About 40% of American adults — some 137 million — are eligible to take the glucagon-like peptide 1 (GLP-1) receptor agonist semaglutide, said authors of a new study.
Currently, statins are the most commonly prescribed medication for American adults, with some 192 million prescriptions written in 2022, according to one estimate. The authors of a research letter published online in JAMA Cardiology estimate that at least 82 million American adults are eligible for statins.
Semaglutide will quickly overtake statins as the most prescribed pharmaceutical for American adults, said the authors. It was the top-selling drug in the United States in 2023, with sales of almost $14 billion, which made it worth taking a closer look at who might be eligible, said lead author Dhruv S. Kazi, MD, MS, associate professor of medicine at Harvard Medical School, Boston.
“We’re hoping to stimulate a transparent public conversation about the number of adults who are eligible,” Kazi told Medscape Medical News.
Kazi said it seems the United States doesn’t really have what he calls a “game plan” to ensure broad and equitable access to a high-cost, but effective medication. “If we can’t afford to treat everybody or offer the treatment to everybody,” he said, then there needs to be something like a “risk-based approach where individuals at greatest risk for adverse consequences related to either overweight or obesity or cardiovascular disease or diabetes are prioritized.”
He and his colleagues at Beth Israel Deaconess Medical Center, Boston, the Harvard T.H. Chan School of Public Health, Boston, and the Feinberg School of Medicine at Northwestern, Chicago, used data from the National Health and Nutrition Examination Survey from 2015 to 2020 to determine how many American adults might be eligible for semaglutide. They focused on diabetes, weight management, and secondary prevention of cardiovascular disease, using inclusion and exclusion criteria from major randomized clinical trials of semaglutide in those indications.
The authors report that 35 million adults are eligible for semaglutide for diabetes, 129 million for weight management, and 8.9 million for secondary cardiovascular disease prevention.
Semaglutide for secondary prevention is likely to be an area of increased growth, as there is more insurance coverage for that indication, the authors wrote.
“The numbers are staggering, but not entirely surprising,” said Beth Abramson, MD, MSc, Paul Albrechtsen Professor in Cardiac Prevention and Women’s Health in the Division of Cardiology at the University of Toronto, Toronto, Ontario, Canada. “Most of us will have many patients that would qualify for this new intervention,” she told Medscape Medical News.
The data are a “call to action” because “it gets us thinking about the issues at hand,” said Abramson, a member of the Prevention Council for the American College of Cardiology.
While millions of American adults might require these expensive medications, their use can ultimately lead to cost savings, said Abramson. Studies have shown that at high doses, semaglutide has reduced cardiovascular events, she said. “Cardiologists need to think about this when they’re seeing their patients and learn about this newer class of drugs,” Abramson said.
She also said semaglutide should only be one piece of the puzzle for patients who need help with weight management. Many patients “need help with making some healthier lifestyle choices,” said Abramson.
Kazi and his coauthors said that American policy makers and clinicians should not ignore the train that’s barreling down the tracks. “We’re going to have to figure out pricing, we’re going to have to figure out supply chains,” said Kazi. And, he said, the medical community will have to get past “the stigma of treating overweight and obesity.”
But, he said, even if clinicians become more comfortable prescribing semaglutide and other GLP-1s, “the cost issue doesn’t go away.”
“We’re going to have to have serious conversations as a society,” said Kazi.
Kazi and his coauthors reported grants outside of the work in the paper. Co-author Sadiya Khan, MD, is an associate editor of JAMA Cardiology but was not involved in any of the decisions regarding review of the manuscript or its acceptance. Abramson reported honoraria from CPD Network Association, Amgen, AstraZeneca, Bayer, BioSyent, BMS-Pfizer, Boehringer Ingelheim, CHRC, HLS Therapeutics, Novartis, Novo Nordisk, Sanofi, and Servier.
Many physicians reacted with the opposite of sympathy to the fatal shooting of UnitedHealthcare CEO Brian Thompson this week, reflecting pent-up frustration and anger over what they described as the health insurer’s routine denials of care for sick or dying patients.
The shocking killing in New York City sparked a wave of antipathy from doctors and patients for the nation’s largest health insurer, which Thompson had led since 2021. UnitedHealthcare, a division of the conglomerate UnitedHealth Group, insures about 50 million Americans and reported more than $281 billion in revenue in 2023. Thompson received compensation of more than $10 million in 2023.
“I’m waiting for a prior authorization before I shed any tears,” wrote Reddit user KR1735, listed as an internal medicine doctor, on the subreddit r/medicine.
One physician online recalled fighting with UnitedHealthcare over its denial of the low-cost drug metformin. Another recalled the insurer requiring a peer-to-peer review for prescribing levodopa, “a drug so old it could join the AARP. The ‘peer’ I spoke with had never heard of Sinemet, Parkinson’s, or the FDA,” a Reddit user describing himself as a neurologist wrote.
Particularly on Reddit, comments were so scathing that the moderators of the leading medical subreddit deleted one thread about Thompson’s slaying, the Daily Beast reported. But clinicians’ harsh criticism of the CEO and UnitedHealthcare’s practices continued throughout the week on Reddit and other social media platforms.
“If you’re the CEO of one of the most comically evil companies in the US, you should be prepared for consequences, and the only surprise should be that this doesn’t happen more often…the fact no one is sad speaks to the legacy left behind; hope the millions were worth it,” wrote Reddit user ThucydidesButthurt, listed as an anesthesiologist, on a separate thread on r/medicine.
A few physicians took a more measured approach.
“While the murder of the UnitedHealthcare CEO is tragic, let’s remember that thousands of Americans die every year when United denies coverage. Violence is never the answer, but we do need to find lawful ways to hold insurance executives accountable for their greed,” wrote Bluesky user “Lisa, MD,” on the social media platform.
‘Deny’ and ‘Defend’
The words “deny,” “defend,” and “depose” were seen on shell casings at the crime scene, police said, echoing words used to describe how health insurers “delay,” “deny,” and “defend” to avoid paying for care in hopes of increasing profits. It’s even the title of a 2010 book on the insurance industry.
UnitedHealthcare used algorithms to improperly deny mental health claims, a system three states deemed illegal, ProPublica reported. A STAT investigation found the insurer similarly used algorithms to deny rehabilitation care for its Medicare Advantage enrollees.
Earlier this year, an employee pension fund in Florida sued Thompson, UnitedHealth Group, and two other executives for alleged fraud and illegal insider trading, claiming that the executives did not disclose a federal antitrust investigation of the company, CNN reported.
While some physicians pointed to a chart showing that UnitedHealthcare denied nearly a third of all claims, more than other US insurers, comparing denial rates among insurers is challenging because insurers are largely not required to report them. Insurers offering Affordable Care Act plans on state exchanges are required to report claim denials for those plans to federal officials.
“What has bothered me the most is people that put fiduciary responsibility (eg, profits) above human lives, none more so than this company as run by him,” wrote one Reddit user who identified himself as an MD otolaryngology professor. “When other’s (sic) human lives are deemed worthless, it is not surprising to have others view your life of no value as well.”
They’re literally not better. Idealistically, sure, but literally not. And there’s really no debate. Meaning there’s never been a reproducible diet and exercise intervention that has led to anywhere near the average weight lost by those takingobesitymedications. Furthermore, when it comes to the durability of weight lost, the gulf between outcomes with diet and exercise vs obesity medications is even more dramatic.
Looking to the literature, one of the most trotted out studies on lifestyle’s impact on weight over time is the Look AHEAD trial. Before useful obesity medications came on the scene, I trotted it out myself. Why? Because it was heartening when faced with the societal refrain that diet and exercise never worked to be able to show that yes, in fact they do. But how well?
Now maybe you want to cling to the notion that if you just try hard enough, your diet and exercise regime can beat our new meds. Well, it’s difficult to think of a more miserable, often actual vomit-inducing intervention, than the spectacle that used to air weekly on prime time called The Biggest Loser, where participants lived on a ranch and were berated and exercised all day long for the chance to lose the most and win a quarter of a million dollars. But even there, the meds prove to be superior. Although the short-term Biggest Loser data do look markedly better than meds (and than bariatric surgery), whereby the average participant lost 48.8% of their body weight during the grueling 7-month long, 24/7 competition, by postcompetition year 6, the average weight lost dropped to 12.7%.
The only reason that the world isn’t comfortable with the eminently provable truth that diet and exercise are inferior to obesity medications for weight management is weight bias. The message is that people simply aren’t trying hard enough. This despite our comfort in knowing that medications have more of an impact than lifestyle on pretty much every other chronic disease. Nor can I recall any other circumstance when coverage of a remarkably effective drug was qualified by the suggestion that known-to-be-inferior interventions are still the best or favored choice.
At this point, obesity medications are plainly the first line choice of treatment. They provide not only dramatically greater and more durable weight loss than lifestyle interventions, they have also been shown to very significantly reduce the risk for an ever-growing list of other medical concerns including heart attacks, strokes, type 2 diabetes, hypertension, sleep apnea, fatty liver disease, and more, while carrying minimal risk.
Let it also be said that improvements to diet and exercise are worth striving for at any weight, though one should not lose sight of the fact that perpetual, dramatic, intentional, behavior change in the name of health requires vast amounts of wide-ranging privilege to enact — amounts far beyond the average person’s abilities or physiologies (as demonstrated with obesity by decades of disappointing long-term lifestyle outcome data).
Let it also be said that some people will indeed find success solely through lifestyle and that not every person who meets the medical criteria for any medication’s prescription, including obesity medications, is required or encouraged to take it. The clinician’s job, however, at its most basic, is to inform patients who meet medical use criteria of their options, and if a medication is indicated, to inform them of that medication’s risks and benefits and expected outcomes, to help their patients come to their own treatment decisions.
It’s not a bad thing that we have medications that deliver better outcomes than lifestyle — in fact, it’s terrific, and thankfully that they do is true for pretty much every medical condition for which we have medication. That’s in fact why we have medications! And so this constant refrain of golly-gee wouldn’t it be better if we could just manage obesity with lifestyle changes needs to be put to rest — we literally know it wouldn’t be better, and it’s only weight bias that would lead this evidence-based statement to seem off-putting.
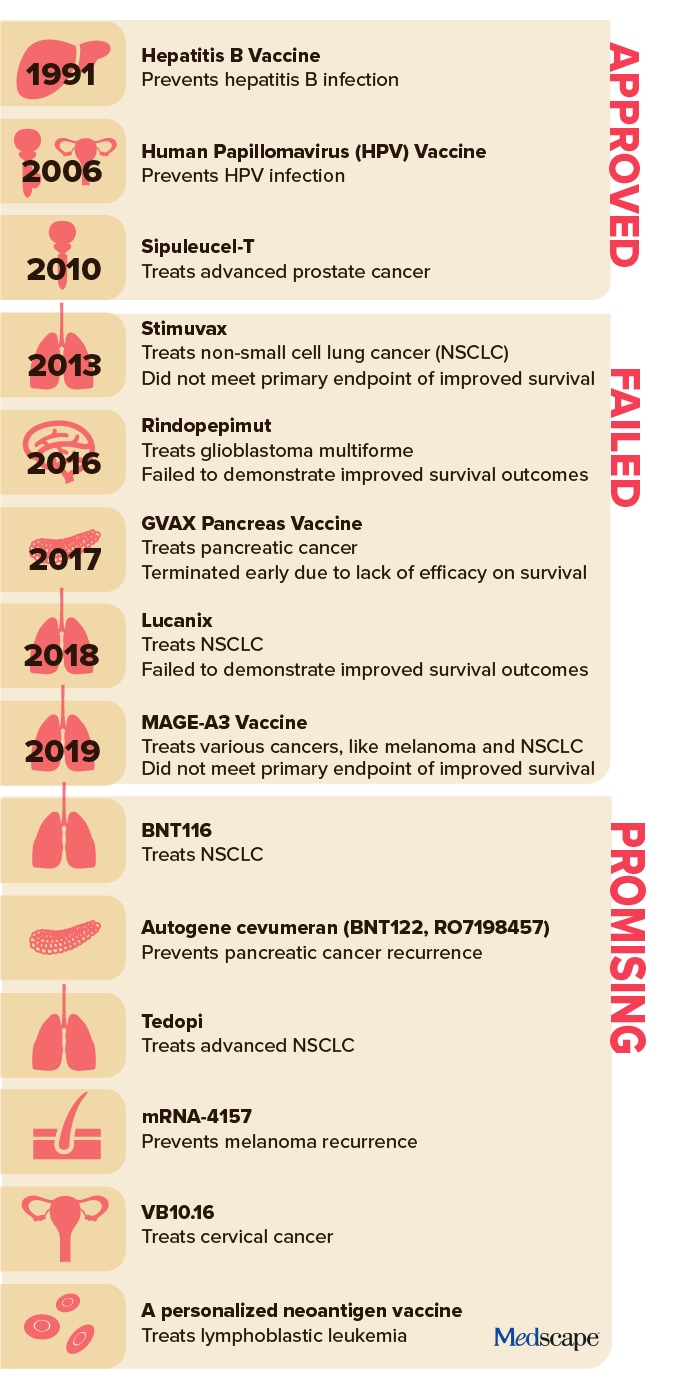
Vaccines for treating and preventing cancer have long been considered a holy grail in oncology.
But aside from a few notable exceptions — including the human papillomavirus (HPV) vaccine, which has dramatically reduced the incidence of HPV-related cancers, and a Bacillus Calmette-Guerin vaccine, which helps prevent early-stage bladder cancer recurrence — most have failed to deliver.
Following a string of disappointments over the past decade, recent advances in the immunotherapy space are bringing renewed hope for progress.
In an American Association for Cancer Research (AACR) series earlier this year, Catherine J. Wu, MD, predicted big strides for cancer vaccines, especially for personalized vaccines that target patient-specific neoantigens — the proteins that form on cancer cells — as well as vaccines that can treat diverse tumor types.
“A focus on neoantigens that arise from driver mutations in different tumor types could allow us to make progress in creating off-the-shelf vaccines,” said Wu, the Lavine Family Chair of Preventative Cancer Therapies at Dana-Farber Cancer Institute and a professor of medicine at Harvard Medical School, both in Boston.
A prime example is a personalized, messenger RNA (mRNA)–based vaccine designed to prevent melanoma recurrence. The mRNA-4157 vaccine encodes up to 34 different patient-specific neoantigens.
“This is one of the most exciting developments in modern cancer therapy,” said Lawrence Young, a virologist and professor of molecular oncology at The University of Warwick, Coventry, England, who commented on the investigational vaccine via the UK-based Science Media Centre.
Other promising options are on the horizon as well. In August, BioNTech announced a phase 1 global trial to study BNT116 — a vaccine to treat non–small cell lung cancer (NSCLC). BNT116, like mRNA-4157, targets specific antigens in the lung cancer cells.
“This technology is the next big phase of cancer treatment,” Siow Ming Lee, MD, a consultant medical oncologist at University College London Hospitals, which is leading the UK trial for the lung cancer and melanoma vaccines, told The Guardian. “We are now entering this very exciting new era of mRNA-based immunotherapy clinical trials to investigate the treatment of lung cancer.”
Still, these predictions have a familiar ring. While the prospects are exciting, delivering on them is another story. There are simply no guarantees these strategies will work as hoped.
Then: Where We Were
Cancer vaccine research began to ramp up in the 2000s, and in 2006, the first-generation HPV vaccine, Gardasil, was approved. Gardasil prevents infection from four strains of HPV that cause about 80% of cervical cancer cases.
In 2010, the US Food and Drug Administration approved sipuleucel-T, the first therapeutic cancer vaccine, which improved overall survival in patients with hormone-refractory prostate cancer.
Researchers predicted this approval would “pave the way for developing innovative, next generation of vaccines with enhanced antitumor potency.”
In a 2015 AACR research forecast report, Drew Pardoll, MD, PhD, co-director of the Cancer Immunology and Hematopoiesis Program at Johns Hopkins University, Baltimore, said that “we can expect to see encouraging results from studies using cancer vaccines.”
Despite the excitement surrounding cancer vaccines alongside a few successes, the next decade brought a longer string of late-phase disappointments.
In 2016, the phase 3 ACT IV trial of a therapeutic vaccine to treat glioblastoma multiforme (CDX-110) was terminated after it failed to demonstrate improved survival.
That year, an attenuated Listeria monocytogenes vaccine to treat pancreatic cancer and mesothelioma also failed to come to fruition. In late 2017, concerns over listeria infections prompted Aduro Biotech, Inc. to cancel its listeria-based cancer treatment program.
In 2018, a phase 3 trial of belagenpumatucel-L, a therapeutic NSCLC vaccine, failed to demonstrate a significant improvement in survival and further study was discontinued.
And in 2019, a vaccine targeting MAGE-A3, a cancer-testis antigen present in multiple tumor types, failed to meet endpoints for improved survival in a phase 3 trial, leading to discontinuation of the vaccine program.
But these disappointments and failures are normal parts of medical research and drug development and have allowed for incremental advances that helped fuel renewed interest and hope for cancer vaccines, when the timing was right, explained vaccine pioneer Larry W. Kwak, MD, PhD, deputy director of the Comprehensive Cancer Center at City of Hope, Duarte, California.
When it comes to vaccine progress, timing makes a difference. In 2011, Kwak and his colleagues published promising phase 3 trial results on a personalized vaccine. The vaccine was a patient-specific tumor-derived antigen for patients with follicular lymphoma in their first remission following chemotherapy. Patients who received the vaccine demonstrated significantly longer disease-free survival.
But, at the time, personalized vaccines faced strong headwinds due, largely, to high costs, and commercial interest failed to materialize. “That’s been the major hurdle for a long time,” said Kwak.
Now, however, interest has returned alongside advances in technology and research. The big shift has been the emergence of lower-cost rapid-production mRNA and DNA platforms and a better understanding of how vaccines and potent immune stimulants, like checkpoint inhibitors, can work together to improve outcomes, he explained.
“The timing wasn’t right” back then, Kwak noted. “Now, it’s a different environment and a different time.”
A Turning Point?
Indeed, a decade later, cancer vaccine development appears to be headed in a more promising direction.
Among key cancer vaccines to watch is the mRNA-4157 vaccine, developed by Merck and Moderna, designed to prevent melanoma recurrence. In a recent phase 2 study, patients receiving the mRNA-4157 vaccine alongside pembrolizumab had nearly half the risk for melanoma recurrence or death at 3 years compared with those receiving pembrolizumab alone. Investigators are now evaluating the vaccine in a global phase 3 study in patients with high-risk, stage IIB to IV melanoma following surgery.
Another one to watch is the BNT116 NSCLC vaccine from BioNTech. This vaccine presents the immune system with NSCLC tumor markers to encourage the body to fight cancer cells expressing those markers while ignoring healthy cells. BioNTech also launched a global clinical trial for its vaccine this year.
Other notables include a pancreatic cancer mRNA vaccine, which has shown promising early results in a small trial of 16 patients. Of 16 patients who received the vaccine alongside chemotherapy and after surgery and immunotherapy, eight responded. Of these eight, six remained recurrence free at 3 years. Investigators noted that the vaccine appeared to stimulate a durable T-cell response in patients who responded.
Kwak has also continued his work on lymphoma vaccines. In August, his team published promising first-in-human data on the use of personalized neoantigen vaccines as an early intervention in untreated patients with lymphoplasmacytic lymphoma. Among nine asymptomatic patients who received the vaccine, all achieved stable disease or better, with no dose-limiting toxicities. One patient had a minor response, and the median time to progression was greater than 72 months.
“The current setting is more for advanced disease,” Kwak explained. “It’s a tougher task, but combined with checkpoint blockade, it may be potent enough to work.”
Still, caution is important. Despite early promise, it’s too soon to tell which, if any, of these investigational vaccines will pan out in the long run. Like investigational drugs, cancer vaccines may show big promising initially but then fail in larger trials.
One key to success, according to Kwak, is to design trials so that even negative results will inform next steps.
But, he noted, failures in large clinical trials will “put a chilling effect on cancer vaccine research again.”
“That’s what keeps me up at night,” he said. “We know the science is fundamentally sound and we have seen glimpses over decades of research that cancer vaccines can work, so it’s really just a matter of tweaking things to optimize trial design.”
Companies tend to design trials to test if a vaccine works or not, without trying to understand why, he said.
“What we need to do is design those so that we can learn from negative results,” he said. That’s what he and his colleagues attempted to do in their recent trial. “We didn’t just look at clinical results; we’re interrogating the actual tumor environment to understand what worked and didn’t and how to tweak that for the next trial.”
Kwak and his colleagues found, for instance, that the vaccine had a greater effect on B-cell–derived tumor cells than on cells of plasma origin, so “the most rational design for the next iteration is to combine the vaccine with agents that work directly against plasma cells,” he explained.
As for what’s next, Kwak said: “We’re just focused on trying to do good science and understand. We’ve seen glimpses of success. That’s where we are.”
Syria is just the latest case of U.S. meddling and the timing could not be more suspicious...
The Biden administration has triggered another proxy war for Donald Trump to deal with when he becomes president next month.
The U.S. deep state is fighting a proxy war in Syria, which appears to be waged with the intention of further destabilizing the Middle East and stirring up another front in World War III.
Syria is collapsing under the weight of another U.S.-sponsored proxy Civil War, with the US, Israel and Sunni jihadists on one side and Russia, Iran, Assad, and Shiite jihadists on the other.
Al Nusra (which is comprised of Al-Qaida and ISIS affiliates) is taking over the country with the help of Turkey, a U.S. ally and key member of the NATO military alliance. These rebels have seized the city of Aleppo and many smaller towns and villages.
Jake Sullivan is Biden’s national security adviser and a key enabler, along with Secretary of State Antony Blinken, of the anti-Russia obsessed deep-state club that shares one thing in common. They all belong to the Trilateral Commission and the Council on Foreign Relations.
Dowling notes that Syria’s civil war started in 2011 after an uprising against President Bashar Assad’s rule. The U.S., Russia, Israel and Iran all have a military presence in Syria. Forces opposed to Assad, along with U.S.-backed rebels, control more than a third of the country and now Russia and Iran have launched a counter-offensive. Russia is very upset with Turkey for instigating the coup against Assad, likely with the direct assistance of the CIA.
The false narrative being proffered by the US mockingbird media is that a rag-tag coalition of so-called “noble rebels” has somehow organically emerged to save Syria from the dictator Assad. No, what we have here are Sunni jihadists backed by the U.S. and NATO fighting Shia jihadists backed by Russia.
As Dowling points out, “All jihadists are bad guys.” They are bad because as soon as they get in power one of the first things they do is start raping the Christian women and executing the Christian men. It happened in Iraq after Saddam Hussein was overthrown and it’s happening now in Syria.
Congress funded jihadist rebels in Syria for years. The chief war whores of the military-industrial complex, Senators Lindsey Graham and John McCain, led the way.
Dowling quotes Joe Kent, a former chief warrant officer in the U.S. Army special forces, saying that the U.S. is “in an endless cycle of violence” and a “regime-change war” in Syria that the US has pushed.
The world is aflame and the regime in Washington appears to be dowsing it with gasoline in anticipation of handing the chaos over to Donald Trump to deal with as the 47th president.
Dowling ends her article with this truth bomb:
“We need to be out of Syria. We’re helping no one, certainly not Americans. This is another spear in World War III.”
The U.S. is also stirring the pot in the Eastern European country of Georgia, where protesters continue to be out in the streets. The U.S. is complicit in the deaths of more than half a million Ukrainians.
I would say we need to be out of every country in the world where there is no direct compelling national interest for America’s national security. Rein in the CIA and limit its actions strictly to intelligence gathering (no more fomenting of revolutions and coups) bring our boys home and return the concept of “defense” to our U.S. Department of Defense.
Decision follows observations of liver transaminitis without clinically significant symptoms in some subjects on azelaprag
Company will evaluate data from patients enrolled to date and share updated plans for azelaprag in Q1 2025
In parallel to evaluating azelaprag, Company will continue to advance earlier platform-derived programs, including IND submission for CNS penetrant NLRP3 inhibitor anticipated in the second half of 2025
The House task force assembled to review the assassination attempts on President-elect Trump’s life held its final meeting on Thursday, grilling the acting Secret Service director before voting to soon release their final report.
It was a meeting that stressed the bipartisan push for reform at the Secret Service, but that sentiment was overshadowed by a tense exchange between Ronald Rowe, the agency’s acting leader, and Rep. Pat Fallon (R-Texas) over the director’s presence at a 9/11 event.
Rowe called the agency’s performance at the first shooting an “abject failure” — one that resulted in the death of one man and the critical wounding of two others in addition to a bullet striking Trump’s ear.
“I personally carry the weight of knowing that we almost lost a protectee and that our failure cost a father and husband his life. This entire incident represents the failure to meet the expectations and responsibilities of the Secret Service,” Rowe said in an opening statement, referencing the shooting in Butler, Pa.
But he and task force Chair Mike Kelly (R-Pa.) saw the second shooting in September as a different story, given agents’ ability to foil the planned attack from shooter Ryan Wesley Routh before Trump entered his line of sight on the president-elect’s Florida golf course.
“Secret Service security redundancies, while not flawless, got the job done,” Kelly said, referring to the multiple layers of protection used that day.
It was a reflective hearing, one in which Rowe continued to be critical of the agency he has led since former Director Kimberly Cheatle stepped down after a disastrous appearance before the House, where she was lambasted by members on both sides of the aisle for failing to answer basic questions about what happened.
The Secret Service has already completed its own internal review of the attack, one that blamed a culture of complacency in the agency and a failure to account for the real risks to its protectees as well as planning and communications lapses.
In responding to a question from Kelly about what he considered the agency’s biggest mistake on July 13, Rowe pointed to the failure to secure the building from which shooter Thomas Matthew Crooks fired shots and to “recognize its significance” in the security setting.
“That to me is glaring, and those are basic tenets — fundamental — of what an advance team is supposed to identify risks and mitigate risks,” Rowe said.
“We did not do that on the 13th.”
But the agency’s tech issues were also a major focus of the hearing, given that agents and local law enforcement assisting in Butler were unable to communicate over the same radio system.
“It’s just wild to me that in 2024, our nation’s premier law enforcement agency, on July 13, was using text messages on their personal cellphones, literally sending emails in some cases, to deliver relevant information and scribbling messages on paper and not using a system,” said ranking member Jason Crow (D-Colo.).
He described a new system that has been implemented “in part” but asked if the agency was considering more advanced systems used by the military.
Rowe said the agency already does this for major events like the Super Bowl and others designated as “national special security events.”
“We should be able to do this, and we can do this on a smaller scale,” Rowe said.
Not all were focused on communications issues, however, with Rep. Mark Green (R-Tenn.) arguing his colleagues have been too focused on technology.
“The lack of attention to detail, lack of sense of urgency, complacency. These are leadership issues. These are command leadership issues,” he said.
“That’s the thing that concerns me the most.”
Rowe has said he wants to end the “doing more with less” culture within the agency, something he has said is “not consistent with achieving a no-fail mission” but also requires more funding.
Tensions flared at the end of the hearing when Fallon asked Rowe about his attendance at a 9/11 event, showing a photo in which Rowe is positioned next to President Biden. Fallon alleged that Rowe bumped protective agents from being in a prime position for the event.
The acting director erupted in anger, saying the protective detail was just outside the frame of the photo.
“That is the day where we remember the more than 3,000 people that died on 9/11. I actually responded to ground zero. I was there, going through the ashes of the World Trade Center,” he said, telling Fallon he was at the memorial to “show respect” for a Secret Service agent who died in the attack.
“Do not invoke 9/11 for political purposes,” Rowe shouted at Fallon.