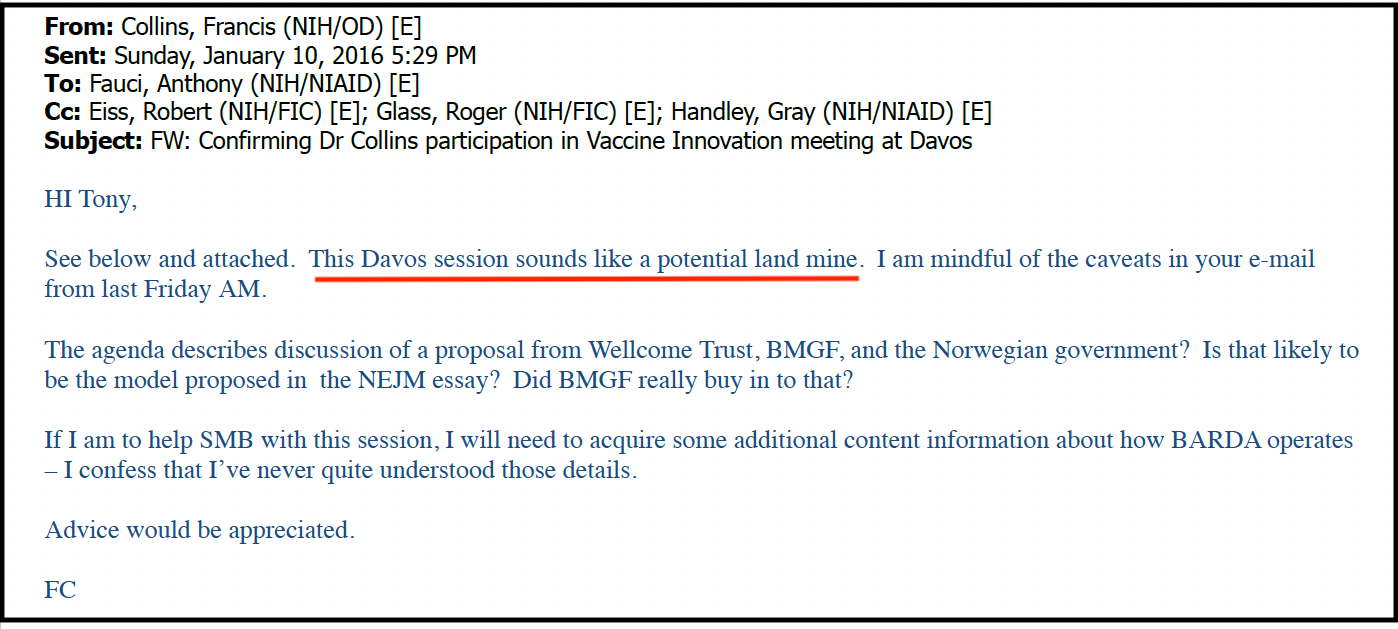
The meeting, titled “Vaccine Innovation for Pandemic Preparedness,” brought together executives from GSK, Merck and Johnson & Johnson, along with representatives from the Gates Foundation and the Wellcome Trust.
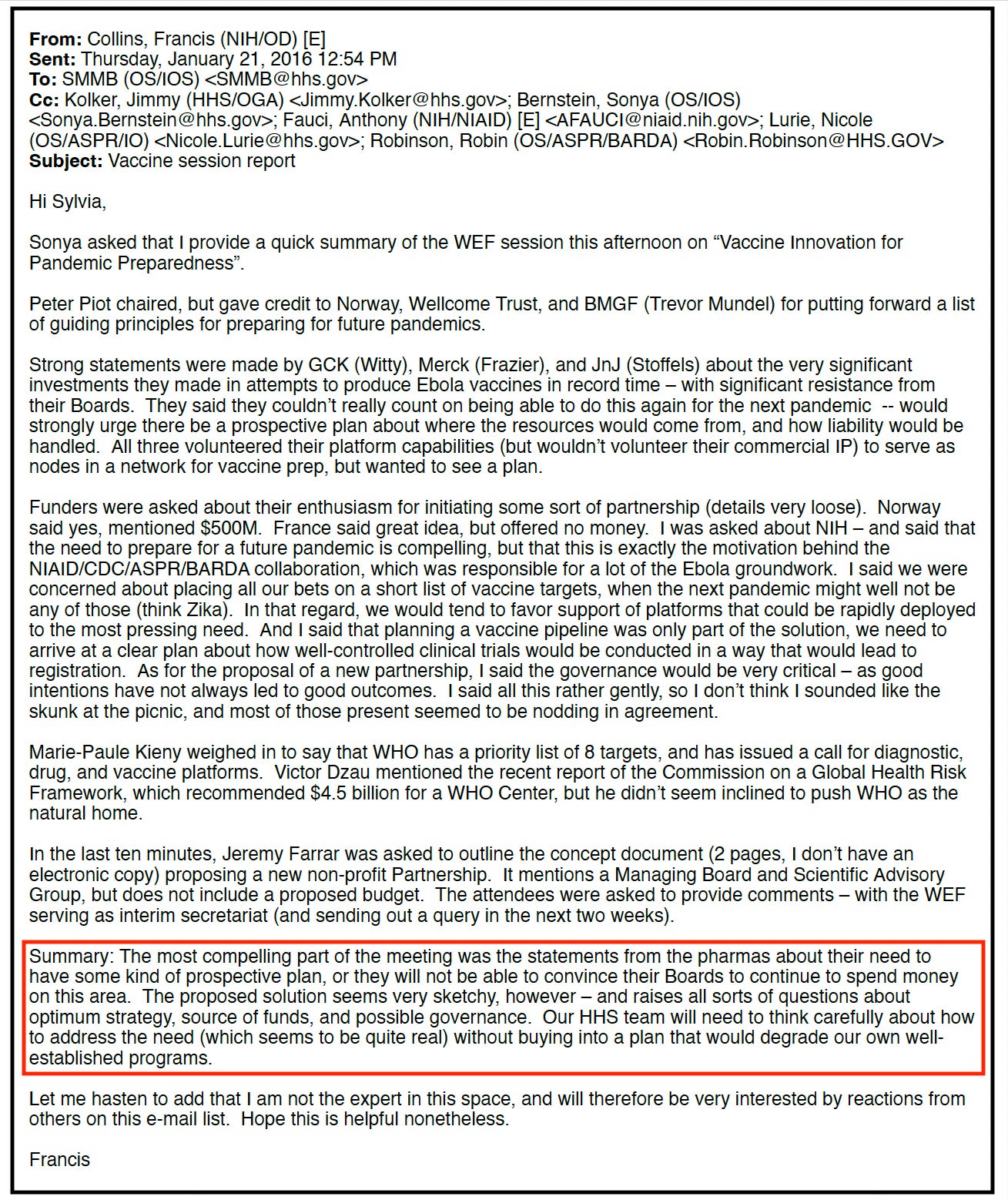
According to Collins’ report to Health and Human Services Secretary Sylvia Burwell, the pharmaceutical companies were blunt about the conditions for their participation — they could not commit to rapidly developing vaccines for every future outbreak unless governments first resolved who would pay and how liability would be handled.
The companies said they were willing to contribute their vaccine platforms but would not share their commercial intellectual property.
Collins described the emerging proposal as “very sketchy” and warned that it raised serious questions about governance, funding and strategy. He cautioned against any plan that would undermine existing US programmes.
The birth of “Germ Games”
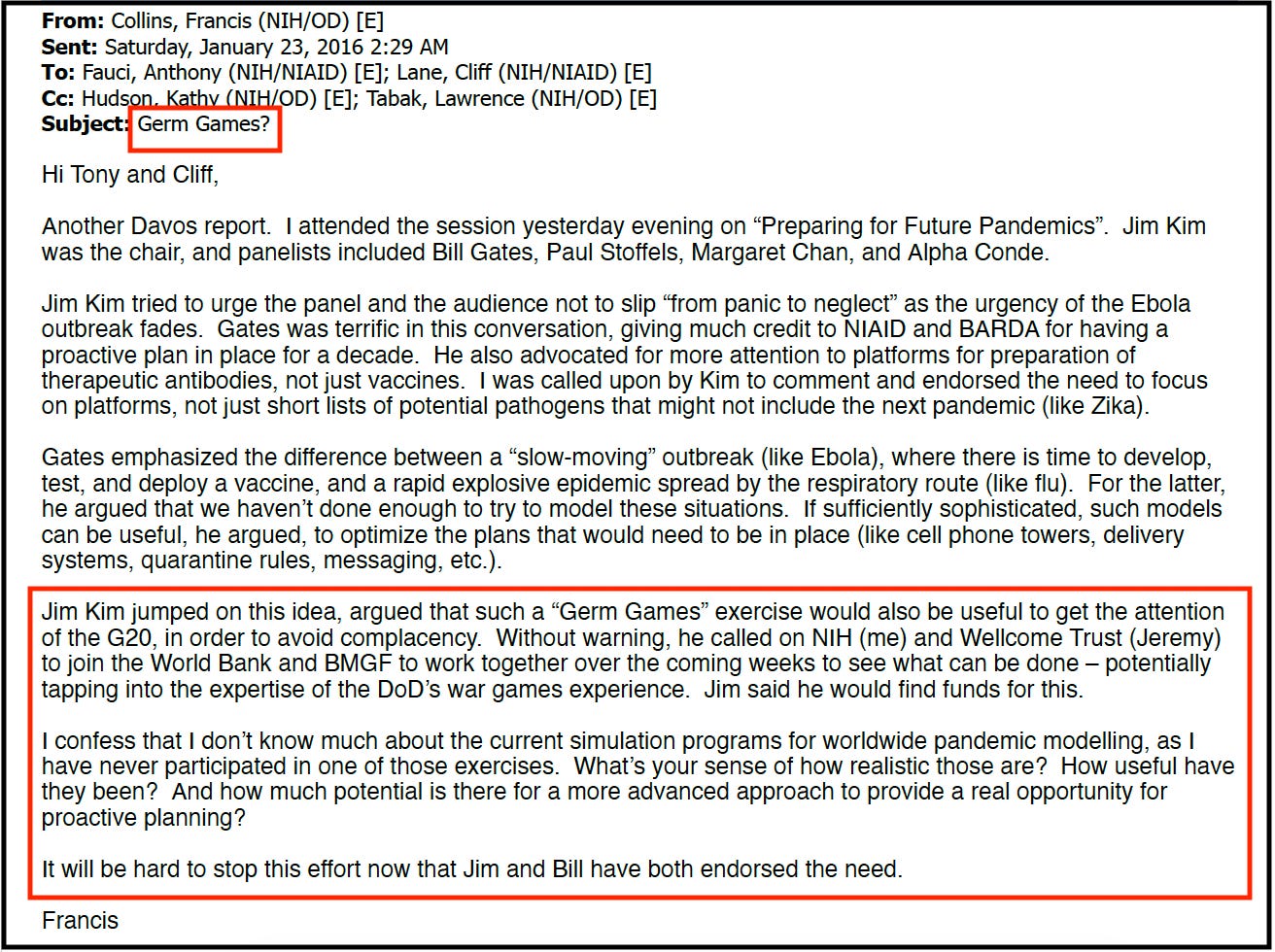
A separate session on preparing for future pandemics proved even more consequential. Chaired by World Bank President Jim Yong Kim, the discussion included Bill Gates.
Gates argued that the world was poorly prepared for a fast-spreading respiratory virus and that more sophisticated simulations could strengthen planning around logistics, communications, quarantine measures, public messaging and vaccine deployment.
Kim seized on the idea. According to Collins’ email, the World Bank president proposed creating “Germ Games” — exercises explicitly modelled on military war games — persuade G20 leaders to invest in pandemic preparedness and avoid complacency once Ebola memories faded.
Kim suggested “tapping into the expertise” of the US Department of Defense, whose war games experience tested command structures, decision-making and crisis response under pressure.
He publicly called on the NIH, the World Bank, the Gates Foundation and the Wellcome Trust to develop the concept together, saying he would “find funds for this.”
Writing to Fauci afterwards, Collins acknowledged that the proposal had quickly gained influential backing. With both the Gates Foundation and the World Bank endorsing the initiative, he wrote, it would be “hard to stop this effort now.”
Collins admitted that large-scale pandemic simulations fell outside his expertise and asked Fauci for his assessment.
Fauci’s reply
Fauci responded that the US government already had considerable experience running simulated “bioterror attacks.”
He explained that the Department of Health and Human Services, the Department of Defense and the Department of Homeland Security had conducted extensive "Table Top" exercises—simulated crisis scenarios in which officials rehearsed responses to biological threats, including aerosolised anthrax, multi-release smallpox and influenza pandemics.
“This may not be ‘exactly’ what [Bill] Gates, [Jeremy] Farrar and [Jim Yong] Kim were referring to,” Fauci wrote, “but it would be pretty close.”
He also suggested involving Nicole Lurie, then Assistant Secretary for Preparedness and Response, noting her previous experience at the RAND Corporation.

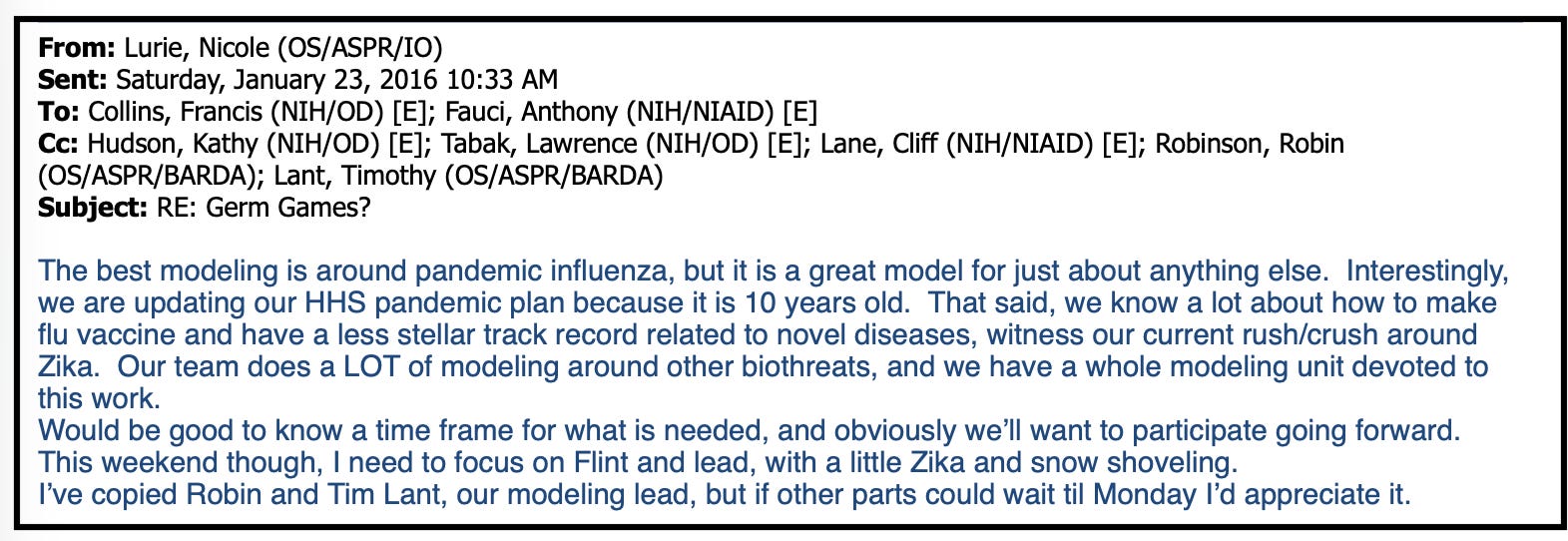
Collins quickly looped Lurie and BARDA Director Robin Robinson into the discussion, asking whether support from the World Bank and the Gates Foundation could help upgrade existing US modelling and preparedness work.
Lurie replied that HHS was already updating its pandemic influenza plan and had an entire team conducting regular modelling for a range of biological threats, including H7N9, MERS, Ebola and Zika.
From “Germ Games” to global agenda
The “Germ Games” concept did not remain a one-off idea.
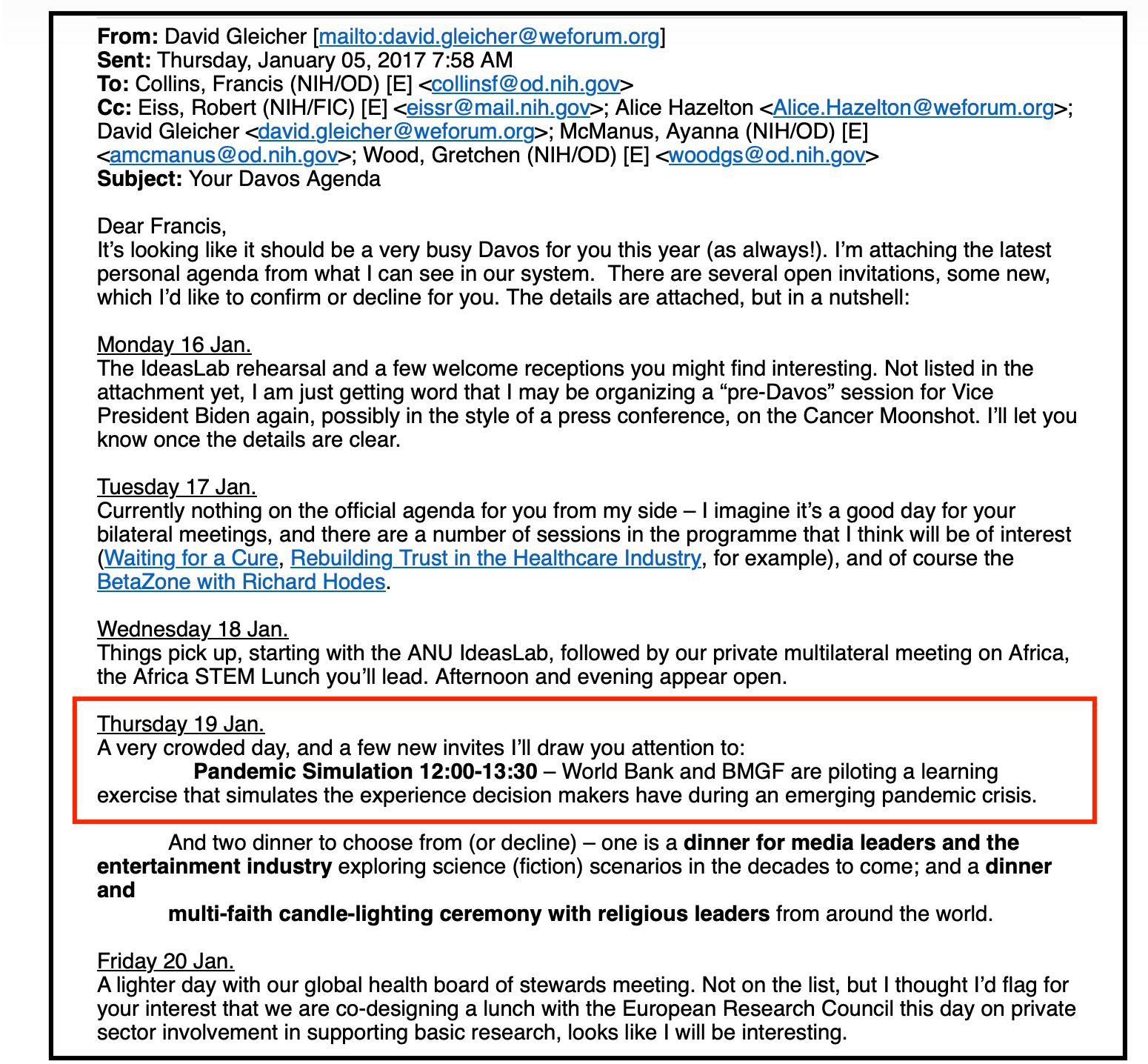
A year later, Collins returned to Davos for the 2017 World Economic Forum meeting.
His schedule included a pilot pandemic simulation organised by the World Bank and the Gates Foundation. The exercise was designed to place senior decision-makers inside a simulated pandemic crisis, using the kind of scenario-based role-playing employed in military war games.
The same approach was later reflected in Event 201, a high-profile simulation of a “fictional coronavirus pandemic” held in October 2019 by the Johns Hopkins Centre for Health Security in partnership with the WEF and the Gates Foundation.
That exercise brought together business leaders, government officials and public health experts to role-play responses to a “hypothetical” pandemic, using the same structured, scenario-based decision-making discussed at Davos three years earlier.
In early 2018, Collins invited Jim Yong Kim to the NIH.
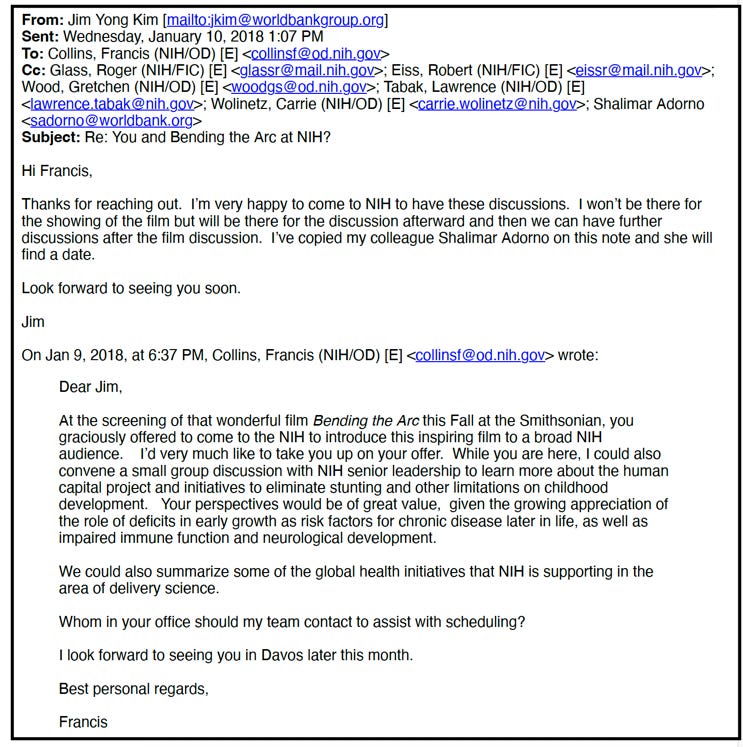
While the public event was a screening of the documentary Bending the Arc, internal planning documents show that officials arranged a closed-door roundtable with Collins, Fauci and nearly every NIH institute director.
The agenda covered pandemic preparedness, airborne threats and deeper collaboration between the NIH and the World Bank.
Collectively, these internal documents show how, from 2016 onwards, pandemic preparedness was increasingly shaped by military planning concepts and biodefence thinking.
What began as discussions at Davos evolved into a sustained international effort to embed simulation-based, war-game-style approaches into global health security — approaches that would later become central to the response to Covid-19.
https://blog.maryannedemasi.com/p/germ-games-nih-emails-reveal-the