Stephen M. Strakowski, MD: Hello. I'm Dr Steve Strakowski. I'm a professor of psychiatry at Indiana University in Indianapolis. Artificial intelligence (AI) has been all over the news, and it's slowly working its way into mental health and mental healthcare.
I’ve brought in two experts who I'm just thrilled are here to talk with us about AI and how it might affect how we practice over time. First, I want to welcome Dr Roy Perlis. Roy is vice chair for research in the Department of Psychiatry at Mass General Hospital.
Roy H. Perlis, MD, MSc: Hi, Steve. Thanks for having me.
Strakowski: Also, Martin Paulus. Dr Paulus is the scientific director at the Laureate Institute for Brain Research in Tulsa.
Martin P. Paulus, MD: Thank you, and hello everybody.
Defining ‘Artificial Intelligence’ and Algorithmic Reasoning
Strakowski: Roy, let's start with you. What is artificial intelligence? Is it a single thing?
Perlis: We think about artificial intelligence as using computers to do tasks or solve problems that traditionally required human intelligence. Sometimes people use it synonymously with machine learning, but it's somewhat broader than that. It's using computers to do tasks that in the past required human intelligence.
Strakowski: I had one of my really smart patients the other day tell me there really is no artificial intelligence, it's just increasingly complex algorithms. The computer's not really reasoning. Is that true? Martin, thoughts?
Paulus: It always depends on how you define intelligence. People in the field, at least in the development of AI systems, have sidestepped the general idea of: is there artificial intelligence? What they're really doing is benchmarking it against very specific processes and then seeing how these systems do compared to what a human might do. And they're really good at some things, and they're really bad at other things.
The important element of it is while there is a general algorithm behind the computation, there's a degree of randomness in the system as well. The computation has gotten so complex that even the people that create these systems at this point in time don't fully understand how they work. There's a basic understanding of what these systems do, but I think how they come up with precisely the solutions is still a bit of a mystery.
Quite frankly, people are studying this on all levels. Even mathematicians are looking at how cognitive processes unfold on these multilayered neural networks, which is really the architecture behind those systems.
Perlis: In fairness, we don't really understand how human cognition works either. Some people say AI is not doing what humans are doing. That's probably true, but we don't actually fully understand what humans are doing.
The things that AI tends to be good at are often different than the things that humans are good at and vice versa. Each approach to problem-solving probably has its strengths. We have to figure where does AI make sense and where does human intelligence make sense?
Large Language Models Are a ‘Neural Net’
Strakowski: What is a large language model? Because that's talked about a fair amount within the mental health space.
Perlis: If you rewind to when I was an undergraduate, I worked on modeling single neurons computationally. I had a giant SPARCstation state-of-the-art computer that could model one neuron at a time.
What really led to a lot of the modern artificial intelligence methods that Martin was alluding to was computational advances that made it possible to model whole networks of neurons. That, plus the availability of material to train them, otherwise known as the internet, are really the two things that sort of drove the field forward.
To your question, large language models are a kind of neural net. They often use a specific architecture called a transformer model, which was developed around 2017, and it's a particular way of building neural networks that turns out to solve a lot of previous computational problems.
If you understand a neural network, which most people in psychiatry have some intuition about, you understand something about how language models are built.
What AI Can and Can't Do Today
Strakowski: As these become available, they're starting to be used in mental health. There are all kinds of stories of kids getting on ChatGPT and other things, trying to actually use them as therapists, which has not been wildly successful in many cases.
Where do we think it's actually useful now, and where do we think it might go? Martin wrote a nice paper published in the June issue of the Journal of Mood & Anxiety Disorders.
Martin, you designed this figure for the paper we just mentioned. Can you walk us through it and help us think about how we might use AI currently?
Paulus: When I was presenting at the conference, and when I was thinking about where we are, it makes sense to think about it in terms of what stages we might be able to include AI at this point. Many people know that AI systems are being used, for example, for charting.
Roy has written a recent paper on this. We can talk about what it does to charting when you use AI. But that's currently already in use, and in a sense, affecting how we interact with patients. We want to think about what kind of risk exposure we have when we use AI. That's how I characterize what's suitable now, what we might be considering in the near future based on research studies, and where we are quite a bit away from considering it. Obviously, this is somewhat of a prediction. Things can be wrong here as well.
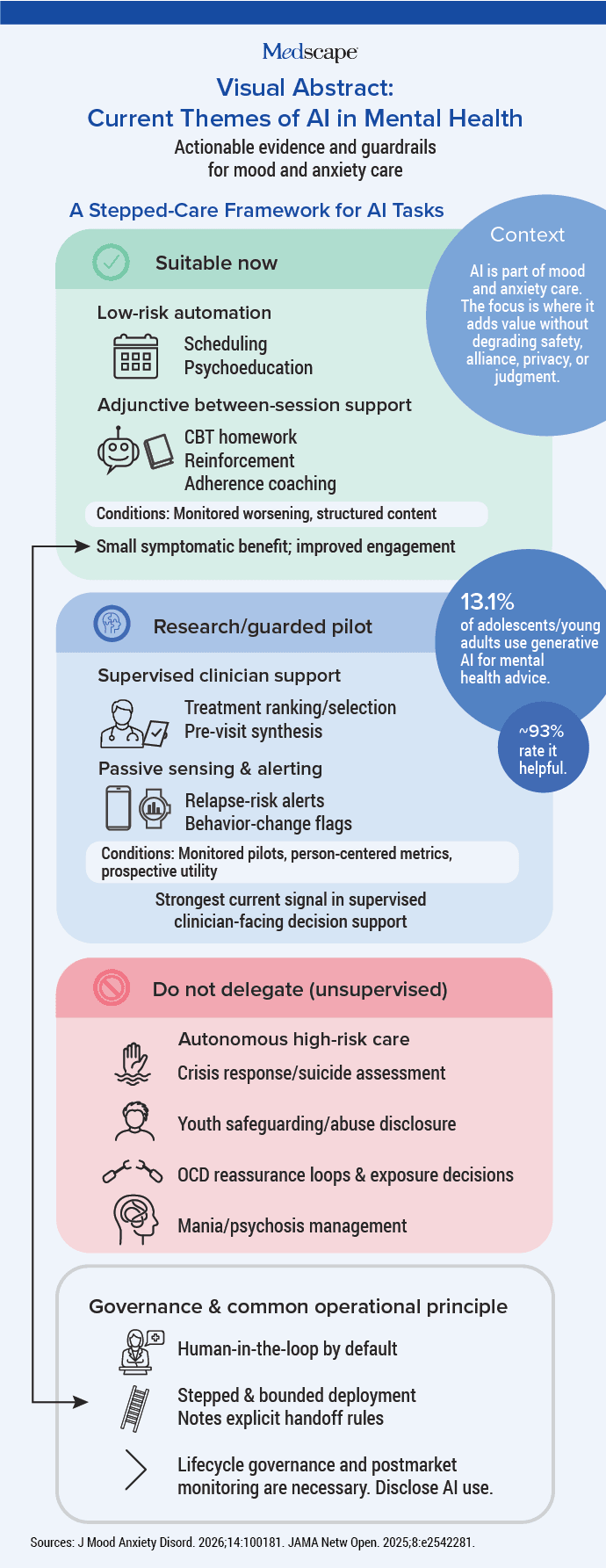
For operational purposes, I think AI can be extremely helpful now: scheduling patients, providing more extensive psychoeducation that is supervised by a clinician.
In terms of behavioral therapy, you can think of it as an adjunct to providing, for example, cognitive-behavioral therapy (CBT) homework, or making sure that people are doing what they're supposed to be doing between sessions. So, essentially, somewhat of a low-level extender. Those kinds of applications are being developed. Some have been tested. The additional efficacy is modest, but it is definitely there. Those are applications where we can think of using them at this point in time.
Where Clinical Decision-Making Gets Riskier
Paulus: Where it gets a little bit trickier, and we're going to need more data, is when we use it to help the clinician make decisions. For example, how frequently should a patient be seen? What kinds of patients should be seen by whom?
What is a little bit more problematic is having a comprehensive pre-visit synthesis. Sometimes large language models can present a write-up as being a fact when, in fact, it isn't. We have to be aware that that continues to be an issue. It's not as prominent an issue as it used to be, but in a high-risk environment, that is still a significant problem.
I also think AI systems eventually can help in analyzing and processing ongoing data as passive-sensing data, but we're not there yet. Also, Roy has done some work in this, processing the electronic health record chart itself and providing input that could help the clinician make decisions. So that, I would say, is on the research level.
AI and Psychiatric Concerns
Paulus: I definitely don't think we're there yet in terms of crisis assessments, whether it's suicide, homicide — those kinds of things.
I also think we need to be very careful when it comes to youth and the interaction between AI and youth if you're a child and adolescent psychiatrist. It is true that many youths are using it. Almost any child psychiatrist that I talk to says that their youth has previously GPTed the questions they're interested in.
There are big issues with this. There are signs from the ABCD (Adolescent Brain Cognitive Development ) study that engagement really skyrockets with these chatbots, and we don't know what the long-term consequences will be.
The other element: there were a few studies that showed GPTs can engage people in a reinforcement loop that can potentially enhance or aggravate symptoms. The study I mentioned in the review was an obsessive-compulsive disorder (OCD) study where people actually developed more OCD symptoms after a while.
And the more complex management of severely mentally ill individuals, we're still not at the stage of being able to utilize AI. That's not to say it might not be used in the future, but I would not trust an AI system to manage a person with a manic episode or a psychotic episode.
The Risk-Benefit Balance of AI
Perlis: I really appreciate framing it as a risk-benefit matrix, where it's not a one-size-fits-all solution, and the way we think about it really depends on where you are in that matrix. That's why I get frustrated when I hear people say stuff like, " I'm not interested in AI. I don't use AI." It's a little bit like saying, "I don't use computers." You can choose not to use a computer, but you're probably missing out on some things that could make you more productive.
The other thing I like about the description that Martin gave is that it's really important to understand that this is a moving target. There are things these models couldn't be used for a year ago that I feel more comfortable applying them for now, and that's quite likely going to continue to change.
One of the challenges in our field is that you're always fighting the last battle. Hallucinations are still a concern. There was an episode of The Pitt where they were using a scribe and mis-scribed one of the medications. The scribe hallucinated one of the medications. That kind of problem is real, and we're getting substantially better at managing it and building systems that are robust to hallucinations.
There was a really interesting paper about the proportion of recently published papers with fabricated or hallucinated references that gives some sense of the scale of the problem. But again, that's something that a year from now is likely to be a lot less of a concern.
In thinking of risks and benefits, my favorite analogy is riding around in a Waymo. If you're a data person and you look at Waymo's safety stats, you are safer getting in a Waymo than getting in a taxi. Look at the numbers. When I went to San Francisco, did I ride in a Waymo? No, because I was anxious about it, and I was afraid that the brakes were going to fail on a hill. That's a reasonable reaction. In the same way, we can now have autopilots that take off and fly the plane and land, and yet, there's still a pilot in the cockpit. So again, the extent to which we are going to need humans in the loop is going to change over time.
The last thing I would say is that we neglect the fact that, currently, psychiatry and psychology do a very poor job of taking care of many of the people we need to take care of. It's not a lack of intention. It's that there's an undersupply. There's huge variation in quality of care. And so, as with any other technology, you have to say, compared to what? Do I want patients using chatbots instead of therapists? No. On the other hand, if they have no access to a therapist, are there circumstances where it could be helpful to people? I believe sometimes it can be.
Why AI Is Advancing Faster Than Expected
Paulus: You hit a very important topic here, which is that the changes are massive, they're quick. There are so many new developments. For instance, we haven't talked about it, but people are using these AI systems for coding purposes. A year ago, if you tried these coding agents, they were okay, but they made mistakes, and you had to basically go through the code and correct some of the things because they weren't using the right libraries, and it was more of a headache to code with these things than it was an improvement.
Now, you basically talk to the coding agents, and they code things up, and they even do things that you didn't even think of when you asked them. When you see what they did, it makes complete sense. They're self-correcting. They're testing the codes out, so you can be assured they actually run. It's remarkable. It has changed the way that software engineers code right now. Some of the top-level people — they essentially are a supervisor of an agent that does coding.
This is an example where the progress has been incredibly rapid and not totally foreseeable in terms of the quality that is being produced. And that is what we're facing in other applications. Maybe there are some residual issues with coding, but also with developing autonomous agents doing interactions with human beings. We have to develop ways of testing where that is going. The systems are developing so fast.
One thing we need to be very clear about is that we call them large language models, and yes, they are token-based language models, but they're now multimodal models. It's not that you're just interacting with them — typing something in or using some script or something. You can use images, you can use voice, you can use other inputs, and they've been trained on these inputs. It allows a much broader way of interacting with these systems, and they're getting better at being able to process the information from different streams.
Preparing the Mental Health Workforce
Paulus: Coming back to training, we really need a body of work that helps people become proficient in basic interactions with these systems. That training process has to be scaled up incredibly fast because everybody will be affected.
When your patient comes in and says, "My GPT says I should be on this medication, not that medication," and "By the way, it gave me these five citations. Have you read them, doctor?" How are you going to respond? Those are challenges that we're going to face. Therefore, we have to train the workforce to meet those challenges. The major organizations that represent psychiatrists and other mental health workers have to stand up and say, "Here's what we need to develop."
I just talked to a colleague in Canada. They have a multisite initiative where they're developing the curriculum for mental health workers. Maybe we can learn what works from them, because the other element is we need to figure out, because it is such a new process, which teaching methods work and which teaching methods don't work.
Why Clinicians Can't Ignore AI
Strakowski: Roy, other thoughts? As a practicing clinician, how do you keep up while we wait for our organizations to start doing that, because it's not happening en masse as far as I know?
Perlis: Podcasts like this and other discussions of AI are a good place to start. What's not really an option is to just ignore it. I would say right now one of the biggest challenges is more an engineering challenge. You can read about these tools, but the actual implementation is still very much a work in progress.
Scribes maybe are the counterexample, where lots of health systems have rolled them out, and lots of community clinicians have started to employ ambient scribes. But a lot of the other things that these agentic systems can do some of the work for us will become part of the health records that we use or the systems that we use, but they're just not there yet.
These agentic systems are remarkable and may solve some of the problems that we have where the clinicians feel like AI — and decision support more generally — contributes to burnout because it's beating on them about, "You need to do this. Just go do it." Some of these automated agentic systems will help. That said, they also, in a manner analogous to hallucinating, will cheat. For example, when you have an agent writing code and you give it a series of tests to run, in some circumstances, it'll just claim to have run the test, or it'll change the test so it can win. It's very much a developing field, and I think it's important to pay attention.
But it is going to profoundly change how we practice. And I think we don't have the luxury of saying, "I'm just going to ignore this stuff." Will there be people in private practice who say, "No AI. My patients come see me, I sit and talk to them for 50 minutes, write prescriptions."? Sure, that will exist, but I think that's not going to be the norm in psychiatry and psychology — and medicine.
Strakowski: Gentlemen, very interesting. It's clearly something we have to work collaboratively as a profession to keep up with and try to learn how to use it because it is going to happen.
I recommend looking at articles that Drs Perlis and Paulus have written. And so, thank you, and we appreciate everyone who tuned in to watch this.
Stephen M. Strakowski, MD, is the professor and vice chair, Research of Psychiatry, at Indiana University School of Medicine, and a professor in the Department of Community and Global Health at the Richard M. Fairbanks School of Public Health at Indiana University in Indianapolis. He also serves as professor of psychiatry and associate vice president, Regional Mental Health, at Dell Medical School, University of Texas in Austin. In addition, Strakowski is editor-in-chief of the Journal of Mood & Anxiety Disorders.
Roy H. Perlis, MD, MSc, is professor of psychiatry at Harvard Medical School and vice chair for research in the Department of Psychiatry at Massachusetts General Hospital. His research focuses on applying data science and artificial intelligence to improve the diagnosis and treatment of psychiatric disorders.
Martin P. Paulus, MD, is scientific director and president of the Laureate Institute for Brain Research in Tulsa, Oklahoma. His research focuses on computational psychiatry, neuroimaging, and the development of biologically informed tools to improve the diagnosis and treatment of mood, anxiety, and substance use disorders.
https://www.medscape.com/viewarticle/ai-psychiatry-whats-ready-and-whats-not-2026a1000l3a
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.