This week, I want to talk about longevity science.
It’s a field that has exploded online, fueling the dramatic expansion of an already booming wellness industry. I have been digging into the data behind wellness and longevity for a new podcast, and the deeper I go, the clearer it becomes that the field has a couple of fundamental problems.
The first is the problem of observational data. People want to know something simple: If I take this supplement, or eat this food, or do this exercise, or take this medication consistently for years, will I live longer and better? But in the observational framework, we run into a major problem because, to put it simply, people who eat kale on the regular are fundamentally different in many ways from people who don't eat kale on the regular. This is known as the "healthy user effect" and it makes it incredibly difficult to tease out the specific benefits of anything you want to put in or do to your body.
That leaves randomized trial data, the gold standard of medical research in which an intervention is assigned at random to a group of people: Some of you get kale and some of you get old-fashioned iceberg lettuce. The problem is that conducting these trials is expensive and few people are interested in funding them. The National Institutes of Health have always focused on the diagnosis and treatment of disease, not necessarily on increasing health span. That's not entirely irrational because, to be fair, studies of people with an underlying disease are way easier to conduct. The outcomes of those studies happen in a relatively short time window from the start of the study. Whether the outcome we’re talking about is cure of the disease or avoidance of a major complication of the disease, either way, you're dealing with things that can occur on a typical 5-year grant cycle.
When it comes to big questions like, should I, a 46-year-old, take this vitamin for the rest of my life to see if it leads to a longer, healthier life when I'm 80? Well, a randomized trial spanning 30 or 40 years is simply infeasible.
But there's a bit of an asterisk here, and it's an asterisk that's going to come into play in a study that came across my desk this week. Because if the effect of an intervention lasts, maybe we can take a randomized trial that happened long ago, track down all the people that participated, and see if 20 years later, there are still lingering effects. Today, we have such a study. And it concerns metformin, the old-school diabetes drug that has somehow become the darling of the biohacking crowd.
Decades ago, a large randomized trial pitted metformin against lifestyle change in people with prediabetes. And this week, in JAMA, we finally get to see which group went on to live the longer, healthier life.
To understand it, I have to take you back to where it began. Pass your mind to the heady days of 2002: Kelly Clarkson just won the first season of American Idol, and Lord of the Rings: The Two Towers blew up the box office.
Back then, the Diabetes Prevention Program trial (the DPP) was published. The researchers had recruited more than 3200 people with prediabetes, defined by conventional criteria: a mildly elevated fasting glucose (in the range of 95-125 mg/dL) plus impaired glucose tolerance on a glucose-tolerance test (a 2-hour value of 140-199 mg/dL) in people carrying some extra weight. At enrollment, the average participant was about 51 years old, roughly two thirds were women, and the cohort was relatively diverse; about 44% came from racial and ethnic minority groups.
Participants were randomly assigned into one of three arms. The first was an intensive lifestyle intervention, with three goals: Lose at least 7% of body weight, keep fat below 25% of calories, and get at least 150 minutes of physical activity a week. The second arm got metformin, titrated up to 850 mg twice a day. And the third, the control group, got a placebo pill.
I will get to the original results in a moment, but first, a word about why metformin is the belle of the biohacker ball. There is actually some biology here. Metformin activates an enzyme called AMPK and, in doing so, increases mitochondrial biogenesis. Some nice studies of worms and fruit flies have shown that metformin can increase lifespan. Moving up to mammals, studies in mice have been beneficial, but results were more mixed when the mice had a more heterogeneous genetic background. Nevertheless, these promising findings, as well as the fact that metformin has beneficial effects on liver fat and other metabolic factors, have led some people without diabetes and even without prediabetes to start taking the drug. But in 2002, the question was far more grounded: Could metformin, the frontline therapy for incident type 2 diabetes, delay the onset of diabetes in high-risk people?
Did it work? It did. Over about 3 years, metformin reduced the risk for progression to type 2 diabetes by 31% compared to placebo. Interestingly, that lifestyle-modification intervention reduced the risk for progression by 58%. Lifestyle beat the drug, but both beat nothing. That result was practice-changing, but it is not what we are here to talk about today.
At the end of the randomized period of the trial, the DPP converted into an observational study. The people in the metformin arm continued to take metformin, open label now, so they knew what they were getting. They also got some lifestyle intervention. The people in the lifestyle-intervention arm got the same lifestyle intervention, plus the opportunity to take some lifestyle booster courses every 6 months — so, sort of an optional recharge of your healthier lifestyle. This phase of the study went on for 20 years.
What's really clever about what was published in JAMA this week is that the researchers linked all of these patients to their Medicare records. Many of them are now above age 65, and so we can get access to exactly what has happened years and decades after they participated in this trial.
The question then becomes, what do you look for? What outcome, decades after this trial, would tell you that metformin or lifestyle intervention — or both or neither — has a meaningful effect on health span? The researchers settled on a concept called multimorbidity. Multimorbidity is the co-occurrence of two or more chronic disease diagnoses — say, diabetes and hypertension, or stroke and kidney disease.
Why multimorbidity?
You could, of course, study each individual comorbidity on its own. In fact, there have been studies of this same population and the rates of cancer and heart disease, but if we're really getting at healthspan, we have to appreciate a phenomenon that happens as we age: an accelerating accumulation of chronic diseases, a set of dominoes that start to fall.
This is the phenomenon that actually defines aging: an accelerating accumulation of chronic illness. And there is good evidence that crossing into multimorbidity is a meaningful threshold. You stop being a person managing one problem and become a person juggling several. More medications, more appointments, more exposure to the healthcare system, and it tends to forecast still more diagnoses to come. So the question here is not really “How long do you stay in perfect health?” It is closer to “How long do you stay free from the beginning of the end?” I am not sure it is a perfect outcome. But it is a very interesting one.
So, let’s look at the numbers.
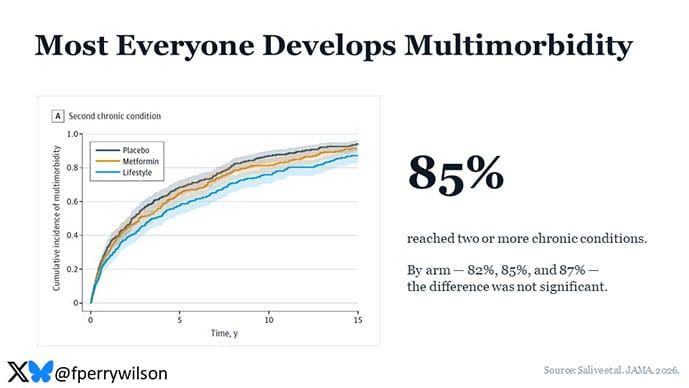
Given the long follow-up and the elevated baseline risk of this prediabetic population, most people developed multimorbidity eventually; 85% of the cohort accumulated two or more chronic conditions. And when you look at the raw, unadjusted rates by group — 82% in lifestyle, 85% in metformin, 87% in placebo — the differences are not statistically significant.
Let’s pause there because I know what you are thinking: Does that mean none of this worked? Maybe. Or maybe it is because these interventions ended two decades ago, and people backslide. The metformin folks stop their metformin, the lifestyle folks drift back to old habits. The authors give us some data on that. There is backsliding, but a meaningful share of people stuck with their original assignment. The metformin group, for instance, kept taking metformin for a median of 18 of those 21 years. Call it the force of habit.
And the picture sharpens when you adjust for baseline differences and dig a little deeper. In the primary, covariate-adjusted analysis, the lifestyle group had a significantly lower risk for multimorbidity compared with placebo: a hazard ratio of 0.79. Metformin showed no such benefit: 0.91, and not significant.
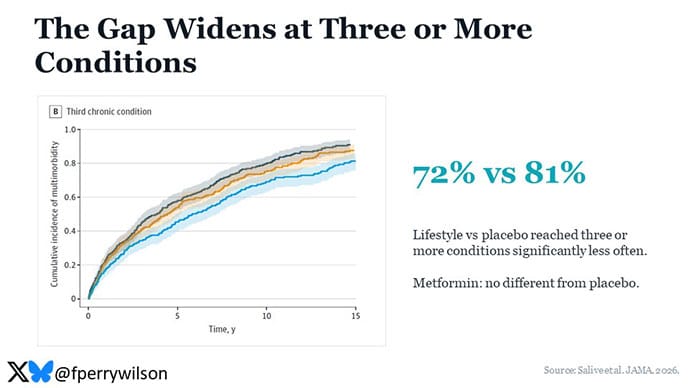
The results get more interesting when we drill down a bit deeper. When we look at the co-occurrence of three or more comorbidities, something that happens less frequently in the dataset, lifestyle interventions significantly improved the outcome vs placebo whereas metformin did not.
We can also treat the number of comorbidities as a count outcome instead of a binary. When the authors examined the data that way, they found that the lifestyle intervention led to, on average, 10% less total comorbidities over time than placebo whereas metformin had no effect. When the authors restricted the outcome to a set of highly costly comorbid dyads, the effect was more stark. Lifestyle cut the risk by 43% and metformin had no effect.
Now, I know I said this is a study about multimorbidity, but of course I couldn't help myself and I looked at some individual outcomes. And I must say, by far the most surprising one was the incidence of type 2 diabetes. If metformin were going to do anything here, surely it would be to prevent diabetes. Yet, the proportion who went on to develop diabetes was lowest in the lifestyle group, 60%, vs 69% in placebo and 71% in metformin.
Together, these data suggest something that I think we all feel and resonate with but often lack the data to describe, which is that lifestyle interventions can be incredibly powerful and incredibly long-lasting.
Building habits leads to persistence of those habits over time, leading to a real change in health. A medication, even one as amazing as metformin, does not have that same effect.
I'd be remiss not to suggest that there's some possibility of biology here. Metformin is not a panacea. In fact, some studies have shown that metformin use blunts the effects of some lifestyle interventions, like exercise. Studies have suggested, for example, that metformin use decreases the improvement in VO2 max among people doing cardiorespiratory fitness training. So it's conceivable that the reason you're not seeing much effect of metformin vs placebo is not that it doesn't do anything at all, but that it has a mix of both beneficial and unbeneficial effects, and they tend to cancel each other out. Figuring out exactly what's going on there might lead to interventions that make metformin work better. But in the end, I see this study as a strong endorsement of the fact that to truly change the outcomes of our lives, we have to change ourselves in ways that are more fundamental than remembering to take a pill twice a day.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator.
https://www.medscape.com/viewarticle/what-beats-biohacking-drug-metformin-healthy-aging-2026a1000k5p
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.