Moderna's COVID-19 vaccine appeared to have a higher effectiveness rate compared with the Pfizer vaccine during the period of time when the Delta variant first became predominant, researchers reported.
While both vaccines were highly protective against infection from January to July in Minnesota (Moderna 86%, Pfizer 76%), their effectiveness estimates declined during the month of July, with an estimate of 76% for Moderna (95% CI 69-81) and 42% for Pfizer (95% CI 13-62), reported Venky Soundararajan, PhD, of nference, a healthcare research company in Cambridge, Massachusetts, and colleagues.
Moreover, in a matched cohort from multiple states, a two-fold risk reduction against breakthrough infection was seen with Moderna's vaccine versus Pfizer's (incidence rate ratio [IRR] 0.50, 95% CI 0.39-0.64), the authors wrote in a study published on the preprint server medRxiv.
However, they found no significant differences in the rate of complications in breakthrough cases from either vaccine, with similar rates of 21-day hospitalizations, 21-day ICU admissions, and 28-day mortality.
An earlier report of a Cape Cod cluster of breakthrough infections published in Morbidity and Mortality Weekly Report late last month did not seem to find an imbalance between the percentage of breakthrough infections and the percentage of Massachusetts residents who received the vaccine (46% and 56% with Pfizer, and 38% and 38% with Moderna, respectively).
In the current study, Soundararajan and co-authors examined adults in the Mayo Clinic Health System or affiliated hospitals in Minnesota, Arizona, Florida, Iowa, and Wisconsin with at least one PCR test for SARS-CoV-2 who received at least one dose of Pfizer or Moderna vaccine after Dec. 1, 2020 but before July 29, 2021, and who did not test positive prior to receiving their first vaccine dose.
Overall, 119,463 patients met this criteria for the Pfizer vaccine, and 60,083 met this criteria for Moderna, the authors said.
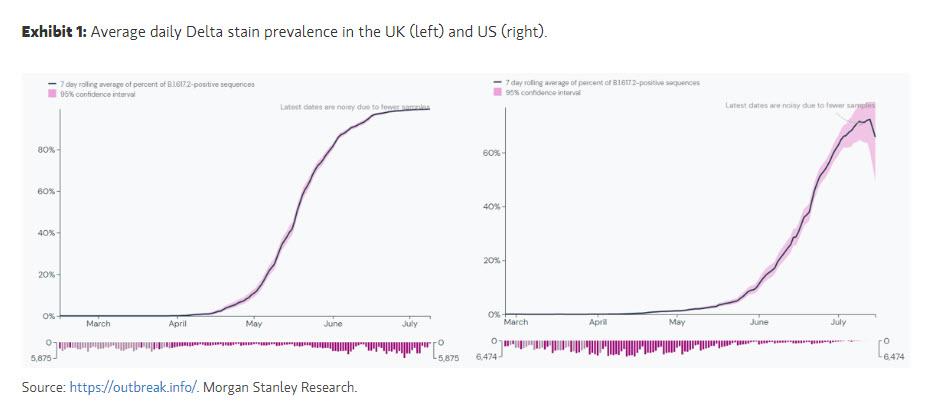
Notably, the prevalence of Delta variant in Minnesota in July was 70% compared with a prevalence of 0.7% in January.
To determine vaccine effectiveness, they matched demographically and "clinically similar" unvaccinated, Moderna-vaccinated, and Pfizer-vaccinated individuals by sex, race, ethnicity, state of residence, SARS-CoV-2 PCR testing history, and date of vaccination, yielding 43,895 "matched triples."
Clinical outcomes of interest included SARS-CoV-2 infection, COVID-associated hospitalization, ICU admission, mortality, and breakthrough infection (defined as infection occurring at least 14 days after the second dose of mRNA vaccine).
From January to July in Minnesota, both the Moderna and Pfizer vaccines were effective at protecting against COVID-associated hospitalization (91.6% vs 85%, respectively) and ICU admission (93.3% vs 87%, respectively). There were no deaths in either cohort.
The Moderna and Pfizer cohorts also had similar rates of hospitalization in Minnesota, the authors noted (IRR 0.57, 95% CI 0.17-1.7, and IRR 0.53, 95% CI 0.0089-10, respectively).
When examining data from multiple states, breakthrough infections were less likely among the Moderna cohort versus the Pfizer cohort. The rate of hospitalization was lower among those vaccinated with Moderna compared with Pfizer (IRR 0.51, 95% CI 0.29-0.88), though the authors found that COVID-associated ICU admission rates were comparable.
When examining data from Florida only, the authors found that risk of infection in July -- when the state started to experience their Delta surge -- was lower in the Moderna cohort versus the Pfizer cohort (IRR 0.39, 95% CI 0.24-0.62).
"We observed a pronounced reduction in the effectiveness of BNT162b2 [Pfizer] coinciding with the surging prevalence of the Delta variant in the United States, but this temporal association does not imply causality," Soundararajan and colleagues wrote.
The cohorts were not geographically representative of the American population, which limits their generalizability. In addition, it was possible that the vaccine effectiveness estimates were impacted by unknown exposure risk variables that were missed in the matching procedure, the authors noted.
They called for further research, namely a head-to-head comparison study of the neutralizing antibody titers produced by both vaccines, as well as larger studies with more diverse populations to further investigate this issue.
Disclosures
Puranik, Soundararajan, and other co-authors are employed by nference, which is collaborating with Moderna, Pfizer, Janssen, and other bio-pharmaceutical companies on data science initiatives unrelated to this study.
Other co-authors disclosed support from Elsevier, Bates College, nference, National Institute of Allergy and Infectious Diseases, amfAR, Mayo Clinic, and various ties to industry.
Several co-authors are employees of the Mayo Clinic, which may stand to gain financially from the successful outcome of the research.