Three Johnson & Johnson pharmaceutical executives stood before a group of staff in the R&D unit Wednesday, joking about expensive Uber rides and one “phenomenal dinner” at a Japanese steakhouse while attending the J.P. Morgan Healthcare Conference in San Francisco in early January.
But just minutes earlier, the mood was anything but jovial, as the leaders explained to a nervous group of employees in the Janssen pharmaceutical unit an overhaul of operations for the infectious diseases and vaccine groups, with sweeping layoffs expected to claim staffers' jobs in countries around the world. Some staff members have yet to be told that their positions will be cut.
Fierce Pharma has obtained internal documents and video of a town hall meeting conducted this week describing what J&J called a “comprehensive review” of its portfolio. Moving forward, J&J plans to operate its vaccines and infectious diseases outfits as one group, the executives explained.
James Merson, Ph.D., currently the head of the infectious disease unit, is set to leave the company “to pursue his next opportunity” according to a memo sent to staff. Penny Heaton, M.D., head of the existing vaccines division, will oversee the merged unit.
One memo on the pipeline revisions says the company will continue to invest in all therapeutic areas while “deprioritizing some programs.” But an internal corporate slide presentation that was delivered to the merged therapeutic team and reviewed by Fierce Pharma shows that the company’s infectious disease pipeline is undergoing a major overhaul.
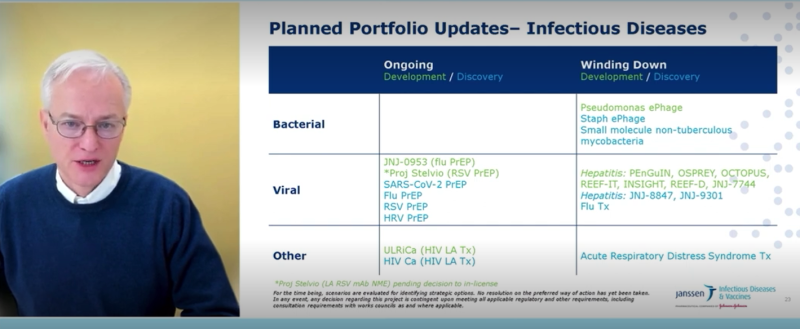
For example, the company is ending work on its hepatitis B and D therapies and continuing only “legacy studies,” according to an internal presentation slide reviewed by Fierce Pharma. J&J is also discontinuing all antibacterial therapeutic efforts, as well as work on acute respiratory distress syndrome.
The company is also winding down work of its COVID-19 and HIV vaccines, the latter of which just failed a phase 3 trial. The COVID shot was authorized during the pandemic but failed to gain a foothold in the market due to concerns about blood clots.
Moving forward, J&J plans to focus on pre-exposure prophylaxis to flu, COVID-19, RSV and HRV, the slides show.
The plan was presented to the infectious disease and vaccine team at the Wednesday town hall hosted by Heaton. Merson and Anthony Fernandez, worldwide vice president of vaccines and infectious diseases, contributed virtually.
When first reached about the cuts, J&J issued the following statement: "As the world’s largest, most diversified healthcare company, we are constantly assessing ways to be more innovative and competitive. We are evolving amidst a rapidly changing environment to better meet the needs of the patients we serve around the world."
In response to follow-up questions about the R&D re-organization, a spokesperson for J&J said: "We have nothing to add beyond the statement I provided yesterday."
Heaton began Wednesday's meeting by saying the company’s R&D divestments were impacting staff in San Francisco and Belgium. She wouldn’t elaborate on how many employees were impacted.
“And obviously I can’t disclose all of the details to you all,” she said at the meeting. “It wouldn’t be appropriate for me to do so because we want to protect the confidentiality of our team members who were impacted.”
Merson went on to blame the downsizing on “the evolving macroeconomic pressures and internal learnings” that required the company to significantly amend its aspirations. As a result, he said the company needed to focus on where it could win.
“We’ve learned that we can’t and shouldn’t do everything,” he said.
References to macroeconomic pressures mirror commentary from the company’s top brass on January 24, during J&J’s public fourth-quarter earnings call. But there was no mention then of the impending R&D rebuild.
“Looking ahead, while we expect some of the headwinds that impacted 2022 to continue, we have proven that Johnson & Johnson is resilient in times of macroeconomic challenge,” CEO Joaquin Duato said on the earnings call. “In this environment, our approach to 2023 can be best described as prudent, and our priorities for the year are clear and remain consistent.”
J&J's only publicly identified pipeline culls at the time were a phase 1 solid tumor and prostate cancer candidate, respectively. The layoffs and reduced development efforts come after the company spent nearly $15 billion on R&D in 2022, accounting for more than 15% of sales.
“Investment in R&D remains a top priority to support long-term growth and value creation,” chief financial officer Joe Wolk said on the same earnings call.
The layoffs also come after the company authorized a $5 billion share repurchasing program in September, half of which was completed before the end of 2022. And at the town hall, Fernandez jokingly recounted him, Merson and Heaton ubering around San Francisco on the company’s dime during the latest J.P. Morgan Healthcare Conference, including one trip to a “phenomenal dinner” at a Japanese steakhouse.
But the joke didn’t land with everyone, given that numerous employees were told they had lost their jobs just hours beforehand.
“You don’t want to just see a bunch of old, rich people talking about how much fun they have on company expense,” said one employee who attended the town hall.
It’s not only R&D that’s being affected by downsizing efforts. Two sources familiar with the company’s decision-making say layoffs have hit the company’s neuroscience team as well, particularly the multiple sclerosis sales team. Janssen nabbed FDA approval for Ponvory to treat relapsing MS in March 2021.
J&J has yet to unveil discrete sales figures for Ponvory, suggesting the med hasn’t met the sales threshold of—at the lowest end of J&J’s reporting—drugs like the $479 million-a-year Procrit. Ponvory’s revenues are likely lumped into J&J’s nebulous “other neuroscience” category, which reeled in a collective $1.73 billion in 2021.
The multiple sclerosis market has become increasingly competitive in recent years with the introduction of generics to Biogen's Tecfidera in 2020, plus Roche's launch of Ocrevus, which quickly scooped up market share and reached blockbuster status after just one year.
While J&J has largely kept mum on its downsizing plans, rumblings of changes afoot arose in October when Wolk offered an ever-so-subtle warning that the company was angling to “rightsize [its] infrastructure” as a two-segment company amid the separation of the consumer health business, Kenvue.
“Clearly, the macroeconomic pressures that all industries and all companies are facing is something that we have to address as well,” Wolk said of J&J’s profit margin in 2023. “While healthcare is a very, very good business and more resilient than most, it’s not as if we’re immune to some of those dynamics.”
It wasn’t immediately clear how many jobs or which functions were under threat, though Wolk told The Wall Street Journal at the time that a major restructuring wasn’t in the cards.
As of the beginning of 2022, J&J counted 141,700 full-time employees among its global staff, up from 134,500 in 2021. About a third of the company’s workforce is based in North America.
J&J typically offers an update on total headcount in its annual report, which is due in late February for 2022. The numbers will be as of January 1.
While J&J has largely stuck to the background amid a spate of job purges across the industry, the company last fall cut loose 64 employees at its Johnson & Johnson Services location in Manhattan, according to a New York state Worker Adjustment and Retraining Notification (WARN) Act notice labeled as “plant layoff.”
The business there is focused on pharmaceutical supplies, according to the filing, and the reason given for the job cuts was listed as “economic.” The workforce reduction was slated to take place over two weeks from Jan. 13, 2023 through Jan. 26, 2023.


