Erasca, Inc., (Nasdaq: ERAS), a clinical-stage precision oncology company singularly focused on discovering, developing, and commercializing therapies for patients with RAS/MAPK pathway-driven cancers, today announced the pricing of its upsized initial public offering of 18,750,000 shares of common stock at an initial public offering price of $16.00 per share. All of the shares are being offered by Erasca. The gross proceeds from the offering, before deducting underwriting discounts and commissions and other offering expenses payable by Erasca, are expected to be $300.0 million. The shares are expected to begin trading on the Nasdaq Global Select Market on July 16, 2021 under the ticker symbol “ERAS.” The offering is expected to close on July 20, 2021, subject to the satisfaction of customary closing conditions. In addition, Erasca has granted the underwriters a 30-day option to purchase up to an additional 2,812,500 shares of common stock at the initial public offering price, less underwriting discounts and commissions.
J.P. Morgan, Morgan Stanley, BofA Securities, Evercore ISI and Guggenheim Securities are acting as joint book-running managers for the offering.
As schools around America begin to prepare for reopening this fall, many states are taking steps to stop public schools from requiring COVID-19 vaccination or proof of vaccination.
At least seven states—Alabama, Arkansas, Florida, Indiana, Montana, Oklahoma and Utah—have already passed such laws, while 34 more have introduced bills that would limit requiring someone to demonstrate their vaccination status,CNN reported.
Such moves leave public health officials worried about the limitations these laws could place on efforts to control the spread of the coronavirus and emerging variants.
"Anytime there's legislation that potentially prohibits the health department from trying to prevent the spread of disease, even if it's putting limits on masks or mandates on vaccination, then it's another step that local health departments would have to go through should there be an outbreak or a rise in cases," Lori Tremmel Freeman, chief executive officer of the National Association of County and City Health Officials, told CNN.
The various laws take different approaches, but the end result is that schools can't require coronavirus vaccines, or in some cases, proof of vaccination, CNN reported.
In Alabama, Gov. Kay Ivey signed into law a bill that states that "institutions of education may continue to require a student to prove vaccination status as a condition of attendance only for the specific vaccines that were already required by the institution as of January 1, 2021," a measure that would exclude coronavirus vaccines.
In Arkansas, its new law notes that receiving a coronavirus vaccine "shall not be a condition of education," while Florida's new law prohibits educational institutions from requiring students or residents to provide proof of vaccination, CNN said.
In Indiana, Gov. Eric Holcomb signed a similar law in late April that notes "the state or a local unit may not issue or require an immunization passport." In Montana, the law signed by Gov. Greg Gianforte in May calls it "an unlawful discriminatory practice" to "refuse, withhold from, or deny" educational opportunities based on a person's vaccination status, CNN reported.
Meanwhile, Oklahoma passed a law in June that prohibits public schools from requiring COVID-19 vaccination as a condition of admittance or attendance. And in Utah, a new law "prohibits a governmental entity from requiring that an individual receive a vaccine for COVID-19." That includes public school districts, CNN said.
Public health officials worry that prohibiting certain vaccine requirements could impact public opinion around both coronavirus vaccines and longstanding school vaccine requirements, Brent Ewig, a policy consultant for the Association of Immunization Managers, told CNN.
He pointed to another factor that is likely slowing the implementation of vaccine mandates.
"I think the other issue is because [vaccines are] still under emergency use authorization, it has created some hesitancy about going too far on this debate about mandating," Ewig said. "My sense is that there are a lot of people that are waiting on the timing of that from when it goes from FDA emergency use authorization to full licensure, which I think we expect sometime in the fall."
New U.S. COVID cases double in past three weeks
New coronavirus infections are once again climbing in the United States, driven by the highly contagious Delta variant, lingering vaccine resistance and Fourth of July celebrations.
Over the past three weeks, new cases per day have doubled, with data from Johns Hopkins showing that confirmed infections climbed to an average of about 23,600 a day on Monday, up from 11,300 on June 23. All but two states—Maine and South Dakota—have reported that case numbers have gone up over the past two weeks.
"It is certainly no coincidence that we are looking at exactly the time that we would expect cases to be occurring after the July Fourth weekend," Dr. Bill Powderly, co-director of the infectious disease division at Washington University's School of Medicine in St. Louis, told the Associated Press.
Not surprisingly, the five states with the biggest two-week jump in cases per capita all had lower vaccination rates: Missouri, 45.9%; Arkansas, 43%; Nevada, 50.9%; Louisiana, 39.2%; and Utah, 49.5%, the AP reported. Nationally, 55.6% of all Americans have received at least one COVID-19 shot, according to the U.S. Centers for Disease Control and Prevention.
Even with the latest surge, new coronavirus case counts don't come close to nearing their peak of a quarter-million per day in January. Deaths are running at under 260 per day, on average, after topping out at more than 3,400 over the winter—a graphic illustration of the power of vaccines to prevent serious illness and death in those who do become infected, the AP said.
As cases climb, health authorities in places such as Los Angeles County and St. Louis are begging even the fully vaccinated to don their masks in public once more. And Chicago officials announced Tuesday that unvaccinated travelers from Missouri and Arkansas must either quarantine for 10 days or have a negative COVID-19 test, the AP reported.
In Mississippi, which ranks lowest nationally for vaccinations, state officials are recommending that people 65 and older and those with chronic underlying conditions stay away from large indoor gatherings because of a 150% rise in hospitalizations over the past three weeks, the AP reported.
In Louisiana, which also has one of the nation's lowest vaccination rates, New Orleans officials said Tuesday that they are likely to extend social distancing measures in place at large sporting and entertainment events until the fall. Those measures include mask mandates or requirements that attendees be vaccinated or have a negative COVID-19 test. State health officials said cases of the coronavirus are surging, largely among the unvaccinated, the AP reported.
Dr. James Lawler, a leader of the Global Center for Health Security at the University of Nebraska Medical Center in Omaha, told the AP that most of the places seeing higher rates of new cases "are exactly the areas of the country that don't want to do any of these things."
But, "the descriptions from regions of the world where the Delta variant has taken hold and become the predominant virus are pictures of ICUs full of 30-year-olds. That's what the critical care doctors describe and that's what's coming to the U.S.," Lawler said. "I think people have no clue what's about to hit us."
People who've been fully vaccinated against COVID-19 have a much stronger immune system response against the new coronavirus than those who've previously been infected, according to a new study.
"Vaccinated individuals had the highest antibody levels, nearly three times higher than that of convalescent individuals recovering from symptomatic COVID-19," an Israeli team reported.
What's more, while 99.4% of vaccinated people tested positive for COVID-fighting antibodies in blood samples just six days after their second dose of vaccine, the number of these "seropositive" people fell to just under 76% for people recovering from a COVID-19 infection.
These findings might encourage people who believe they're already well-protected because of a prior encounter with SARS-CoV-2 to go ahead and get vaccinated, one expert said.
"This is an encouraging study that further confirms that vaccination against COVID-19 provides a stronger immune response than recovering from infection," said COVID-19 expert Dr. Eric Cioe-Peña, who directs Global Health at Northwell Health, in New Hyde Park, N.Y. He wasn't involved in the new research.
The study also found that men and women have different antibody levels after either vaccination or infection.
"It's well-known that there are differences in immune response that vary with sex," noted virologist Dr. Amesh Adalja, who wasn't involved in the research.
"This is likely the result of differential proportions of hormones like estrogen and testosterone," said Adalja, a senior scholar at the Johns Hopkins Center for Health Security, in Baltimore.
The new research was led by Noam Shomron, head of the Computational Genomics Laboratory at Tel Aviv University, and Dr. Adina Bar Chaim, from the Shamir Medical Center in Tel Aviv. Their team assessed COVID-19 antibody levels in more than 26,000 blood samples from vaccinated and unvaccinated people, along with people who'd recovered from their COVID-19 infections.
The researchers also found age-related differences between convalescent or vaccinated men and women.
Among those older than 51, antibody levels were found to be higher in women than in men. This may be related to the change in levels of the female hormone estrogen, which occur around this age and affect the immune system, the study authors said.
In men, a rise in antibody levels was seen starting around 35, possibly associated with changes in levels of the male sex hormone testosterone and its effect on the immune system.
Overall, young adults had a higher level of antibodies that lasted longer compared to older vaccinated adults, the study found, and a decrease at a level of tens of percent occurred over time between younger and very old adults.
In young adults, a high concentration of antibodies is usually due to a strong immune response, while in older people it usually indicates overreaction of the immune system associated with severe illness, the researchers explained.
"Further research is required in order to obtain an in-depth understanding of the immune system's response to COVID-19, to recovery from the disease, and to the vaccine," the two lead authors wrote jointly in a Tel Aviv University news release.
The study was published on medRxiv, a "pre-print" server for health research, so it's important to note that the data have not yet been peer-reviewed.
NOAA’s smoke forecast based on where fires were burning on July 15, 2021. Credit: NOAA
Something unusual happened this year in Idaho. Fire and health officials began issuing warnings about the health risks of wildfire smoke several weeks earlier than normal. With almost the entire U.S. West in drought, it was only a matter of time before the risks became reality
As an environmental toxicologist, I am interested in understanding wildfire smoke effects and how they differ from other sources of air pollution. We know that breathing wildfire smoke can be harmful. It's not totally clear what the worsening wildfire landscape will mean for public health, but research is raising red flags.
In parts of the West, wildfire smoke now makes up nearly half the air pollution measured annually. A new study by the California Air Resources Board found another threat: high levels of lead and other metals turned up in smoke from the 2018 Camp Fire, which destroyed the town of Paradise. The findings suggest smoke from fires that reach communities could be even more dangerous than originally thought because of the building materials that burn.
With large wildfires already burning, here's a closer look at what makes up wildfire smoke and what you can do to protect yourself and your family.
What's in wildfire smoke?
What exactly is in a wildfire's smoke depends on a few key things: what's burning—grass, brush or trees; the temperature—is it flaming or just smoldering; and the distance between the person breathing the smoke and the fire producing it.
The distance affects the ability of smoke to "age," meaning to be acted upon by the Sun and other chemicals in the air as it travels. Aging can make it more toxic. Importantly, large particles like what most people think of as ash do not typically travel that far from the fire, but small particles, or aerosols, can travel across continents.
Smoke from wildfires contains thousands of individual compounds, including carbon monoxide, volatile organic compounds, carbon dioxide, hydrocarbons and nitrogen oxides. The most prevalent pollutant by mass is particulate matter less than 2.5 micrometers in diameter, roughly 50 times smaller than a grain of sand. Its prevalence is one reason health authorities issue air quality warnings using PM2.5 as the metric.
The new study on smoke from the 2018 Camp Fire found dangerous levels of lead in smoke blowing downwind as the fire burned through Paradise, California. The metals, which have been linked to high blood pressure and developmental effects in children with long-term exposure, traveled more than 150 miles on the wind, with concentrations 50 times above average in some areas.
The human body is equipped with natural defense mechanisms against particles bigger than PM2.5. As I tell my students, if you have ever coughed up phlegm or blown your nose after being around a campfire and discovered black or brown mucus in the tissue, you have witnessed these mechanisms firsthand.
The really small particles bypass these defenses and disturb the air sacs where oxygen crosses over into the blood. Fortunately, we have specialized immune cells present called macrophages. It's their job to seek out foreign material and remove or destroy it. However, studies have shown that repeated exposure to elevated levels of wood smoke can suppress macrophages, leading to increases in lung inflammation.
Dose, frequency and duration are important when it comes to smoke exposure. Short-term exposure can irritate the eyes and throat. Long-term exposure to wildfire smoke over days or weeks, or breathing in heavy smoke, can raise the risk of lung damage and may also contribute to cardiovascular problems. Considering that it is the macrophage's job to remove foreign material—including smoke particles and pathogens—it is reasonable to make a connection between smoke exposure and risk of viral infection.
Recent evidence suggests that long-term exposure to PM2.5 may make the coronavirus more deadly. A nationwide study found that even a small increase in PM2.5 from one U.S. county to the next was associated with a large increase in the death rate from COVID-19.
What can you do to stay healthy?
Here's the advice I would give just about anyone downwind from a wildfire.
Stay informed about air quality by identifying local resources for air quality alerts, information about active fires and recommendations for better health practices.
If possible, avoid being outside or doing strenuous activity, like running or cycling, when there is an air quality warning for your area.
Be aware that not all face masks protect against smoke particles. Most cloth masks will not capture small wood smoke particles. That requires an N95 mask in conjunction with fit testing for the mask and training in how to wear it. Without a proper fit, N95s do not work as well.
Establish a clean space. Some communities in western states have offered "clean spaces" programs that help people take refuge in buildings with clean air and air conditioning. However, during the pandemic, being in an enclosed space with others can create other health risks. At home, a person can create clean and cool spaces using a window air conditioner and a portable air purifier.
The Environmental Protection Agency also advises people to avoid anything that contributes to indoor air pollutants. That includes vacuuming that can stir up pollutants, as well as burning candles, firing up gas stoves and smoking.
Microbiologist Ronald Corleyhas gone to work every day throughout the pandemic as director of theNational Emerging Infectious Diseases Laboratories. Within this secure lab facility in Boston, scientists study pathogens as diverse as tuberculosis, Ebola virus, yellow fever virus and Zika virus. Many investigators there quickly turned their attention in 2020 to SARS-CoV-2, the virus that causes COVID-19.
Here, Corley answers some of the most frequently asked questions about this kind of biosecure lab and the work researchers do inside it.
Infectious diseases don't respect borders. Because of the global economy and unprecedented mobility, everyone on the planet is vulnerable to potentially devastating infectious diseases that may have originated halfway across the world. In this age of high-speed travel, we are as little as 36 hours away from any outbreak.
As with SARS-CoV-2, scientists may know little about emerging pathogens or the diseases they cause. Studying these germs—whether bacteria, viruses or other microorganisms—in the safe environment of a biocontainment laboratory is the best protection humankind has against these diseases. In the lab, researchers can safely test new diagnostics, therapeutics and vaccines. The more scientists learn about these new diseases, the better prepared we are for the ones that will come after.
This is where labs like the NEIDL, and our stringent safety measures, are important. I feel safer from infection working in the NEIDL than I do in my apartment building. We know what we're working with in the lab and how to keep ourselves and others safe. But outside, I don't know who I might pass who could have a transmissible pathogen, including the coronavirus.
This is not to say that there is no risk working within the laboratory—there is. But we minimize it through a series of safety measures—including building systems, laboratory design, personal protective equipment, training and safety protocols—that have been tried and tested in laboratories across the world.
How do you try to minimize risk?
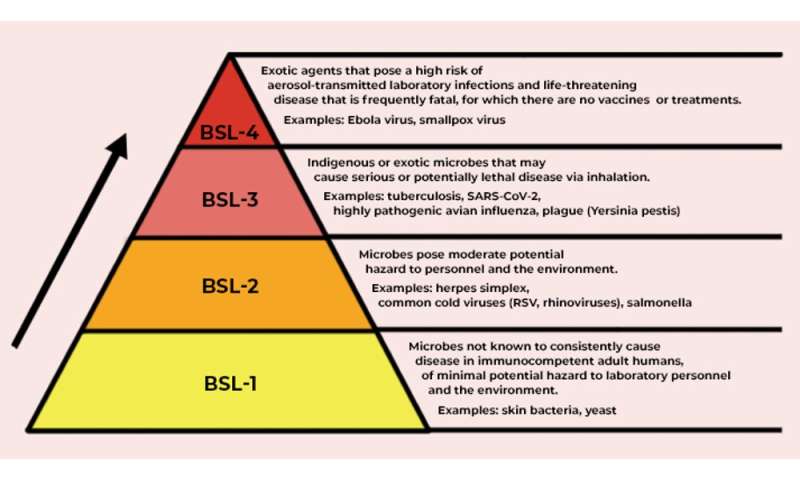
Our biosafety manual sets the standards for all work with biological material in the NEIDL. Requirements increase in complexity from Biosafety Level 2 (BSL-2) on to BSL-3 and BSL-4.
In the U.S., the Centers for Disease Control and Prevention determines each pathogen's biocontainment level, based on what's known about how it infects its host, the severity of the disease it causes, how easily transmissible the pathogen may be and the nature of the work itself—does it potentially create aerosols, for example.
The biosafety levels require different types of engineering controls—such as the building materials the space uses, directional air flow to ensure pathogens can't get out, HEPA filtration so that only sterile air is discharged from the lab space and so on.
Biosafety levels are defined by how much risk is involved in working with particular pathogens. Credit: The Conversation, CC BY-ND
The administrative controls required vary by biosafety level, as well—safety protocols, requirements for personnel training, limiting access and so forth.
Each level requires different types of personal protective equipment: gloves and lab coats in a BSL-2 laboratory, protective lab wear and N95 or PAPR respirators in BSL-3 or a fully encapsulating suit in a BSL-4 laboratory.
"Safety First" is not just a bumper-sticker phrase at the NEIDL. Everyone from public safety officers to support staff to researchers has fully bought into the culture of safety. It informs the way we're trained and drilled, the way pathogens are transported to the facility, and policies that govern our employees. We know the risks of the work, train on protective measures, and ensure every member of our staff follows our protocols.
What does containment look like with these safety strategies in place?
Everyone undergoes annual background checks, medical clearances and training. Only cleared staff can enter the building alone.
There are limited ways into the space, one for pedestrians, and one for vehicles, like delivery trucks. Entry requires access via biometric or card access or both, and screening by security. Access controls limit staff members to entering spaces where they have permission to work, based on their training, clearances and biosafety protocols. A network of security systems and closed-circuit cameras monitors the facility.
Entering laboratories requires that workers don the appropriate PPE for the area. Within the labs, we know what pathogen we are working with and how it is being used and are confident staff are following the safety measures required to keep them safe. This ensures the safety of others in the building as well as the surrounding community.
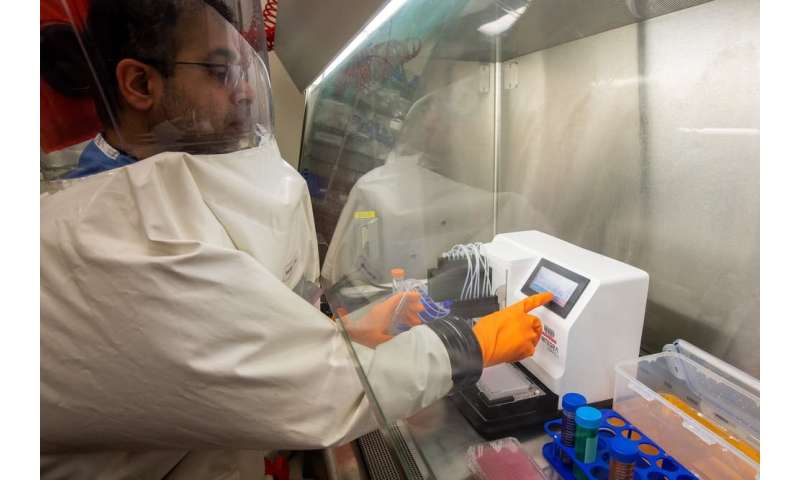
Importantly, the biosafety practices ensure that each pathogen we're studying is restricted to the appropriate spaces. Researchers work at biosafety cabinets that sterile-filter the air before releasing it back into the lab.
What kinds of regulation and oversight are there?
Biocontainment laboratories do not function in a vacuum. The building and laboratory designs, and the PPE and operating procedures that protect staff, meet the guidelines set by the CDC and by the 574-page book "Biosafety in Microbiological and Biomedical Laboratories" from the CDC and National Institutes of Health.
To carry out a project, the lead scientist begins with an application to the Institutional Biosafety Committee. Experts in biosafety and science review the application, as do laypersons who provide a community perspective. These deliberations are open and transparent thanks to public participation on the committee. Its minutes are posted online. Safety professionals also inspect the laboratory facilities before work gets underway.
In the city of Boston, projects that involve any BSL-3 or BSL-4 work require review and approval from the Boston Public Health Commission, one of the only local public health departments with this type of oversight. Work with certain types of pathogens called "select agents" that pose a severe threat is further regulated by the Division of Select Agents and Toxins within the CDC.
Here at the NEIDL, both city and federal officials inspect the laboratories, interviewing personnel and reviewing records, including maintenance records. They also inspect pathogen inventories. Inspections can be announced or unannounced.
Working with pathogens only within a specially ventilated biosafety cabinet provides another layer of security. Credit: Boston University Photography, CC BY-ND
What would happen if something went wrong?
An important aspect of safety is making sure everyone knows what to do in an emergency. Three trainings per year involve first responders from the city as well as from Boston University. These are done as either live drills or tabletop exercises with experts walking through what an emergency would look like. Afterward we review how we did and develop plans for improvement.
Community members are also part of the exercises, and this keeps our neighbors involved and hopefully provides assurance of our ability to handle accidents, keeping ourselves and the community safe.
At Boston University, we post all laboratory incidents, including those at the NEIDL, on a quarterly basis to ensure that we remain transparent in our activities. Depending on what went wrong, we may also report to the BPHC and the CDC.
Why place these high-security labs in urban environments with lots of neighbors instead of the middle of nowhere?
Scientific research is a communal activity, and advances happen in places where diverse expertise is concentrated. It's no different for research on emerging pathogens. Research on pathogens relies on faculty with expertise in not only the pathogens themselves but chemistry, engineering, stem cell biology, structural biology, immunology and more.
Biocontainment research also requires facilities engineers, safety professionals and security personnel. You can find personnel with diverse experience and expertise in metropolitan areas that are already home to biomedical research.
The original permitting process of the NEIDL mandated a comprehensive risk assessment to determine any potential danger for the community. After two years and independent review by two scientific panels, we ended up with the most extensive analysis of risk for any BSL-3 or BSL-4 facility in the U.S. It considered hundreds of possible scenarios that might result in exposure of a worker to a pathogen, or the release of a biological agent. The report concluded that it's as safe, or even safer, to have such a facility in an urban environment than in a rural or suburban environment.
"Near misses" have occurred at these kinds of labs within the U.S. and Europe. A near miss might, for example, involve glove tears and a potential exposure to a pathogen during laboratory work, but these have never resulted in any community infections. At the NEIDL, we intend to maintain this track record.
What are the risks of not doing this research?
Science builds on what's been learned before, accelerating our ability to respond to new outbreaks. The data we generate speeds progress on other pathogens as well, and informs how we develop and test potential therapeutics and vaccines. The risk of not doing this work is to leave ourselves more vulnerable to emerging pathogens as they arise.
Professionals working on emerging infectious diseases are interested in solving problems that benefit the public's health. We take pride in our work and are serious about our responsibility to perform our work safely and securely. We recognize that this research is often viewed skeptically and thus strive to keep the trust of the public by ensuring transparency around the work we do.
For thousands of years, people looked into the night sky with their naked eyes—and told stories about the few visible stars. Then we invented telescopes. In 1840, the philosopher Thomas Carlyle claimed that "the history of the world is but the biography of great men." Then we started posting on Twitter.
Now scientists have invented an instrument to peer deeply into the billions and billions of posts made on Twitter since 2008—and have begun to uncover the vast galaxy of stories that they contain.
"We call it the Storywrangler," says Thayer Alshaabi, a doctoral student at the University of Vermont who co-led the new research. "It's like a telescope to look—in real time—at all this data that people share on social media. We hope people will use it themselves, in the same way you might look up at the stars and ask your own questions."
The new tool can give an unprecedented, minute-by-minute view of popularity, from rising political movements to box office flops; from the staggering success of K-pop to signals of emerging new diseases.
The story of the Storywrangler—a curation and analysis of over 150 billion tweets—and some of its key findings were published on July 16 in the journal Science Advances.
Expressions of the many
The team of eight scientists who invented Storywrangler—from the University of Vermont, Charles River Analytics, and MassMutual Data Science—gather about ten percent of all the tweets made every day, around the globe. For each day, they break these tweets into single bits, as well as pairs and triplets, generating frequencies from more than a trillion words, hashtags, handles, symbols and emoji, like "Super Bowl," "Black Lives Matter," "gravitational waves," "#metoo," "coronavirus," and "keto diet."
"This is the first visualization tool that allows you to look at one-, two-, and three-word phrases, across 150 different languages, from the inception of Twitter to the present," says Jane Adams, a co-author on the new study who recently finished a three-year position as a data-visualization artist-in-residence at UVM's Complex Systems Center.
The online tool, powered by UVM's supercomputer at the Vermont Advanced Computing Core, provides a powerful lens for viewing and analyzing the rise and fall of words, ideas, and stories each day among people around the world. "It's important because it shows major discourses as they're happening," Adams says. "It's quantifying collective attention." Though Twitter does not represent the whole of humanity, it is used by a very large and diverse group of people, which means that it "encodes popularity and spreading," the scientists write, giving a novel view of discourse not just of famous people, like political figures and celebrities, but also the daily "expressions of the many," the team notes.
In one striking test of the vast dataset on the Storywrangler, the team showed that it could be used to potentially predict political and financial turmoil. They examined the percent change in the use of the words "rebellion" and "crackdown" in various regions of the world. They found that the rise and fall of these terms was significantly associated with change in a well-established index of geopolitical risk for those same places.
What's happening?
The global story now being written on social media brings billions of voices—commenting and sharing, complaining and attacking—and, in all cases, recording—about world wars, weird cats, political movements, new music, what's for dinner, deadly diseases, favorite soccer stars, religious hopes and dirty jokes.
"The Storywrangler gives us a data-driven way to index what regular people are talking about in everyday conversations, not just what reporters or authors have chosen; it's not just the educated or the wealthy or cultural elites," says applied mathematician Chris Danforth, a professor at the University of Vermont who co-led the creation of the StoryWrangler with his colleague Peter Dodds. Together, they run UVM's Computational Story Lab.
"This is part of the evolution of science," says Dodds, an expert on complex systems and professor in UVM's Department of Computer Science. "This tool can enable new approaches in journalism, powerful ways to look at natural language processing, and the development of computational history."
How much a few powerful people shape the course of events has been debated for centuries. But, certainly, if we knew what every peasant, soldier, shopkeeper, nurse, and teenager was saying during the French Revolution, we'd have a richly different set of stories about the rise and reign of Napoleon. "Here's the deep question," says Dodds, "what happened? Like, what actually happened?"
Global sensor
The UVM team, with support from the National Science Foundation, is using Twitter to demonstrate how chatter on distributed social media can act as a kind of global sensor system—of what happened, how people reacted, and what might come next. But other social media streams, from Reddit to 4chan to Weibo, could, in theory, also be used to feed Storywrangler or similar devices: tracing the reaction to major news events and natural disasters; following the fame and fate of political leaders and sports stars; and opening a view of casual conversation that can provide insights into dynamics ranging from racism to employment, emerging health threats to new memes.
In the new Science Advances study, the team presents a sample from the Storywrangler's online viewer, with three global events highlighted: the death of Iranian general Qasem Soleimani; the beginning of the COVID-19 pandemic; and the Black Lives Matter protests following the murder of George Floyd by Minneapolis police. The Storywrangler dataset records a sudden spike of tweets and retweets using the term "Soleimani" on January 3, 2020, when the United States assassinated the general; the strong rise of "coronavirus" and the virus emoji over the spring of 2020 as the disease spread; and a burst of use of the hashtag "#BlackLivesMatter" on and after May 25, 2020, the day George Floyd was murdered.
"There's a hashtag that's being invented while I'm talking right now," says UVM's Chris Danforth. "We didn't know to look for that yesterday, but it will show up in the data and become part of the story."
More information: "Storywrangler: A massive exploratorium for sociolinguistic, cultural, socioeconomic, and political timelines using Twitter" Science Advances (2021). DOI: 10.1126/sciadv.abe6534
CSIRO, Australia's national science agency, played an important role in evaluating heat-tolerant COVID-19 vaccine formulations developed by the Indian Institute of Science (IISc) and biotech start-up Mynvax—against all current SARS-CoV-2 variants of concern.
Published last week in the peer-reviewed ACS Infectious Diseases journal, researchers showed the vaccine formulations triggered a strong immune response in mice, protected hamsters from the virus, and remained stable at 37°C up to a month and at 100°C for up to 90 minutes.
Most vaccines require refrigeration to remain effective, like Oxford-AstraZeneca which must be kept between 2-8°C and Pfizer which requires specialized cold storage at -70°C.
CSIRO scientists at the Australian Center for Disease Preparedness in Geelong contributed to the study by assessing vaccinated mice sera (blood samples) for efficacy against key coronavirus variants, including the Delta variant currently spreading globally including in Sydney.
Dr. S.S. Vasan, CSIRO's COVID-19 project leader and co-author, said the Mynvax-vaccinated mice sera show a strong response to all variants of the live virus.
"Our data shows that all formulations of Mynvax tested result in antibodies capable of consistent and effective neutralization of the Alpha, Beta, Gamma and Delta SARS-CoV-2 variants of concern," Dr. Vasan said.
CSIRO's evaluation of the different Mynvax formulations will support selection of the most suitable candidate for planned human clinical trials in India later this year.
CSIRO's Health and Biosecurity Director, Dr. Rob Grenfell, said the pandemic has demonstrated the need for global scientific collaboration to address the urgent demand for multiple cost-effective COVID-19 vaccines and treatments.
"CSIRO has a long history of developing and testing vaccines for humans and animals," Dr. Grenfell said.
"Since the start of the pandemic, CSIRO has played a crucial role in fighting COVID-19 by conducting preclinical evaluation of two COVID-19 vaccines including Oxford-AstraZeneca, tracking emerging variants of concern, and monitoring wastewater to detect hotspots in the community.
"A thermostable or 'warm vaccine' is critical for remote or resource-limited locations with extremely hot climates which lack reliable cold storage supply chains, including regional communities in Australia's outback and the Indo-Pacific region."
The peer-reviewed paper, Immunogenicity and protective efficacy of a highly thermotolerant, trimeric SARS-CoV-2 receptor binding domain derivative, was published by ACS Infectious Diseases on 15 July 2021.