by Maryanne Demasi via The Brownstone Institute,
In a recent interview, famed astrophysicist Neil deGrasse Tyson was challenged on his scientific views about COVID-19 and he said “I’m only interested in consensus” – words that would have Nicholas Copernicus and Galileo Galilei rolling in their graves.
The appeal to “scientific consensus” is fraught with problems, just like “The science is settled” and “Trust the science” and other authoritarian tropes that have dominated the pandemic.
A widely accepted theory, such as the theory of evolution, depends on a consensus being reached among the scientific community, but it must be achieved without censorship or reprisal.
As Aaron Kheriaty, a fellow at the Ethics and Public Policy Center, recently said:
Science is an ongoing search for truth & such truth has little to do with consensus. Every major scientific advance involves challenges to a consensus. Those who defend scientific consensus rather than specific experimental findings are not defending science but partisanship.
Consensus by Censorship
It’s not difficult to reach a scientific consensus when you squelch dissenting voices.
The origin of COVID is a classic example. Twenty-seven scientists published a letter in the Lancet condemning “conspiracy theories” that suggested the virus did not have a natural origin. Dissenting views were censored on social media and labelled “misinformation.”
It’s only now that the US Department of Energy and the FBI say the virus was likely the result of a lab leak in Wuhan, that it’s possible to have these discussions openly.
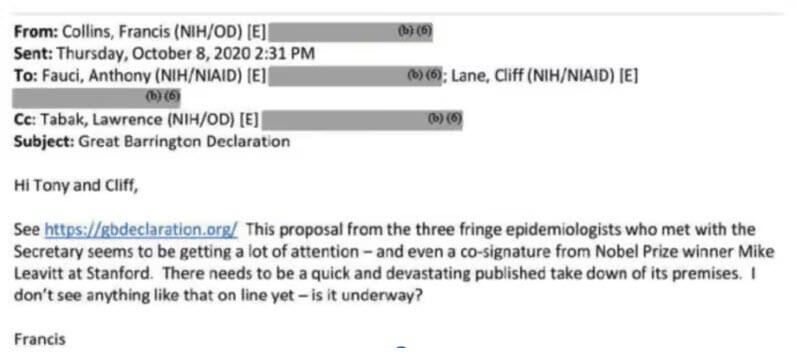
The Great Barrington Declaration is another example. Three eminent professors from Harvard, Stanford, and Oxford Universities, argued against lockdowns, which they said would disproportionately harm the underprivileged.
But former NIH director Francis Collins dismissed them as “fringe epidemiologists” asking Anthony Fauci for “a quick and devastating take down” of the declaration.
Scientific consensus has become a manufactured construct, dictated by politics and power.
The recent release of the ‘Twitter Files’ reveals how government agencies, Big Tech, media, and academia colluded in an effort to police online content, and censor dissenting voices to create a false perception of consensus.
One egregious example was Stanford University’s Virality Project that brought together elite academia, experts in artificial intelligence, and social media companies to censor “true” stories of vaccine injuries under the guise of fighting disinformation.
Robert Malone, physician and pioneer of mRNA technology summed up the situation accurately when he said;
“The real problem here is the damn press and the internet giants. The press and these tech players act to manufacture and reinforce “consensus” around selected and approved narratives. And then this is being weaponized to attack dissenters including highly qualified physicians.”
The pandemic has made this insidious behaviour more visible, but the reality is, it has been happening for a long time – I would know – I was caught up in it.
Consensus in mainstream media
As a TV presenter on ABC’s top ranking science program Catalyst for over a decade, my role was to investigate science issues and, if necessary, challenge orthodoxy.
The ABC is not funded by private industry, but by the public purse, to avoid the bias which befalls the commercial networks. Or so I thought.
Several years ago, my successful career at the ABC came to a grinding halt after defenders of “scientific consensus” criticised several documentaries I produced, which questioned various medical orthodoxies such as cholesterol-lowering drugs, nutritional guidelines, and the over-prescription of medicines.
One documentary questioned the health impacts of prolonged exposure to wireless devices (such as iPads, laptops, and smartphones) which emit low frequency radiation – we did our due diligence and undertook an excruciating process of reviewing the program for legal, editorial, and factual integrity.
In the program, we questioned why the Australian government’s radiation safety authority (ARPANSA) had safety standards that were out-of-date, and excluded important evidence from multiple peer-reviewed papers by independent scientists.
It unleashed a firestorm of complaints from the Telco industry, the regulatory authority and ARPANSA, all of which had been preparing for the biggest wireless rollout the country had ever seen.
Industry experts emerged from the shadows, and the media obliged, uncritically reporting criticisms of the program, while ignoring those defending it. No attention was paid to industry’s influence over the science.
Critics complained that I’d given weight to a “fringe” position that was not supported by science. And by “fringe” they were referring to Devra Davis, professor of epidemiology at the University of Pittsburgh, with a distinguished career at the National Academy of Sciences, and the National Research Council.
The ABC caved to the relentless pressure and suspended me from on-air duties, concluding that I’d given prominence “to views challenging the scientific consensus.”
And by “scientific consensus,” they meant the position taken by ARPANSA, the very organisation I had criticised for its lax regulations.
Eventually, the ABC banned the program and “restructured” the department by firing the staff. What the network believed would be a quick solution had serious and far-reaching consequences.
It would not only deter future journalists from questioning orthodoxy, but it sent a chilling message that the ABC would succumb to industry pressure and favour scientific consensus.
I think Michael Crichton – physician, producer, and writer – explained it best when he gave a lecture on science, politics, and consensus in 2003;
I regard consensus science as an extremely pernicious development that ought to be stopped cold in its tracks. Historically, the claim of consensus has been the first refuge of scoundrels; it is a way to avoid debate by claiming that the matter is already settled.
He continued:
Consensus is the business of politics….The greatest scientists in history are great precisely because they broke with the consensus. There is no such thing as consensus science. If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.
https://www.zerohedge.com/technology/scientific-consensus-manufactured-construct
